
Abstract
The diagnosis and management of allergy is complex; the clinical symptoms associated with allergic reactions span a broad spectrum of severity, from mild hay fever-type symptoms through to life-threatening anaphylaxis. Obtaining an allergy-focused clinical history is therefore vital for identifying possible allergic triggers and directing testing. However, this focus could be changing as scientific and technological advances have paved the way for developments within in vitro testing for allergy. With knowledge of allergens at the molecular level expanding, there are now the facilities to characterize the sensitization profiles of allergy sufferers and determine the specific molecules (or components) against which the allergen-inducing immunoglobulin type E proteins have been produced. This technology is termed component-resolved diagnostics. We know that accurate identification of immunoglobulin type E specificity, the source of the causative allergen, and knowledge of potential allergic cross-reactivities are required for optimal clinical management of allergy patients. These factors can make allergy a diagnostic challenge outside of a specialist centre, and contribute to the difficulties associated with requesting and interpreting allergy tests. The incorporation of component-resolved diagnostics into current practice has provided a platform for patient-tailored risk stratification and improved the application of allergen-specific immunotherapy, revolutionizing specialist management of these patients. This review discusses the roles of each type of testing in allergy management and predictions for future pathways.
Keywords
Background
Allergy is an increasingly prevalent phenomenon in the population. Allergy is typically associated with a small number of commonly encountered food types, pollens, drugs, and other sources. The molecules within these substances that illicit allergic reactions are known as allergens. Laboratory approaches to assist in the diagnosis of allergic disease revolves around the detection of specific immunoglobulin E (sIgE), directed against likely causative sources of allergens based on an allergy-focussed patient history. The allergens in these tests are mixed in nature, as an extract from an allergen source will contain many different molecules. Advances in laboratory techniques have led to the development of tests that detect sIgE directed against molecularly defined allergenic components. The overarching term for this concept is component-resolved diagnostics (CRD). The ability to distinguish between sIgE against unique components allows clinicians to identify true allergen sensitization (production of sIgE towards a primary allergenic stimulus) from cross-reactivity (whereby sIgE against one allergen can bind to other allergens of similar molecular structure) with greater certainty.
Following a recent survey into the use of CRD within allergy testing across the UK and Europe, 1 it was apparent that use of CRD was becoming increasingly incorporated into routine diagnostics. Its clinical utility however was potentially being compromised due to limited understanding and interpretive guidance for requesting clinicians. With wider implementation, the immunology laboratory must consider the practical aspects for CRD, both methodological and interpretative, prior to the introduction of these specialized tests. Given the need for an allergy-focussed patient history and the fact that CRD testing provides a wealth of complex allergomic data, it is envisaged that molecular allergology will remain in the specialist setting at the current time. However, in the future, allergy testing could be transformed with the assistance of artificial intelligence and machine learning algorithms that guide and direct primary care physicians through the complex interpretation of CRD and allergy diagnostics.
The aim of this article is to provide an overview of diagnostic allergy testing and to review the relevance of some of the recently introduced tests that require a clinical interpretation. It is outside the scope of this review to provide an in-depth evaluation on the applications of CRD. Instead this review will provide an overview of the indications and advantages of using CRD in allergy diagnosis and management.
The burden of allergy for health care
Allergic disease is one of the major causes of illness in developed countries and prevalence is increasing. The World Allergy Organisation estimates that allergy prevalence of the whole population by country ranges between 10 and 40%. 2 In Europe, an epidemiological review placed the prevalence of self-reported allergy at 17.3; thus, nearly one in five people will experience some form of allergic reaction in their lifetime. In the UK, allergic disease affects about one in three of the population. In 13- to 14-year-old children, 32% report symptoms of asthma, 9% have eczema, and 40% have allergic rhinitis. The UK ranks highest in the world for asthma symptoms and is also near the top of the world ranking for allergic rhinitis and eczema. High and increasing trends are also apparent in nut allergy, anaphylaxis, occupational allergy (e.g. latex), and allergic reactions to drugs.3,4 In the 20 years prior to 2012, there was a 615% increase in the rate of hospital admissions for anaphylaxis in the UK. 5
IgE-driven allergic reactions
The vast majority of proteins we are exposed to daily are well tolerated. However, in some individuals, IgE immunoglobulins are produced in response to innocuous ‘non-self’ proteins encountered from various animal, plant, and microbial sources. These misdirected immune responses result in allergic reactions.
