
Abstract
Introduction
Laboratory comments appended on clinical biochemistry reports are common in the UK. Although popular with clinicians and the public, there is little evidence that these comments influence the clinical management of patients.
Methods
We provided reflex automated laboratory comments on all primary care lipid results including, if appropriate, recommendation of direct referral to the West Midlands Familial Hypercholesterolaemia service (WMFHS). Over a two-year period, the number GP referrals from the Wolverhampton City Clinical Commissioning Group (CCG) to the WMFHS were compared with four comparator CCGs of similar population size, who were not provided with reflex laboratory comments.
Results
Over the study period, the WMFHS received more referrals from Wolverhampton GPs (241) than any other comparator CCG (range 8–65) and greater than the combined referrals (172) from all four comparator CCGs.
Conclusion
Targeted reflex laboratory comments may influence the clinical management of patients and may have a role in the identification of individuals with familial hypercholesterolaemia.
Introduction
Familial hypercholesterolaemia (FH), a disorder of lipoprotein metabolism characterized by raised circulating concentrations of LDL cholesterol, carries an increased risk of premature atherosclerotic cardiovascular disease (CVD).1–3 Early detection and treatment of FH are important, since lipid-lowering therapy is highly effective and gives the same life expectancy as the general population. 4 Subsequent cascade testing to identify relatives of people with FH is also highly cost-effective. 4 People with FH, however, are commonly undiagnosed and are therefore untreated. 4
In March 2017, the West Midlands Regional Familial Hypercholesterolaemia Service (WMFHS), the first region-wide screening service in the England, was launched with extensive primary care promotion by the WMFHS of the service similarly across all clinical commissioning groups (CCGs) within the West Midlands. From December 2017, we provided automated rule-based comments on all general practitioner (GP) lipid results specific for primary or secondary CVD prevention based on National Institute for Health and Care Excellence (NICE) clinical guidance (CG): NICE CG071 and NICE CG1815,6 and the WMFHS guidelines. These comments included, if appropriate, recommendations for direct GP referral to WMFHS service.
The addition of comments onto clinical biochemistry reports is widespread in the UK, but there is scant evidence that they influence the patient management.7,8 We, therefore, evaluated the impact of reflex comments, based on lipid results, recommending direct GP referral to the WMFHS.
Methods
Patients and methods
Requesting and reporting of pathology tests by GPs, using our pathology services, are almost exclusively electronic. The electronic requesting of lipids requires the requester to complete two dropdown boxes to determine if fasting or non-fasting and primary or secondary CVD prevention.
Serum cholesterol, HDL cholesterol and triglycerides were measured using methods and reagents supplied by Abbott diagnostics on the Abbott ARCHITECT c16000 analyser (Abbott Diagnostics, Abbott Park, IL, USA). The Friedewald equation was used to automatically calculate LDL-cholesterol in fasting serum samples when triglycerides concentrations were less than 4.5 mmol/L. 9
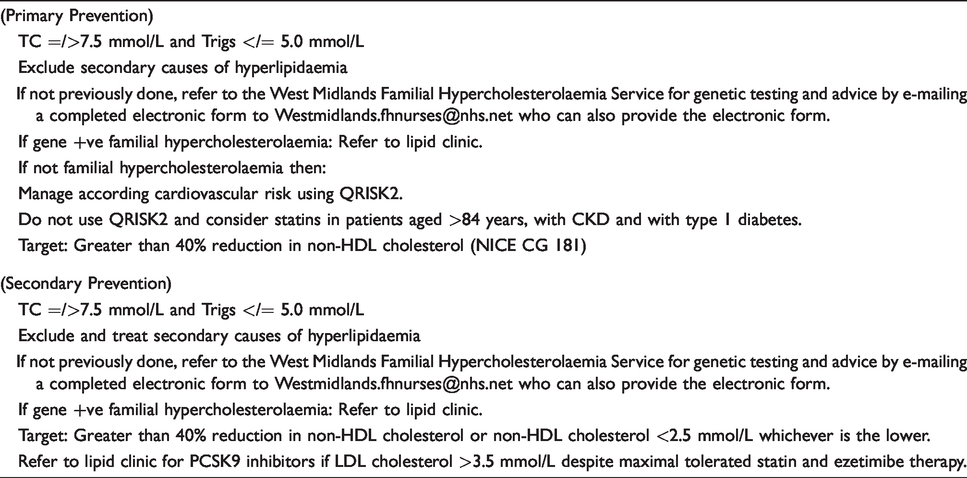
Lipid comments were then appended on all primary care lipid results, including those recommending referral to WMFHS (Table 1). GPs following these recommendations then complete and email a referral FH proforma to the WMFHS. The referrals are reviewed by WMFHS specialist FH nurses, who assess eligibility for genetic testing largely based on the Welsh criteria. 11 Eligible patients are invited to attend the WMFHS and are seen within their respective primary care CCG. Patients undergo full assessment and FH genetic analysis if indicated. Patients with an FH mutation are counselled and provided information on FH and then referred directly into the local lipid clinic for further management and follow-up. Cascade screening is undertaken by the WMFHS. Patients without FH are counselled and discharged back to their GP with advice to manage according to NICE CG181. 6 However, patients with a polygenic aetiology and high CVD risk/family history may also be directly referred to a local lipid clinic for assessment.
