
Abstract
Background
Alkaline phosphatase isoenzyme analysis is an expensive and time-consuming laboratory test. We evaluated the effect of a locally derived screening algorithm for alkaline phosphatase isoenzyme requests on the number of alkaline phosphatase isoenzyme analyses performed, laboratory cost and patient care.
Method
A total of 110 alkaline phosphatase isoenzyme analysis requests from the year 2015 were reviewed and subsequent alkaline phosphatase concentrations were monitored over a two-year period, to determine if the decision of performing/not performing alkaline phosphatase isoenzyme analysis, based on the algorithm, had an impact on patient care and laboratory cost. All alkaline phosphatase isoenzyme analysis requests with two consecutive elevated alkaline phosphatase concentrations (>upper limit of reference interval) were screened and, subject to the gamma glutamyl transferase being within the reference interval, either Bone alkaline phosphatase or 25 hydroxyvitamin D was measured depending on the age of the patient.
Results
Compliance with this algorithm led to the normalization of subsequent serum alkaline phosphatase in 97% of patients without requiring alkaline phosphatase isoenzyme analysis. The cost of performing Bone alkaline phosphatase and 25 hydroxyvitamin D in-house was £778.50, while the cost of performing alkaline phosphatase isoenzyme analysis would have been £3040. This resulted in a laboratory saving of £2261.50.
Conclusions
Implementation of this algorithm led to a significant reduction in alkaline phosphatase isoenzyme analysis, without compromising patient care. Total savings could be increased if 25 hydroxyvitamin D was used as a first-line test, for all patients with an elevated alkaline phosphatase and a normal gamma glutamyl transferase regardless of age. This algorithm is cost-effective and can be implemented in laboratories with 25 hydroxyvitamin D assay.
Keywords
Introduction
In humans, alkaline phosphatase (ALP) exists in several isoforms that originate from a variety of tissues: bone, liver and kidney (B/L/K ALP) (collectively known as tissue non-specific ALP), intestinal, placental (PLAP or Regan isoenzyme) and germ cell ALP. Liver and Bone ALP account for the majority of serum ALP. Due to both of these isoforms being the products of the same genetic loci with only a difference in post-translational glycosylation, the differentiation between the two isoforms is difficult but can be vital for reaching an accurate diagnosis of liver and bone-related disorders.1,2
ALP isoenzyme analysis is requested by clinicians to aid the differential diagnosis of some diseases, in particular, to differentiate between a liver and bone origin of an elevated total serum ALP. The current analytical technique that is used to separate ALP isoenzymes is electrophoresis. This technique is laborious, expensive and requires specialist interpretation. Consequently, this method cannot satisfy the requirements for inclusion as part of a routine screening panel for determining the cause of an elevated serum ALP. 3 Analysis of Bone ALP and gamma glutamyl transferase (GGT) will establish, in the majority of cases, liver and/or bone origin of the elevated total serum ALP. The resulting effect is a reduced turnaround time and improved patient care due to an earlier diagnosis and hence an earlier management plan. We introduced a screening algorithm for all ALP isoenzyme requests in 2015 to evaluate the clinical and cost-effectiveness of performing these additional tests, as opposed to the traditional ALP isoenzyme electrophoresis.
Method
At the Norfolk and Norwich University Hospitals (NNUH), all ALP isoenzyme analysis requests are vetted according to the screening algorithm outlined in Figure 1. GGT concentration was evaluated if the total serum ALP was found to be elevated (i.e. above the age- and gender-related reference interval). Depending on the age of the patient, above or below 65 years, if a normal GGT activity (within the reference interval) was obtained despite a raised total ALP, either 25 hydroxyvitamin D (25-OHD) or Bone ALP analysis was performed via liquid chromatography tandem-mass spectrometry method (LC-MS/MS) (Waters Corp., Milford, MA, USA) or an enzyme linked-immunosorbant assay (Ostase® BAP EIA, IDS, Tyne & Wear, UK), respectively. The measurement of these analytes was dependant on the age of the patient (≥65 years was used as a cut-off for this algorithm (see Figure 1). For this study, the results of ALP, GGT, 25-OHD and/or Bone ALP in all ALP isoenzyme analysis requests, during the year 2015 (total 110), were collated, and the total serum ALP was monitored for two years in order to evaluate the clinical effectiveness of following this screening algorithm.