Allergic reactions driven by IgE have three characteristic stages: sensitization, elicitation, and late phase. During sensitization, an allergen is recognized by the immune system, causing production of sIgE. The sIgE then circulates in the blood to sites of connective tissue (such as the skin and lungs) where they bind to the complementary high affinity IgE receptors on mast cells. In the elicitation phase, further exposure to the same allergen results in cross-linking of sIgE molecules bound to the IgE receptors through binding of the allergen to two adjacent sIgE molecules. This induces the mast cell to release proinflammatory mediators including histamine, tryptase, prostaglandins, leukotrienes, and complement anaphylatoxins which cause the clinical symptoms associated with an allergic reaction. In late phase responses, further release of biochemical mediators and recruitment of eosinophils and basophils plays a key role in amplification of the allergic reaction.6,7
The severity of allergic reactions is dependent upon the nature of the allergen, the susceptibility of the patient, and the route of exposure. Mild symptoms may be limited to hives, rhinitis, or minor swelling (usually affecting the lips, tongue, and orbital region), whereas severe allergic reactions can induce systemic anaphylaxis. This variation provides a clinical dilemma in managing individual patients. Patients whose allergic triggers and clinical symptoms are consistent with the potential to develop more serious complications requiring assessment from specialist services need to be distinguished from those patients who can be confidently managed in primary care.
Exposure to allergic triggers
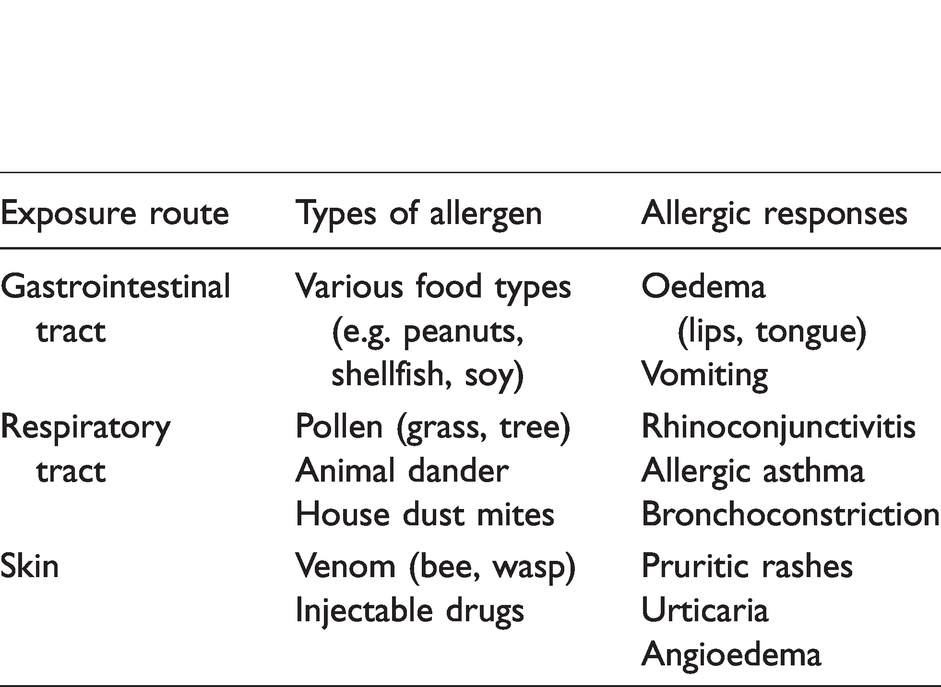
Allergens are most frequently encountered via ingestion, inhalation, or via a compromised skin barrier (Table 1). Food allergies elicit allergic reactions in the gastrointestinal tract upon consumption.8,9 Airborne particles (e.g. pollen) cause allergic reactions in the respiratory system or upon contact with the eyes, 10 while allergens that cross the skin barrier typically cause pruritic rashes and hives. 11 Each of these exposure routes may progress to systemic reactions including anaphylaxis. The extent of allergic reaction is graded by severity of clinical manifestations. 12
Common routes of exposure to allergenic proteins. Protein allergens may be encountered by a variety of routes. Severity of reaction is determined by type of allergen, its native integrity, and the level of exposure.
