
Abstract
The most commonly used techniques to measure vitamin D are automated immunoassays which are known to be affected by interferences, especially from immunoglobulins present in the patient’s serum. We present a case of a patient with myeloma in whom interference with the vitamin D assay was identified. An 83-year-old female, known to have IgG myeloma, was found to have a high concentration of 25-OH vitamin D on a routine test without any signs of vitamin D toxicity. She was not taking vitamin D supplements or any other multivitamin preparation and had minimal sun exposure. The initial and subsequent samples run by the ARCHITECT 25-OH vitamin D assay (chemiluminescent microparticle immunoassay technology, Abbott Laboratories, Abbott Park, IL) showed a high concentration of 25-OH vitamin D of 281 nmol/L and 327 nmol/L, respectively. Further fresh samples taken for 25-OH vitamin D and analysed by liquid chromatography-mass spectrometry (LC-MS/MS) and ARCHITECT analysis showed results of 49 nmol/L and 289 nmol/L, respectively. Our patient had high concentrations of circulating IgG paraproteins and had a long history of rheumatoid arthritis; paraproteins and rheumatoid factor may interfere in the assay. In conclusion, we report a case of a patient with IgG myeloma and rheumatoid arthritis with high concentrations of 25-OH vitamin D detected by the Abbott ARCHITECT, but not by a reference method (LC-MS/MS). The most likely cause of the discordant results is interference in the immunoassay by the paraprotein but interference from rheumatoid factor remains a possibility.
Introduction
Vitamin D deficiency is gaining increasing research and clinical interest as a potential factor in bone and non-bone related disorders, such as autoimmune diseases, cancers and cardiovascular disease. 1 The number of vitamin D tests requested in clinics across the world has increased dramatically, and the treatment for vitamin D deficiency or insufficiency is generally affordable and readily available.1–3 It is therefore important that the methods of analysis should be reproducible to aid accurate diagnosis. The most commonly used techniques are automated immunoassays. Immunoassays are known to be subject to many interferences, especially from immunoglobulins present in the patient’s serum. Paraproteins, rheumatoid factor and anti-animal antibodies are the most frequently encountered interfering immunoglobulins.
According to the British Committee for Standards in Haematology, patients with multiple myeloma should be considered for treatment with bisphosphonate infusions to reduce the risk of vertebral fractures and bone pain. Prior to starting bisphosphonate infusions, the British National Formulary recommends correcting disturbances of calcium metabolism (e.g. vitamin D deficiency, hypocalcaemia) and monitoring of serum electrolytes, (sodium, potassium, calcium, phosphate and magnesium). Therefore, we monitor all our patients’ serum electrolytes and 25-OH vitamin D concentrations to avoid unnecessary side-effects.
We present a case of a patient with myeloma in whom interference with the vitamin D assay was identified.
Case report
An 83-year-old female, known to have IgG myeloma, was found to have a high concentration of 25-OH vitamin D of 281 nmol/L with a paraprotein concentration of 38 g/L on a routine test before having a monthly bisphosphonate infusion.
She did not demonstrate signs of vitamin D toxicity. There was no history of any change in appetite, nausea or vomiting. On further enquiry, she was not taking vitamin D supplements or any other multivitamin preparation that may contain vitamin D. She had minimal sun exposure.
Patient's medical and surgical history, drug history and allergy status.
The initial sample was run by the ARCHITECT 25-OH vitamin D assay (Abbott Laboratories, Abbott Park, IL) and showed a high concentration of 25-OH vitamin D of 281 nmol/L in September 2015. On the day, the results of renal and bone profiles were within reference range (creatinine of 58 µmol/L, adjusted calcium 2.29 mmol/L, although potassium and phosphate were unreportable because of haemolysis). A repeat sample was performed on her next monthly visit for pamidronate infusion. The same technique (ARCHITECT 25-OH Vitamin D assay) was used and confirmed an abnormally high concentration of 25-OH vitamin D of 327 nmol/L.
A month later, fresh samples were taken from the patient for further analysis using the liquid chromatography-mass spectrometry (LC-MS/MS), at the Pathology Department of Norfolk and Norwich University Hospitals. The same sample was analysed locally using the ARCHITECT 25-OH vitamin D assay. Again, the ARCHITECT assay confirmed a high concentration of 25-OH vitamin D of 289 nmol/L; a result of 49 nmol/L was reported using the LC-MS/MS method with a 1,25-OH vitamin D concentration of 65 pmol/L by LC-MS/MS.
The most likely explanation for the discrepant results was interference affecting the Abbott ARCHITECT immunoassay.