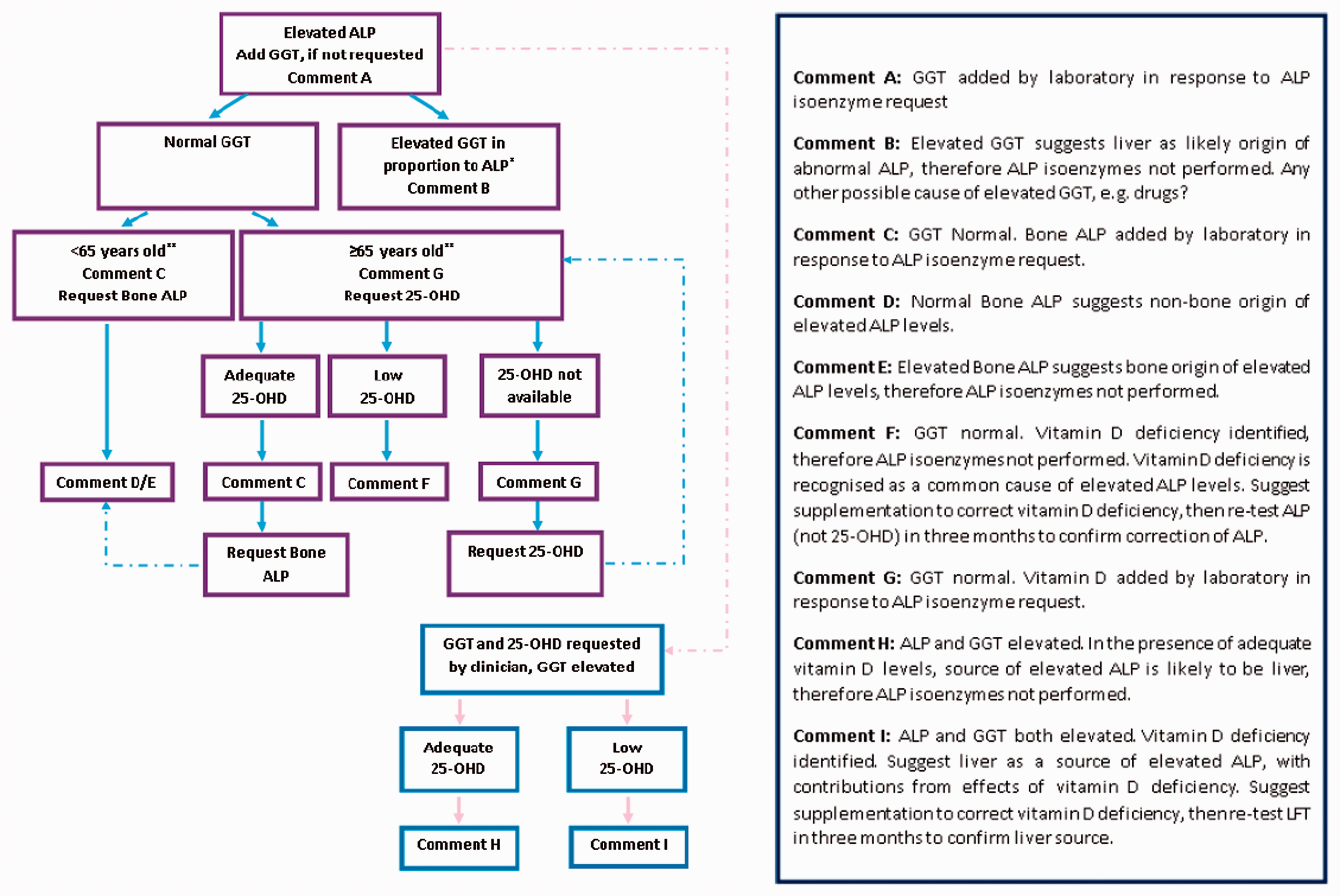
Current ALP isoenzyme screening algorithm at the Norfolk and Norwich University Hospitals.
To evaluate the cost-effectiveness of this algorithm, the total cost of performing Bone ALP and 25-OHD in these 110 ALP isoenzyme requests was calculated and compared against the potential cost of ALP isoenzyme analysis at a referral laboratory.
Results
Number of avoided ALP isoenzyme analyses
Data from 110 ALP isoenzyme analysis requests were evaluated. In 31 requests, the ALP concentration was within or below the reference interval, and ALP isoenzyme request was rejected. One sample for a pregnant patient was sent for ALP isoenzyme analysis upon request from the clinician. The remaining ALP isoenzyme requests (n = 78) met the criteria for screening via the pathway outlined in Figure 1. On reviewing subsequent total serum ALP concentrations over a two-year period, all those patients with an elevated ALP had normalized (to within the manufacturer stated age- and gender-specific reference interval) with the exception of two patients who had died during this period.
Turnaround times
The average turnaround times for performing 25-OHD and Bone ALP in the years 2015/2016 were 22 and 37 days, respectively. Reviewing the turnaround time for 25-OHD in 2017, post-introduction of in-house automated immunoassay for 25-OHD, the turnaround time was reduced to <24 h.