The clinical approach to allergy diagnosis
In any patient with suspected clinical allergy, investigation is directed by a thorough allergy history which includes details of symptoms and time interval between exposure and onset of clinical symptom. Skin prick testing (SPT) is still a widely used diagnostic procedure and most commonly the first line investigative procedure used in allergy centres across Europe. 13 These in vivo tests involve the cutaneous administration of allergen extracts, and the presence of a localized allergic response indicates a positive or negative result when compared with a control response. SPTs have been shown to have high sensitivity for identifying sensitization in oral challenge-positive individuals, compared with in vitro specific allergen testing,14,15 and are reliable tests for respiratory allergy. 16 Allergen panels for SPT can vary considerably, and studies are limited by the availability of defined allergens. 17 The lack of standardization in the manufacturing of allergen extracts for use in skin testing has also recently been highlighted and is currently being addressed in Europe.18,19 In addition, biological variation between patients affects the test performance. The sensitivity of skin testing is also affected by the threshold for positivity, and it is therefore vital that this is established locally based on equipment and technique or protocol used. 20
The laboratory approach to allergy diagnostics
Following an allergy-focussed patient history to identify potential triggers, and subsequent SPT, in vitro methods to detect allergen-specific IgE are also commonly used. The in vitro tests for specific IgE, as with in vivo SPT, use whole allergen extracts for analysis, and therefore are negatively affected by the heterogeneous nature of purified allergens. This problem is overcome through use of CRD, as the IgE being measured in this case is directed against separate allergen components, and therefore avoids any interference from minor or non-specific allergens. These issues have a significant impact on the usefulness of tests in clinical practice. This highlights the need for specialized allergy services alongside a standardized approach when assessing patients, particularly when selecting patients for immunotherapy in consideration of test results. While this approach remains clinically relevant for the routine mono-sensitized allergic patients, an improved diagnostic approach remains a clinical need, particularly for more complex cases which mainly arise due to the complexities of protein components of allergens, and their respective allergenicity. Subsequent testing using molecular-based allergen components may follow later, in an approach termed the ‘top-down’ diagnostic approach. 21
The increased availability and use of CRD is not only beginning to have an impact on the investigation of these challenging patients but is also unravelling further scientific understanding of the immunological signalling pathways involved in IgE-mediated hypersensitivity. Given the high levels of clinical variability observed between allergy patients, and even between patients with the same apparent allergy, it would appear that multiple factors and signalling pathways are at play following allergen binding and cross-linking IgE on the surface of mast cells and basophils, which can influence the overall clinical outcome.
Molecular data generated from undertaking CRD in patients with peanut allergy have enabled a level of risk stratification to be realized. This has improved diagnosis by introducing a more clear-cut decision points for peanut CRDs and has reduced the number of challenge tests undertaken in clinic. 22 These changes are having significant consequences for the patient. The precise signalling pathways triggered following the binding of each peanut component to mast cell surface IgE have yet to be elucidated, raising the question of whether a single common cell signalling pathway is activated for all allergens, or in fact multiple, cross-talking pathways are triggered depending on the inciting molecule(s).
As we obtain more molecular data for allergens and begin to scratch the surface as to the signalling pathways activated, we have become aware that particular molecules within allergen proteins can exhibit a hierarchy or allergenic dominance, allowing risk stratification to be determined for certain allergies.23,24 This now raises further questions as to whether the IgE-driven immune response triggered by every allergen follows a common sequence of signalling events in order to elicit the well-recognized allergic symptoms. Alternatively, a hierarchy of allergen epitope dominance exists within allergen-driven signalling, which contains multiple cross-talking signalling pathways, activation of which is dependent on the particular allergen molecule–receptor binding.
One way of deciphering this complex enigma is to utilize technologies including CRD, specifically ISAC allergen microarrays. ISAC microarray consists of 112 characterized allergens in a single test. This method provides additional information which can be made available to clinicians, but requires interpretation by highly specialized experts to be of clinical value. Most likely due to this limitation, it has not as yet been fully supported by current guidelines for management of allergy, but has been shown to have significant value in appropriately selected patients, 25 in particular with respect to patterns of sensitization, and idiopathic anaphylaxis.
Promoting the use of CRD and associated platforms such as ISAC in a controlled manner will potentially expand our knowledge of the allergic response pathways and may uncover sensitizations that are as yet unknown. This should not be underestimated given the asymptotic nature of allergens that are yet to be characterized.
How can CRD help?
Allergen families and prediction of severity
Up to 90% of food allergies are caused by a group of animal and plant sources collectively known as the ‘Big 8’: cow’s milk, eggs, peanuts, tree nuts (e.g. almonds, hazelnuts), fish, shellfish, soy, and wheat. 26 The same allergen source can elicit different types of allergic response among individuals. For example, peanuts can cause fatal allergic reactions in some individuals, while others only experience local mild reactions. 27
This variation can be attributed to specific allergenic components and their biochemical properties. Each source contains a number of different proteins, or allergen components, which can cause an allergic reaction; any two individual patients could be allergic to the same or different allergenic proteins within a source. Knowledge of the allergenic components linked to these reactions can help resolve the complex nature of allergy.
Components from different sources can be grouped into allergen families based on shared molecular characteristics. 28 Molecular analysis of the ∼700 known allergens has demonstrated that the majority of allergens can be distributed into few protein families and possess a limited number of biochemical functions. 29 Determining the sensitizing component, and its associated allergen family, can aid the clinician in determining the level of risk. This will ultimately improve the management of allergy patients; high-risk patients can be appropriately given and trained to use adrenaline injector pens, while reassurance can be given to lower risk patients, preventing unnecessary diet restrictions, anxiety, and referrals to tertiary care.