Discussion
Observations of falsely elevated test results for 25-OH vitamin D and interferences in immunoassays affecting the results have been reported in various studies.4,5 Human anti-animal antibodies are known to interfere with immunoassays and were more commonly found with sandwich-type immunoassays than competitive ones. 5 Holmes et al. reported that the DiaSorin Liaison® immunoassay showed up to a 2.6-fold increase in 25-OH vitamin D results when compared with the LC-MS/MS method from a patient group with 25-OH vitamin D of greater than 145 nmol/L. They also proposed that heterophilic antibodies to goat IgG (human antigoat antibodies) may be the cause of interference in some of the affected samples. 4 Similarly, Cavalier et al. found that human antirabbit antibodies were detectable in the majority of their discordant patients. Since interference from heterophilic antibodies has been observed with the Liaison DiaSorin vitamin D assay and we suspect these heterophilic antibodies may affect other vitamin D immunoassays.
We found an abnormally high concentration of 25-OH vitamin D of 289 nmol/L in our patient using the Abbott ARCHITECT assay. This is a delayed one-step competitive immunoassay using chemiluminescent microparticle immunoassay technology. The sample is pretreated with 8-anilino-1-naphthalensulfonic acid in a triethanolamine methanol buffer as a displacement agent.6,7 As with other immunoassays reported from a recent case study, 8 this method may be subject to interference at any stage of the process. According to the manufacturer guide, potential interference in the ARCHITECT 25-OH vitamin D assay by haemoglobin, bilirubin, triglycerides, protein, rheumatoid factor, human antimouse antibodies (HAMA) and red blood cells is less than 10%. However, in patients with very high concentrations of rheumatoid factor, 25-OH vitamin D may be overestimated by 20%.
Heterophilic antibodies in human serum can react with reagent immunoglobulins, interfering with in vitro immunoassays. 9 Patients who were routinely exposed to animal or to animal serum products can be prone to this interference and anomalous values may be observed. Patients who receive preparations of mouse monoclonal antibodies for diagnosis or therapy may develop HAMA10–12 and therefore specimens from such patients may produce anomalous results when tested with assay kits that use mouse monoclonal antibodies.11,12 Our patient was not tested for anti-animal antibodies, and we are unsure whether this may have contributed to the anomaly on the ARCHITECT 25-OH vitamin D assay.
There are a few possible explanations to why our patient had such high levels reported on the Abbott ARCHITECT assay. She had high concentrations of circulating paraproteins due to IgG myeloma. In retrospect, we observed that as her disease progressed along with increased concentration of paraproteins, the 25-OH vitamin D concentration increased. She was not on vitamin D supplementation. Prior to September 2015, we found that her 25-OH vitamin D concentrations were within expected range, between 64 g/L and 128 g/L (see Figure 1). The paraproteins may have interfered in the assay, binding either directly to the coated microparticles or to the anti-biotin acridinium-labelled conjugate complex, resulting in decreased binding of the conjugate complex to the microparticles and overestimation of the vitamin D concentration. Another possibility is that rheumatoid factor (also an immunoglobulin) was interfering in the assay in a similar way to a paraprotein. This patient had a long history of rheumatoid arthritis. She had evidence of joint deformity, with ulnar deviation and swan neck deformities clinically. Sadly, the patient passed away and we were unable to obtain samples for further analysis.