Reflex comments advising referral to the West Midlands Familial Hypercholesterolaemia Service.
Data collection
Data from 1 November 2017 to 31 October 2019 were collected from the WMFHS database on referrals to the WMFHS from GP practices in the Wolverhampton CCG and from four comparator CCGs serving a similar size population. The GPs from the comparator CCGs were not provided with automated laboratory-based reflex comments on lipid results.
Patients referred by Wolverhampton GPs were then identified, and the receipt, by the GP, of comments recommending referral to WMFHS was confirmed.
Results
The WMFHS received more referrals from Wolverhampton GPs than any other comparator CCG and greater than the combined primary care referrals from all four comparator CCGs (Table 2).
Number of referrals to WMFHS from Wolverhampton CCG and four comparator CCGs between 1 November 2017 and 31 October 2019.
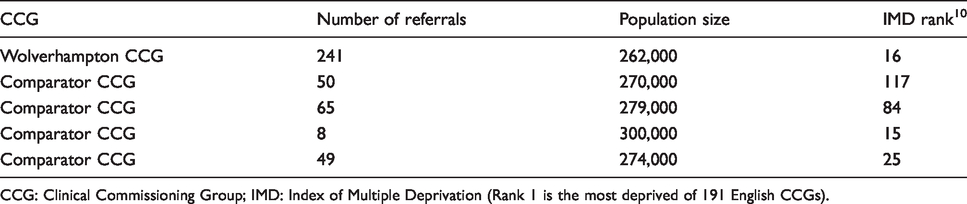
CCG: Clinical Commissioning Group; IMD: Index of Multiple Deprivation (Rank 1 is the most deprived of 191 English CCGs).
Wolverhampton GP referral to the WMFHS was preceded by laboratory-reported reflex comments in all 241 patients. Of those referred, 27 failed to respond to several invitations to attend the WMFHS, 5 were new referrals waiting processing, 108 were ineligible for genotyping and 9 are awaiting DNA results. Nineteen monogenetic mutations were identified in the remaining 92 patients who were genotyped.
Discussion
Although reflective and reflex comments on laboratory reports are widespread7,8 and generally appreciated by clinicians and the public,12–14 evidence for their effectiveness is limited.7,8 Reflective testing is a process whereby a laboratory specialist adds additional tests or individualized interpretative comments or both to aid the diagnosis and management of individual patients.15–18 Reflex testing, on the other hand, is a less time-consuming process based on automated computerized rules to generate appropriate extra tests or interpretative comments or both.
Previous case-controlled studies report that reflective comments on laboratory reports on hypercholesterolaemic patients advising specialist referral increase the detection of FH.15,16 Our report, however, indicates that reflex interpretative comments may also influence clinical practice, since direct referrals from the Wolverhampton GPs to the WMFHS were 3.7- to 30-fold greater than comparator CCGs. Our study is particularly notable since GPs have to obtain, complete and email a referral proforma to the WMFHS; a significant effort.
It is possible that the difference in GP referrals across CCGs could be related to wider social determinants, such as access to healthcare and socioeconomic status, as well promotion of the WMFHS within each CCG. Wolverhampton, however, has a high index of multiple deprivation, and apart from the reflex comments, the WMFHS was not advertised by any local initiative within the Wolverhampton CCG.
Currently in England, only 7% of those with FH have been identified. NHS England, therefore, plans to expand access to genetic testing for FH to identify at least 25% of those with FH in the next five years through the NHS genomics programme. 4 It has been proposed that this will be achieved through NHS Health Checks run by local authorities working with Public Health England (PHE), community pharmacists and GP practices detecting high-risk conditions including FH. PHE recommend systematic searching of primary care records to identify those at highest risk of FH based on their lipid levels. 19 The clinical laboratory, however, is also ideally positioned to facilitate improved detection of FH as demonstrated in this and other studies.15,16
Based largely on the Welsh criteria, 11 45% of referrals were ineligible for genotyping. Direct and more appropriate referral from our laboratory to WMFHS is possible, but this would require GPs to provide more clinical information, when electronically completing lipid requests, to enable calculation of the Welsh score, and patient consent for genetic testing. GP representatives felt that this would require considerable effort as clinical information is difficult to access during the electronic requesting process, especially as many patients on whom lipids are requested would not meet criteria for consideration of FH.
In conclusion, as far as we are aware, this is the first study indicating that reflex comments on laboratory reports directly influence the clinical practice of primary care physicians. This approach may have a role in the identification of individuals with FH and warrants further exploration.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Service evaluation and therefore ethical approval not required.
Guarantor
RG.
Contributorship
BW researched the literature and wrote the first draft. EG and RG conceived the idea of writing a report. All contributed data, critically reviewed the article and approved the final version of the article.