Cross-reactivity between allergens from different sources is explained by the homogeneity exhibited within these protein families. 30 High levels of cross-reactivity with other plant food allergens can result in allergic reactions when consumed (typically raw and/or unprocessed), despite not being originally sensitized to that source. 31 The most prevalent plant-sourced allergens are distributed into distinct families: pathogenesis-related (PR) proteins, profilins, prolamins such as non-specific lipid transfer proteins, and seed storage proteins. Figure 1 illustrates the major allergen components found in peanut (Ara h) and links them to their associated protein families; the individual components (and protein families) are depicted in order of risk severity.
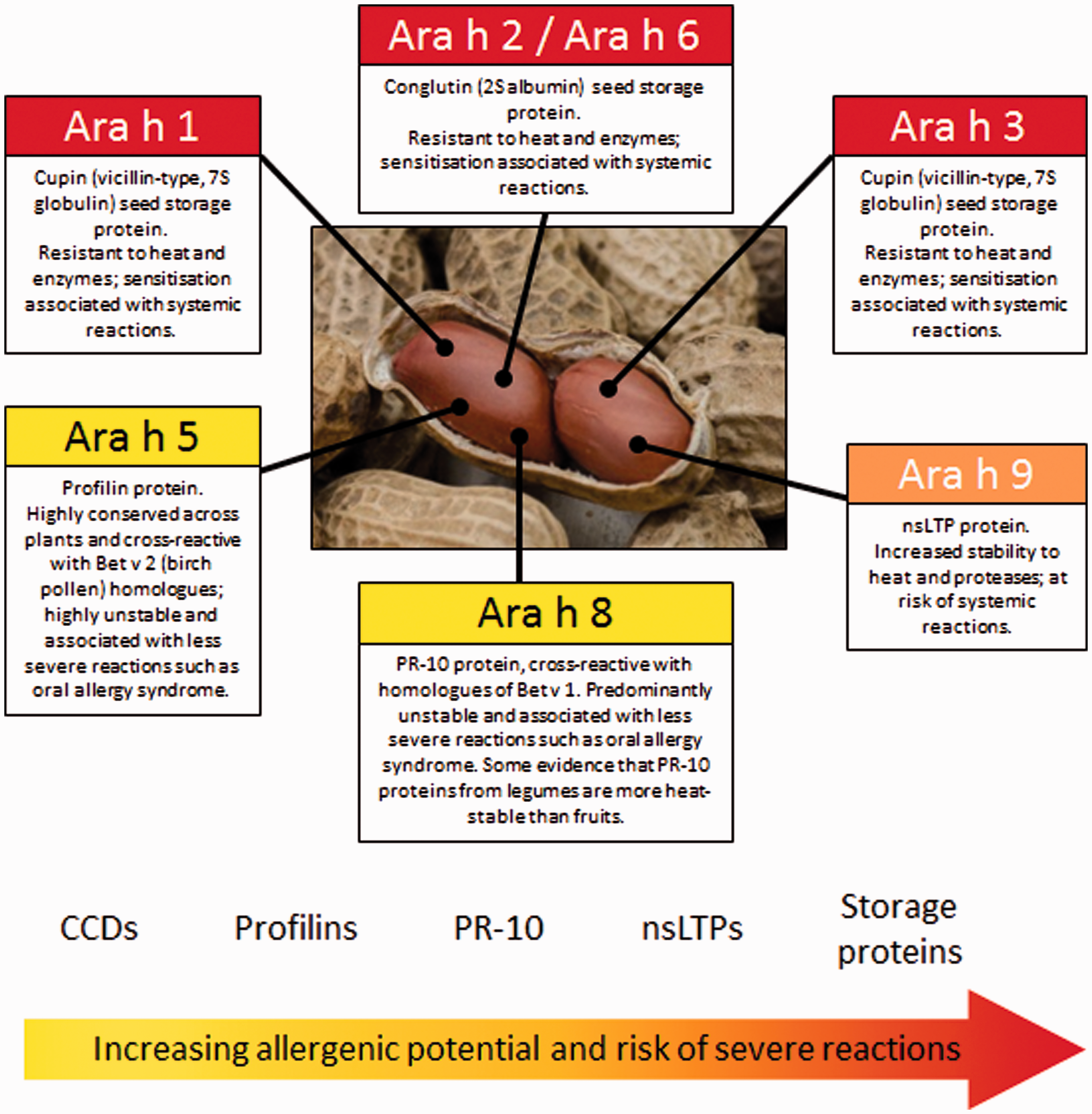
Allergenic potential of peanut (A. hypogea) components. A number of proteins have been identified as allergens within the peanut. Identification of the specific component responsible for allergic sensitization can help to guide clinicians in stratifying patients as high- or low-risk for systemic reactions. CCD: cross-reactive carbohydrate determinant; nsLTP: non-specific lipid transfer proteins. Source: Image obtained from sources that permit free-to-use reproduction for commercial and non-commercial purposes.
