
Abstract
Background
This study developed a novel high-performance liquid chromatography (HPLC) method for the simultaneous quantification of clozapine and its active metabolite, N-desmethylclozapine, in human plasma and investigated the effects of various factors, including genetic polymorphisms in cytochrome P450 (CYP) 2D6, CYP3A5, ABCB1 and ABCG2, on the steady-state plasma trough concentrations (C0) of clozapine and N-desmethylclozapine in Japanese patients with schizophrenia.
Methods
Forty-five patients had been receiving fixed doses of clozapine for at least four weeks. The CYP2D6 (CYP2D6*2, CYP2D6*5, CYP2D6*10), CYP3A5 (CYP3A5*3), ABCB1 (1236C > T, 2677G > T/A, 3435C > T) and ABCG2 (421 C > A) genotypes were identified by polymerase chain reaction.
Results
The within- and between-day coefficients of variation (CV) were less than 11.0%, and accuracy was within 9.0% over the linear range from 10 to 2500 ng/mL for both analytes, and their LOQs were each 10 ng/mL. The median C0/dose (C0/D) ratios of clozapine were significantly higher in patients with the ABCG2 421 A allele than in those with the 421 C/C genotype (P = 0.010). However, there were no significant differences in C0/D ratios of clozapine and N-desmethylclozapine among ABCB1, CYP2D6 or CYP3A5 genotypes. In multiple regression analysis, including polymorphisms, age, body weight and biochemical data of patients, the ABCG2 polymorphism alone was correlated with the C0/D ratios of clozapine (R2 = 0.139, P = 0.016).
Conclusions
Among the various CYPs and drug transporters, BCRP appeared to most strongly influence clozapine exposure. Knowledge of the patient’s ABCG2 421 C > A genotype before initiating therapy may be useful when making dosing decisions aimed at achieving optimal clozapine exposure.
Introduction
Clozapine is one of the most effective agents for treatment-resistant schizophrenia in patients who exhibit little or no response to antipsychotic medications. 1 However, clozapine can cause several severe side-effects, including neutropenia, agranulocytosis and seizures, and has been shown to be associated with myocarditis and diabetes.2–7 One of these side-effects, agranulocytosis, is a condition involving a dangerous decrease in the number of white blood cells that led to death in some patients. Therefore, patients taking clozapine need to undergo routine haematological monitoring due to the risk of neutropenia and/or agranulocytosis. In addition, some previous studies have investigated the relationship between clinical response (or side-effects) and plasma clozapine concentrations.8–10 Ulrich et al. 11 reported that serum concentrations of clozapine less than 250 ng/mL are associated with relapse, and the risk of intoxication is increased with serum concentrations greater than 750 ng/mL. Additionally, Freeman et al. showed that clozapine concentrations above 1000 ng/mL increase the risk of adverse effects on the central nervous system (seizure, confusion and delirium). 12 Therefore, the use of therapeutic drug monitoring (TDM) during clozapine treatment is strongly recommended, 9 and follow-up examinations to identify the factors affecting the blood concentration of clozapine are critical in the clinical setting.
Clozapine is absorbed rapidly and undergoes extensive hepatic metabolism.13–15 CYP1A2 and CYP3A have been reported to play an important role in the N-oxidation and N-desmethylation of clozapine to clozapine-N-oxide and N-desmethylclozapine, respectively, whereas CYP2D6 plays a minor role in N-desmethylclozapine formation.13–15 N-desmethylclozapine has pharmacological properties similar to those of the parent compound. CYP3A and CYP2D6 have single-nucleotide polymorphisms (SNPs) that may affect the disposition of many substrate drugs. One report has shown that there are no significant differences in the steady-state concentrations of clozapine or N-desmethylclozapine between Swiss patients with the CYP3A5*1 allele and those with the CYP3A5*3/*3. 16 Additionally, Lee et al. reported that the CYP2D6 polymorphism rs1135840 is significantly associated with the N-desmethylclozapine/clozapine concentration ratio 17 ; however, this polymorphism has not been identified in Asian populations. In Asian populations, although the frequency of the nonfunctional CYP2D6*5 allele is low, the CYP2D6*10 allele, which has reduced activity, is present at a high frequency (about 50%). 18 However, no studies have examined the influence of the CYP3A5*3 and CYP2D6*10 alleles on clozapine exposure. Thus, these polymorphisms may affect the C0 of clozapine and/or N-desmethylclozapine.