Staff time
ALP isoenzyme testing and interpretation freed 108 h of highly specialized Biomedical Scientist’s (band 7) time per year. The automated tests and the implementation of the full protocol required similar staff time; however, this was delegated to a less specialized Biomedical Scientist.
Costs
The total cost (labour, reagents and equipment use) of performing 25-OHD and Bone ALP was £5.00 and £16.50 per request, respectively. The cost of performing ALP isoenzyme analysis for all 110 requests at a referral laboratory would have equalled £3040. By performing 25-OHD and Bone ALP according to the current algorithm, the total laboratory savings, at the end of 2015, was £2261.50.
Additional findings
When monitoring the ALP concentration post vitamin D replete, as per comment F (see Figure 1), total serum ALP had not normalized by three months (n = 17). On average, ALP concentrations required six months to normalize following vitamin D replacement (20,000 international units (IU) weekly for a duration of three months followed by 1000 IU daily for three months). On nine occasions, a request for 25-OHD was made separately from the ALP isoenzyme analysis request and bypassed the screening algorithm. From these nine patients, seven were found to be 25-OHD deficient or insufficient (results between 15–30 and 30–50 nmol/L, respectively) in addition to having an elevated Bone ALP.
Discussion and conclusions
From evaluating the effectiveness of the algorithm outlined in Figure 1, we have demonstrated that the use of this pathway can lead to increased laboratory savings. The total laboratory savings from the implementation of this screening algorithm, of £2261.50, in 2015 indicates that this algorithm is cost-effective, as it meets the cost of the assays in the algorithm, as well as providing additional savings that can be used for other purposes within the laboratory. Additionally, the introduction of this screening algorithm could save time of highly specialized laboratory staff by avoiding unnecessary ALP isoenzyme analysis and interpretation. A run of ALP isoenzyme through gel electrophoresis (Sebia, Surrey, U.K.), from assay set-up to the clinical interpretation of results, can take up to 3–4 h (depending on batch size). In comparison to this, the screening of requests for ALP isoenzyme analysis with this algorithm can be performed within minutes.
The use of this algorithm provided a clear differentiation between liver and bone-related cause of the increased total serum ALP in the majority of samples, which are the most frequent reasons for ALP isoenzyme requests.2,4 A study carried out by Zhan et al. 2 highlighted that when liver ALP isoenzyme predominated over Bone ALP isoenzyme in traditional ALP isoenzyme analysis via gel electrophoresis, there was an increase in errors associated with the measurement of Bone ALP isoenzyme, which required visual determination to differentiate the two ALP fractions. This error can compromise the accuracy of Bone ALP estimation in certain patient groups, for example patients with cholangitis or intrahepatic space-occupying lesions. 2 Measuring Bone ALP via an immunoassay diminishes the possibility of error associated with visual determination.
Performing 25-OHD as a first-line additional test on those patients with elevated ALP and normal GGT, regardless of age, could lead to a further increase in laboratory savings by avoiding the performance of Bone ALP testing.
Applied in this protocol, ALP proved a reliable and cost-effective marker of the efficacy of vitamin D supplementation. It was noted that the three-month time-frame stated in comment F was insufficient to allow all ALP concentrations to normalize. On average, ALP normalized after six months of vitamin D supplementation. Following this study, we have changed our comment, so that clinicians request ALP measurement six to nine months after commencing vitamin D.
The application of the screening algorithm in 2015, and the addition of Bone ALP and 25-OHD analyses, increased the turnaround time in comparison to the ALP isoenzyme analysis; however, at this point in time, the 25-OHD analysis was performed using an LC-MS method. Following the introduction of the Abbott Architect immunoassay method (Abbott, Maidenhead, U.K.), the turnaround time for the 25-OHD assay was reduced to <24 h.
We highlight the impact of the ALP screening algorithm on laboratory cost and the benefit of performing 25-OHD and Bone ALP in aiding the discrimination between liver and bone-related causes of an increased total serum ALP. A limitation of this algorithm is that a clear conclusion detailing the possibility of Regan or placental isoenzyme is not provided in cases, where ALP is increased along with normal Bone ALP, 25-OHD and GGT. If the clinical history is indicative of a malignancy, then ALP isoenzyme analysis can be requested by the clinician if bone-ALP, GGT and 25-OHD are within the reference interval. Following this study, a further comment, suggesting the possibility of Regan or placental isoenzyme where GGT, Bone ALP and 25-OHD are within the reference interval, has been included into this algorithm.
Footnotes
Contributorship
WDF and JG had the original concept for this paper. JG produced the screening algorithm for ALP isoenzyme requests. SMIH collected and processed the data and prepared a draft report. AC had the original concept for this audit, set the objectives and criteria and assisted with analysis of the data. All authors reviewed and edited the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SMIH.