Allergenicity (the potential to trigger an allergic response) is reflected in the molecular structure of an allergen, with relevant features such as size, solubility, stability, and conformation contributing to the ability of a particular molecule to trigger an allergic response. 32 A primary allergen is the original molecule that induces sensitization and production of sIgE. Cross-reactive allergens can cause allergic reactions to molecules present in different sources. Cross-reactivity occurs due to similarities between amino acid sequence homology and 3D protein-folding of allergen components. Shared structural conformations allow cross-reactive allergens to interact with IgE previously generated against the primary allergen, with the potential to induce an allergic response. 32 Reactions to cross-reactive molecules may be less severe than the reactions to primary genuine allergens. 21
Cross-reactivity also occurs due to post-translational glycosylation or cross-reactive carbohydrate determinants (CCDs) which exhibit similarity between different sources such as plants, venom proteins, and house dust mites. The production of sIgE against CCDs can give a broad sensitization profile, causing multiple positive responses by SPT or in vitro IgE measurements. 33 These cases can be difficult to interpret for the requesting clinicians; however, as CCD do not usually associate with clinical symptoms, the ability to identify sensitization to CCD can help eliminate clinically irrelevant positive results from true major allergen sensitization.
Allergen molecules
Genuine or major allergenic molecules are classified as those causing species-specific sensitization and subsequent IgE-mediated immune reactions for most allergic individuals. The definition of a major allergen is based on the prevalence of IgE or positive skin prick test to the total allergen extract; however, this does not take into consideration the allergenic risk for eliciting an immune response. Generally, in allergic patients major allergenic molecules bind to IgE and trigger responses in >50% of individuals with an allergy to its source, whereas minor allergens induce allergic reaction in <50% of allergic patients.21,34
Sensitization to Bet v 1, the major allergen of Betula verrucosa (birch pollen), is found in over 90% of birch pollen allergy patients in Europe, with minor panallergen molecules Bet v 2 and Bet v 4 found to be responsible for sensitization of 44.6 and 9.4% of birch allergy patients, respectively.35–37 The term ‘panallergen’ refers to widely distributed ubiquitous protein molecules occurring across multiple species and allergen sources, and includes molecules such as profilins and calcium-binding proteins. 31 The clinical relevance of panallergen sensitization is considered limited, although can present problems if patients develop symptomatic multiple sensitives.38,39 The key aspect of all diagnostic allergy investigations, the allergy-directed clinical history, will ultimately guide interpretation of serological results; however, CRD can have a significant influence on future management options.
Clinical example: Pollen-associated food allergy/oral allergy syndrome (Bet v 1 homologues)
A well-known group of cross-reacting plant allergens are the Bet v 1 homologues, belonging to the PR-10 family of proteins. As illustrated in Figure 2, cross-reactive Bet v 1 homologues are found in a number of allergens from pollen, fruits, nuts, vegetables, and legumes. Exposure, usually of raw, unprocessed allergen-containing foods, can result in a localized, symptomatic IgE-mediated allergic response in patients identified to have an allergy to birch pollen, driven by the major allergen Bet v 1. Using CRD to define primary sensitization to PR-10 allergen molecules can aid diagnosis of oral allergy syndrome. Furthermore, CRD can be helpful in identifying birch allergy patients with sensitization to the minor allergen Bet v 2, thus potential cross-reactivity to components from the profilin family. As profilins are the most widely distributed proteins of the allergen families, cross-reactivity can occur from a wide range of unrelated species, including trees, weeds, grasses, fruits, vegetables, and nuts, but will be distinct from those of the Bet v 1 homologues. Molecule-based approaches enable distinction between genuine sensitization and the less clinically relevant IgE cross-reactivity due to panallergens or carbohydrate determinants. Polysensitivity within birch allergy patients can also be identified using CRD, for which the determination of the primary sensitizing source can help to direct appropriate management, including suitability for allergen immunotherapy (AIT).