Recent studies have reported that drug transporters may also affect the pharmacokinetics of clozapine. 19 P-glycoprotein (P-gp; encoded by the ABCB1 gene) belongs to the adenosine triphosphate (ATP)-binding cassette (ABC) superfamily and is an efflux pump capable of transporting a wide range of compound structures. 20 Three SNPs in the ABCB1 gene, i.e. 1236C > T, 2677G > T/A, and 3435C > T, are associated with low activity of P-gp. 21 Breast cancer resistance protein (BCRP; encoded by the ABCG2 gene) also belongs to the ABC efflux transporter group and plays some roles in xenobiotic elimination in various tissues. 20 An in vitro study showed that clozapine can act as a BCRP inhibitor and may cause drug interactions with BCRP substrates. 22 In the Japanese population, the SNP 421 C > A in the ABCG2 has been shown to be the most prevalent allele (33%) exhibiting functional importance. 23 Therefore, ABC polymorphisms may contribute to the plasma concentrations of clozapine and active metabolites.
In this study, we aimed to comprehensively investigate the effects of genetic variations on the C0 of clozapine and N-desmethylclozapine in Japanese patients with schizophrenia. Additionally, four genetic polymorphisms (CYP2D6, CYP3A5, ABCB1, and ABCG2) and multiple patient factors, including age, weight, and gender, were selected to clarify the contributions of genotype to the pharmacokinetics of clozapine in 45 Japanese patients.
Materials and methods
Chemicals and reagents
Clozapine, N-desmethylclozapine and doxepin as an internal standard (IS) were purchased from Wako Pure Chemical Industries (Osaka, Japan). Stock solutions of clozapine, N-desmethylclozapine and doxepin were prepared independently on two occasions, i.e. once for the calibration and once for the quality control. The solutions were prepared by dissolving an accurately weighed amount of drug in methanol to obtain a final concentration of 1.0 mg/mL. Potassium dihydrogen phosphate, acetonitrile, methanol and acetic acid were purchased from Wako Pure Chemical Industries (Osaka, Japan). Water was deionized and purified using a Milli-Q system (Millipore, Bedford, MA, USA). All chemicals used in this study were high-purity high-performance liquid chromatography (HPLC) grade.
Patients
Forty-five patients (11 males and 34 females) were enrolled in this study after giving written informed consent. Patient characteristics are listed in Table 2. The mean (±standard deviation) age and body weight were 36.4 ± 12.5 years (range, 15–67 years) and 57.9 ± 11.2 kg (range, 38–90 kg), respectively. Study protocols were approved by the Ethics Committee of Akita University School of Medicine, and written informed consent was obtained from each participant prior to the study.
Drug treatment
All patients had received clozapine for at least four weeks. Plasma concentrations of both clozapine and N-desmethylclozapine are known to reach steady state by four weeks after repeated oral administration. The daily clozapine dose was fixed at 100–600 mg/day (Clozaril; Novartis Pharma Ltd, Tokyo, Japan) in all cases, and clozapine was administered once or twice daily at 9:00 and/or 21:00. The patients received no other psychotropic drugs except 200–800 mg/day lithium, 600–1200 mg/day valproate and 16–24 mg/day blonanserin. Patient adherence was confirmed by the nursing staff or their families. Blood samples were taken at 8:30.
Analytical methods
Plasma samples were stored at −20℃ until use. Plasma concentrations of clozapine and N-desmethylclozapine were measured using HPLC with ultraviolet (UV) detection. In brief, following the addition of doxepin (1 μg) in methanol (10 μL) as an IS to 200 μL of plasma, the plasma samples were diluted with 800 µL of water and vortexed for 30 s. This mixture was applied to an Oasis HLB extraction cartridge that had been activated previously with acetonitrile and water (1.0 mL each). Cartridges were then washed with 1.0 mL of 40% acetonitrile in water and eluted with 1.0 mL of 100% acetonitrile. Eluates were evaporated to dryness under vacuum at 70℃ using a rotary evaporator (Iwaki, Tokyo, Japan). The residues were then dissolved in 50 μL of mobile phase, and the samples were vortexed for 30 s. Aliquots of 30 μL were then injected into the HPLC apparatus. The HPLC system consisted of a Shimadzu Nexera and a Shimadzu Work station LC solution chromatography integrator (Kyoto, Japan). The HPLC column was a C18 STR ODS-II column, used as an analytical column (column II; 150 mm × 4.6 mm I.D., particle size 5 µm; Shinwa Chemical Industry, Kyoto, Japan), and the mobile phase was 0.5 M KH2PO4 (pH 4.0)-acetonitrile-acetic acid (65:35:0.1, v:v:v). The temperature for the column was 40℃. A flow rate of 0.5 mL/min was used. Peaks were detected by a UV detector set at a wavelength of 254 nm. The peak areas were used for the quantification of clozapine and N-desmethylclozapine. The limits of quantification (LOQs) were determined as the lowest non-zero concentration measured with a CV of less than 20%, as recommended by international guidelines, 24 and the limit of detection (LOD) was determined as the lowest concentration with a signal to noise ratio of 3:1.