The scatter plot of serum 25-OH vitamin D (nmol/L) and paraprotein concentration (g/L) of this patient reported in this case report overtime.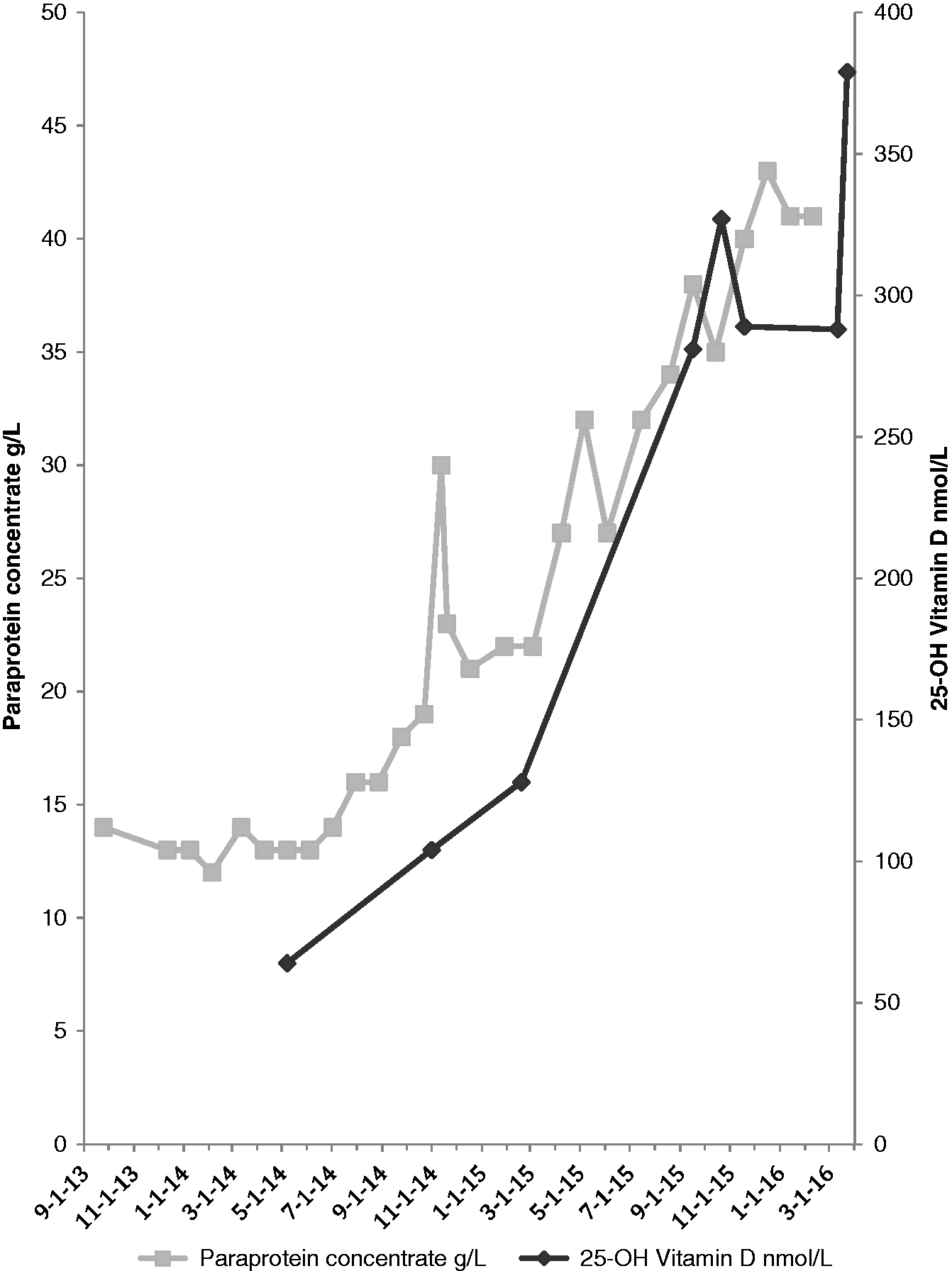
Recently, questions have been asked regarding the accuracy and specificity of immunoassays for 25-OH vitamin D and the fluctuations of assay performance noted in long-term surveys such as the National Health and Nutrition Examination Survey.13–15 In comparison to various immunoassays, the LC-MS/MS is considered as gold standard and is used as a reference method as it is more accurate, precise, and specific.14,16–20 This method has been chosen by the Nutritional Laboratory at the Centers for Disease Control and Prevention and the National Laboratory in the United Kingdom for analysis of vitamin D for health and nutrition surveys as it can separate and quantify vitamin D2 and vitamin D3 in plasma, but most immunoassays cannot.14,21,22 However, the LC-MS/MS method is not commonly used in routine laboratories because it tends to be labour intensive, technically difficult and more expensive. 23
In order to investigate further, we chose LC-MS/MS as the reference method, which confirmed a total 25-OH vitamin D concentration of 49 nmol/L. A recent case report had similar findings. The initial automated analyser reported >150 ng/mL of 25-OH vitamin D concentration with a myeloma-related monoclonal peak of immunoglobulin G (30 g/L) was found. On further analysis, mass spectrometry method confirmed 25-OH vitamin D concentration of less than 25 ng/mL. 8 The LC-MS/MS uses two separation stages: chromatography based on polarity (using hexane extraction prior to chromatography), followed by mass spectrometry, detecting mass-to-charge ratio. The MS/MS step is highly specific because fragments unique to the molecule of interest are detected; in this case, 25-OH vitamin D2 (molecular mass of 412.6 ± 0.5 Da) and 25-OH vitamin D3 (molecular mass of 400.6 ± 0.5 Da). 20
In conclusion, we report a case of a patient with IgG myeloma and rheumatoid arthritis with high concentrations of 25-OH vitamin D detected by the Abbott ARCHITECT 25-OH Vitamin D assay, but not by a reference method (LC-MS/MS). The most likely cause of the discordant results is interference in the immunoassay by the paraprotein but interference by rheumatoid factor remains an alternative possibility.
Footnotes
Acknowledgements
The authors thank all the colleagues who looked after this patient and laboratory staff who helped to process samples appropriately.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Consent gained from family member for write up.
Guarantor
LJ.
Contributorship
All authors have made substantial contributions to all of the following: (1) the conception and design of the case, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.