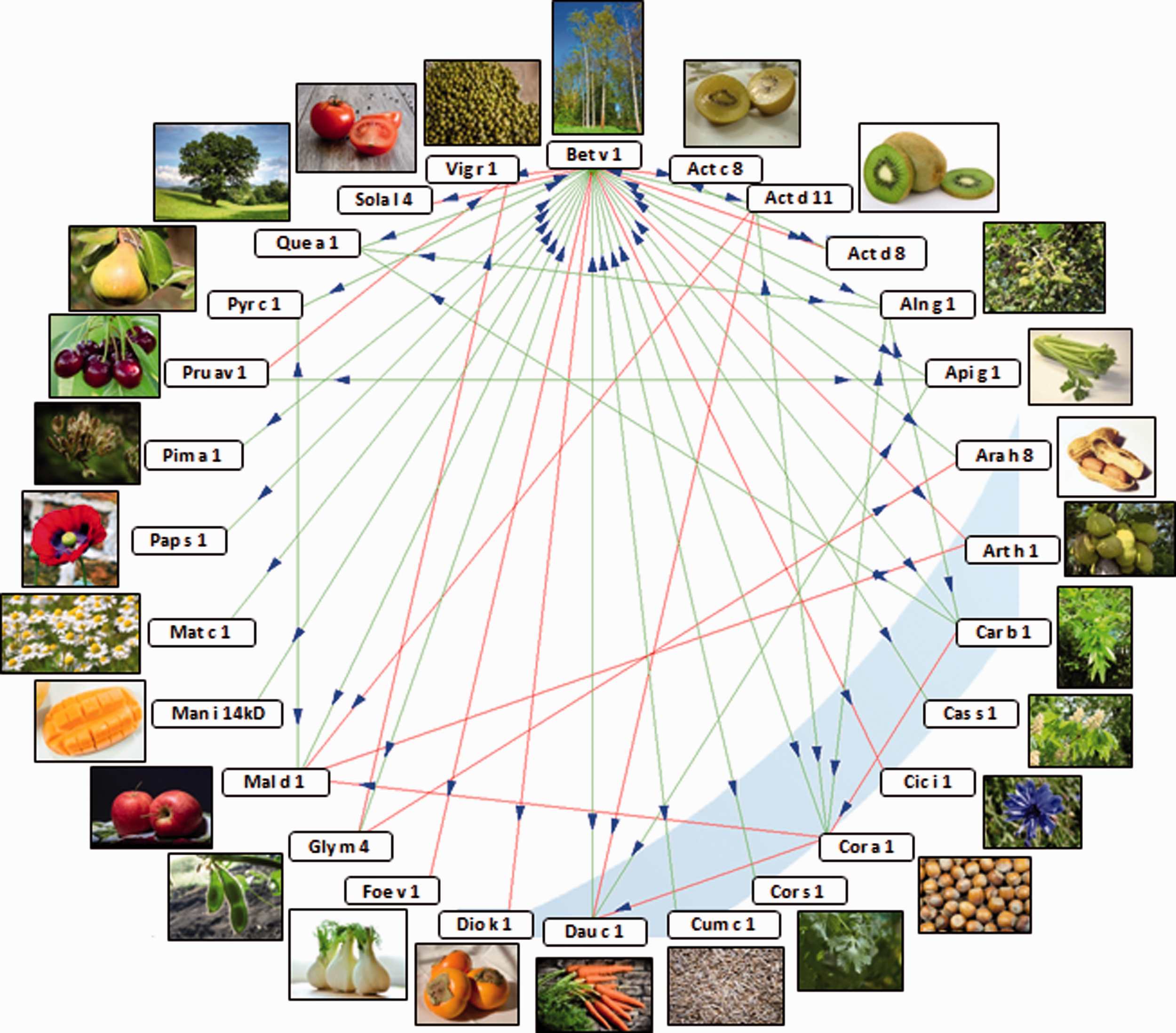
IgE cross-reactivity of Bet v 1. The major birch pollen allergen, Bet v 1, is a PR-10 protein. Sensitization to Bet v 1 is associated with cross-reactivity to one or more allergenic food sources that contain related PR-10 proteins in over 70% of birch pollen allergy cases, causing oral allergy syndrome. Sensitization to Bet v 2, a profilin protein, has a cross-reactive pattern of allergenic food sources distinct to that associated with Bet v 1. Identifying the specific allergenic component of birch pollen to which the patient has been sensitized can guide recommendations for avoidance of likely cross-reactive triggers of oral allergy syndrome caused by ingestion of foods with homologous PR-10 proteins. Reciprocal cross-reactivity between allergen components is demonstrated by double-headed arrows, and unilateral cross-reactivity is demonstrated by single-headed arrows. This figure was generated using the online Allergome O-ring tool. 40 Source: All images were obtained from sources that permit free-to-use reproduction for commercial and non-commercial purposes.