DNA assay
DNA was extracted from a peripheral blood sample using a QIAamp Blood Kit (Qiagen, Hilden, Germany) and was stored at −80℃ until use. For genotyping of the CYP3A5*3 allele, we used the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method described by Fukuen et al. 25 and Gao et al. 26 The CYP2D6*2 and CYP2D6*5 (deleted) alleles and CYP2D6*10 (reduced) allele were identified using long PCR analysis and the PCR-RFLP method, respectively, as described by Naveen et al. 27 The patients were grouped into three groups according to the combination of alleles: extensive metabolizers (EMs; CYP2D6*1/*1 and CYP2D6*1/*2; n = 11), heterozygous EMs (CYP2D6*2/*5, CYP2D6*1/*10, and CYP2D6*2/*10; n = 18) and intermediate metabolizers (IMs; CYP2D6*5/*10 and CYP2D6*10/*10; n = 12). Genotyping procedures identifying the C and T alleles in exon 12 (1236C>T), the G and T/A alleles in exon 21 (2677G>T/A) and the C and T alleles in exon 26 (3435C>T) of the ABCB1 gene were performed using the PCR-RFLP method described by Wu et al., 28 Tanaka et al., 29 and Cascorbi et al., 30 respectively. The ABCG2 421 C>A polymorphism was genotyped using the PCR-RFLP method of Kobayashi et al. 31 The analytic results obtained from PCR-RFLP were confirmed by a fully automated SNP detection system (prototype i-densy; ARKRAY Inc., Kyoto, Japan). All frequencies for the different analysed loci were at Hardy-Weinberg equilibrium.
Pharmacokinetic analysis and statistical analyses
The clinical characteristics of the patients taking clozapine are presented as the number or mean ± SD and the range. The Shapiro-Wilk test was used to assess distributions. The Spearman’s rank correlation coefficient test was used to assess correlations in continuous values between groups, and all the results were expressed as a correlation coefficient of determination (r). All results are expressed as the median (range). Kruskal-Wallis tests or Mann-Whitney U tests were used to determine the differences in continuous values between groups. The C0 values of both compounds were adjusted by the dose of clozapine, and the median C0/dose (C0/D) ratios were used in statistical analyses. Stepwise multiple linear regression analysis was performed to determine the effects of factors that were examined in the univariate analysis. Statistical analyses were performed using SPSS (Version 20.0; SPSS Japan Inc, Tokyo, Japan). Differences with P-values of less than 0.05 were considered statistically significant.
Results
Chromatographic optimization
Typical chromatograms obtained for blank plasma and plasma samples spiked with clozapine and N-desmethylclozapine are shown in Figure 1. The separation of clozapine and N-desmethylclozapine was satisfactory and free of interfering peaks in the biological matrix. The peaks of clozapine and N-desmethylclozapine were clearly separated using a mobile phase of 0.5 M KH2PO4 (pH 4.0)/acetonitrile/acetic acid (65:35:0.1, v:v:v) on a C18 STR ODS-II column at a flow rate of 0.5 mL/min. The LOQ was 10 ng/mL for both clozapine and N-desmethylclozapine, and LOD was 5 ng/mL for both clozapine and N-desmethylclozapine. The validated concentration range of this assay for plasma samples was 10–2500 ng/mL for both clozapine and N-desmethylclozapine. The within- and between-day coefficients of variation were less than 11.0%, and accuracy was within 9.0% over the linear range of both analytes (Table 1). All observed data (intraday and interday precision) were below 15.0%, as recommended based on FDA guidelines.