An official list of allergens is published by the World Health Organization and the International Union of Immunological Societies (WHO/IUIS) allergen nomenclature sub-committee (http://www.allergen.org). This list currently contains approximately 880 proteins, drawn from a variety of sources, each proven to have evidence of causing allergic reactions and IgE-binding capacity from the serum samples of at least five patients. Allergen names are assigned by the allergen nomenclature sub-committee for consistent reproduction, compromising a reduced form of the taxonomic name (e.g. peanut, Arachis hypogea, is abbreviated to Ara h), followed by a number to identify the protein family. 41
Diagnostic accuracy in polysensitization and cross-reactivity
Allergy diagnosis is as complex as finding needle in a hay-stack. The patient may report several potential allergenic triggers and it is often difficult to pin-point the exact culprit without detailed allergy-focused clinical history and the additional laboratory diagnostics. Although sIgE testing is widely used in clinical practice especially within primary care settings, the obtained serological results can often further complicate matters, particularly if sensitization to several different allergens is detected (co- or polysensitization).
A major advantage of CRD includes assisting in the prediction of response by specifying ‘genuine’ as well as the ‘cross-reactive’ components in polysensitized individuals; such resolution is not possible using conventional testing. This has been demonstrated for several allergens including food, pollen, venom, and idiopathic anaphylaxis. 39 Use of CRD in these patients not only improves the diagnostic accuracy but also provides additional information around individuals’ sensitization profile which can assist risk stratification (illustrated in Figure 1). Co-sensitization is distinct from cross-reactivity and occurs when IgE-driven responses are triggered by major allergenic molecules from two or more unrelated sources. The determination of genuine co-reactivity and cross-reactivity using CRD can have a significant impact on the interpretation of allergy results, particularly in complex cases whereby patients demonstrate presence of sIgE against multiple antigens. Major advantages of CRD include the identification of primary major allergen components (and protein families) to aid determination of reaction severity and the prediction of additional cross-reactivities including CCD-based cross-reactivity (which are unlikely to elicit reactions).
Furthermore, CRD results will support the appropriate administration of allergy immunotherapy, as treatment responses vary depending on whether genuine or cross-reactive allergen sensitization is determined.
Immunotherapy and scope for personalized treatment
Although exact immunological mechanism underlying the development of immune tolerance, and thus response to allergen-specific immunotherapy remains to be fully elucidated, it is accepted that the allergen component specificity to which the patient is sensitized plays a fundamental role. 42 As highlighted earlier, a considerable challenge for diagnostic investigations is associated with the extracts used to represent the allergen source. For both serological (in vitro) or skin prick (in vivo) testing, these are traditionally based on crude extracts of the allergen source, and therefore contain a mixture of relevant and less clinically relevant allergen components. Immunotherapy products face a similar problem, in addition to the fact that standardization of allergen concentration is usually only reported for major allergen molecules. This is likely to explain the variation in treatment responses between patients as some allergen molecules to which a patient is sensitized to will be poorly represented in the therapeutic product. 43 In light of this, it is vital to identify the allergen components to which patients are responding to, as this will massively assist in anticipating the efficacy of treatment. 44
For instance, not all patients will be suitable candidates for immunotherapy as they will not be sensitized to the major allergens found in commercial immunotherapy extracts, or, due to heterogeneity between therapeutic extracts, the major allergens they are susceptible to are poorly represented. 43 Prediction of treatment response using CRD would prevent inappropriate use of expensive immunotherapy in patients shown to respond to minor allergens, levels of which are found at much lower concentrations in commercial AIT (often unstandardized) and therefore are unlikely to induce allergen tolerance. CRD could also be used to reduce severe adverse responses during treatment. Some of the minor allergen components can be found in high concentrations within commercial IAT and sudden exposure on commencement of treatment could potentially trigger life-threatening anaphylaxis. 45 These situations could be avoided if patients found to be sensitized to these molecular components can be identified prior to starting treatment.
Further considerations for diagnostic allergy testing
In comparison with the heterogeneous nature of SPT and specific IgE tests, the products used in molecular component in vitro allergy tests are highly purified and the constituents of the component tests are fully characterized with no other minor antigens present. Single allergens are used (rather than multiple allergen extracts with varying compositions), and testing is carried out in laboratories where analytical performance is tightly regulated. However, due to the availability of allergens, the repertoire of these assays is restricted by the expansive existence of allergens which cannot feasibly be reflected in analytical tests using current methods.16,17
Both SPT and in vitro diagnostic techniques are restricted in their use of allergenic source extracts. By their nature, they are a mix of proteins and other molecules from an animal, plant, or microbial source. Thus, detection of a positive response only identifies the source material, but not the specific protein to which the immune response has raised a specific IgE against. This lack of specificity causes difficultly in accurately identifying whether positive results are linked to reaction severity and predicting the likelihood of experiencing future allergic reactions to similar molecules in other allergenic sources.17,21
An absence of international calibration standards for specific IgE assays, including allergen component testing, poses further analytical problems with inconsistencies, as a reference standard is only available for the measurement of total IgE (WHO 11/234). Instead, the units measured in sIgE assays are converted into quantitative sIgE antibody levels (kUA/L), using a reference curve calibrated to the WHO standard for total IgE. The assumptions made in the process (around the binding avidity and avidity of sIgE and allergen extract being comparable to the antibody binding when generating the total IgE reference curve) introduce one of many sources of error, resulting in potential quantitative inaccuracies up to 10%. 46 These aforementioned factors have implications for laboratory testing and quantitation of sIgE. Of particular importance, and relevant in order to achieve UKAS accreditation is the ability to define the measurement of uncertainty within allergy diagnostics. Adherence to ISO 15189 laboratory standards requires that each laboratory must define their uncertainty budget for each analyte measured, meaning the inherent error of a result from analytical and biological differences. The lack of standardization makes defining this measurement with confidence a challenge for laboratories.
Multiple studies have also compared the performance of CRD with SPTs and challenge tests (gold standard provocation testing) for diagnosis of allergy, but a consensus has yet to be reached as the analytical performance varies depending on the allergen. 17 When considering this in the clinical pathway, it would seem reasonable that both testing methods are used, particularly while there is an absence of appropriate clinical trials providing evidence of efficacy of treatment by allergen-specific immunotherapy based on components.17,21
The future
As with most diagnostic testing, the immediate clinical context and past medical history are essential in order to interpret laboratory results. Often in the case of allergy, which is not monospecific, the presence of multiple reactivities to a range of allergens presents a diagnostic challenge. This is particularly evident when tests are requested by non-specialists such as general practitioners in the community. This lack of understanding often leads to wide variation in practice and inappropriate referrals to specialist allergy services and the greater use of emergency departments. The getting right first time initiative 47 seeks to address these issues and improve the quality of care within the NHS. By reducing variation and promoting best practice, it is predicated that there will be improved patient outcomes and opportunities for cost efficiencies. The challenge for allergy will be how best to support health care providers in the community given an ever increasing workload and limited time available for patient individual consultations.
The NHS Five Year Forward plan48,49 identifies the need for more GPs who are supported by other professionals. It is hoped that this will be accelerated by partnerships between services in the community and hospital setting. How this might be achieved for allergy diagnostics remains unclear given the shortage of allergy specialists. It is apparent that the current ways of delivering education and information are struggling to have a significant impact which will continue until alternative ways are established. This situation is likely to be compounded with the wider use of CRD. It is therefore important that new ways of delivering allergy services across integrated pathways are developed. Following the publication of the Industrial Strategy 50 and, in particular, the Health Sector deal, 51 it is clear one such area might be the use of machine learning and artificial intelligence. The creation of case-based algorithms might provide opportunities for clinical standardization and reduction in the unwarranted variation of allergy diagnostics. The use of machine learning and big data approaches might also provide a framework to support education across all health care providers potentially operating to a single governance structure. The use of exception rules provided by new cases would help refine the clinical utility of such an approach especially as new knowledge is uncovered by the wider adoption of CRD testing. Empowering patients to be more responsible for their care is a key objective in the NHS Five year Forward plan 49 and the greater use of artificial intelligence might offer a means by which this can be achieved on a large scale.
What does the future hold for the allergy patient? Given the growth in analytical services available over the internet, in conjunction with the influence of social media, it is likely that patients will continue to present to primary care services with an abundance of information, and potentially, with results from unconventional and unregulated sources. Providing the health care provider, in whatever setting, with clear succinct information at the point of consultation will be central for providers of allergy tests to ensure the appropriate test is performed for the appropriate patient at the appropriate time.
Conclusion/summary
At the current point in time, the application and routine use of CRD remain in its infancy, in need of immunology specialists, laboratories, and requesting clinicians to evaluate the wealth of new evidence around their use in the absence of standardized protocols. CRD will undoubtedly add value to understanding the IgE response on a molecular level in addition to expanding the current armoury of tests available for allergy investigation. The enhanced use of CRD by clinicians and allergy specialists is now required in order to obtain useful clinical and laboratory information in terms of sensitivity, specificity, PPV, NPV, and risk assessment. This is evidenced in the wealth of recently published literature; however, there is still a long way to go before CRD is being routinely used, confidently interpreted, and adding value to individual patient cases on a regular basis.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
N/A.
Guarantor
AWR.
Contributorship
Shared intellectual contributions, discussions, writing, and revising of the manuscript EC, CK, NB, AWR.