24
The plasma blank samples that were collected before clozapine administration exhibited no detectable clozapine or N-desmethylclozapine in this assay.
Typical chromatograms of a blank plasma sample (a), plasma samples spiked with 500 ng/mL (b) or 10 ng/mL (c) of clozapine and N-desmethylclozapine and 1 µg/mL of IS, and a plasma sample after oral administration of 250 mg clozapine; the plasma concentrations of clozapine and N-desmethylclozapine were 491.1 and 172.2 ng/mL, respectively (d). Peaks: 1 = N-desmethylclozapine, 2 = clozapine, 3 = IS. Inaccuracy and imprecision of the determination of clozaapine and N-desmathylclozapine in human plasma (n = 5).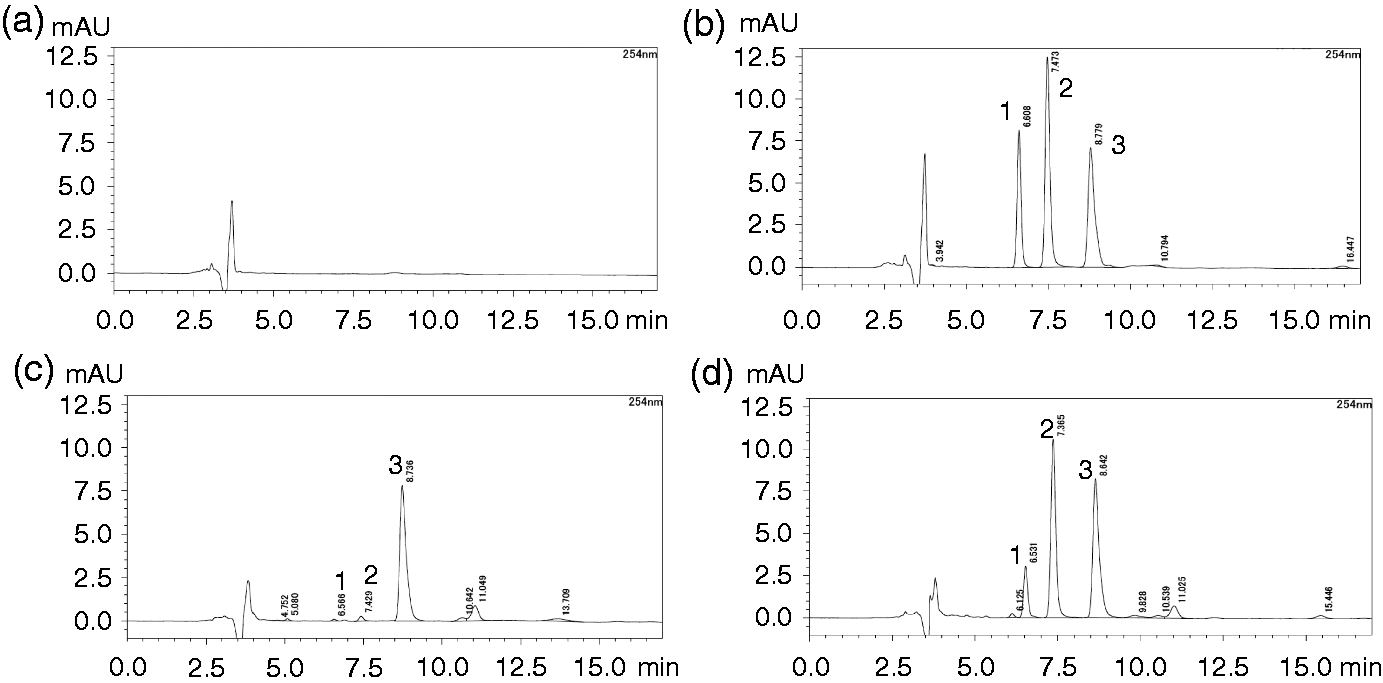
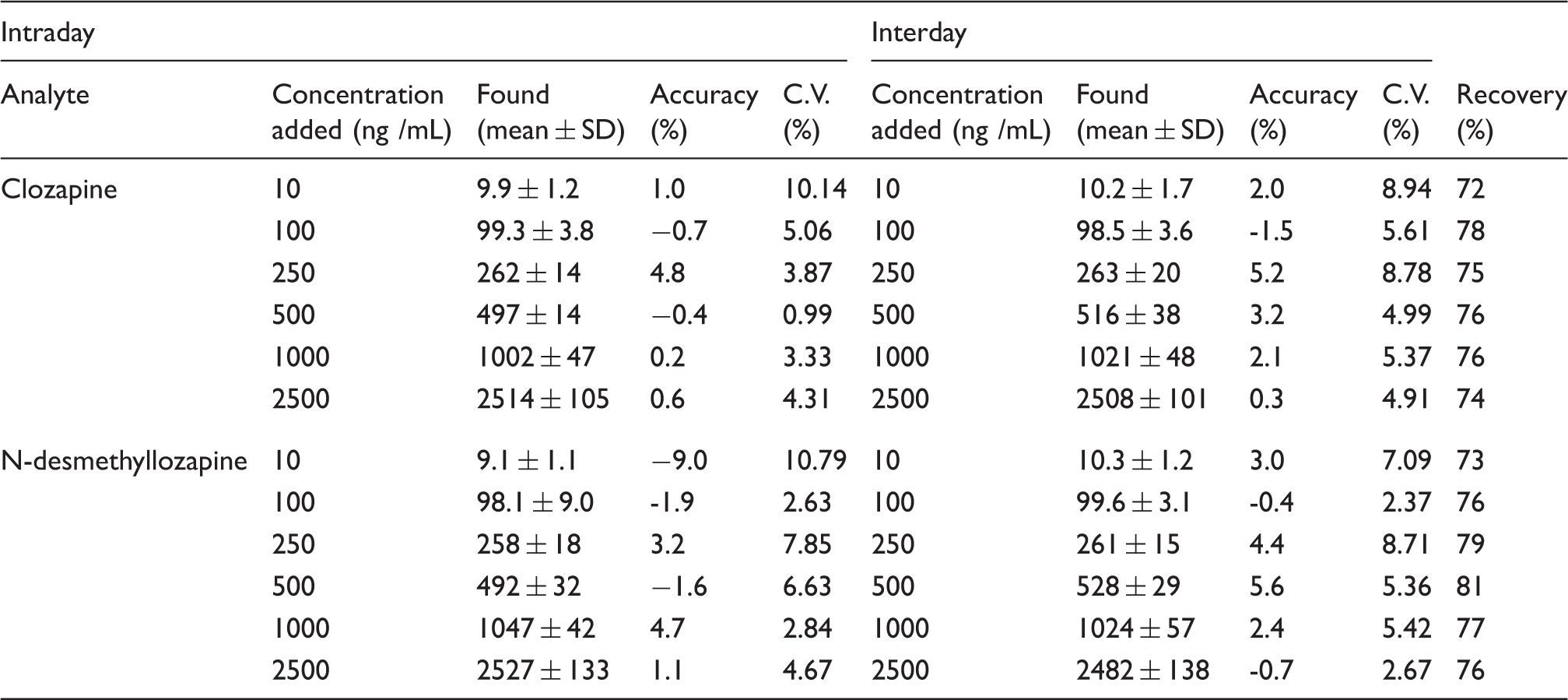
The results of recovery studies from human plasma are shown in Table 1, with the recoveries of clozapine and N-desmethylclozapine determined by adding known concentrations of clozapine (10–2500 ng/mL) and N-desmethylclozapine (10–2500 ng/mL) to drug-free plasma. The extraction recovery values for clozapine and N-desmethylclozapine were 72–78% and 73–81%, respectively (Table 1). The mean recovery for the IS was 71.3%.
In the present study, there were no interfering peaks from endogenous substances with retention times similar to the peaks of clozapine and N-desmethylclozapine in blank plasma samples from healthy subjects (Figure 1(a)). A typical chromatogram of the working solution is shown in Figure 1(b); the retention times for N-desmethylclozapine, clozapine and IS were 6.6, 7.4 and 8.7 min, respectively. The chromatogram of an extracted sample spiked with 10 ng/mL of both clozapine and N-desmethylclozapine and 1 µg/mL of IS is shown in Figure 1(c). The chromatograms of extracted plasma samples obtained from one patient receiving 250 mg of clozapine did not have any interfering peaks (Figure 1(d)). This patient repeated oral doses (250 mg) of clozapine for at least four weeks, and the plasma concentrations of clozapine and N-desmethylclozapine were determined to be 491.1 ng/mL and 172.2 ng/mL, respectively.
Influence of ABC transporter genotypes
Clinical patient characteristics.
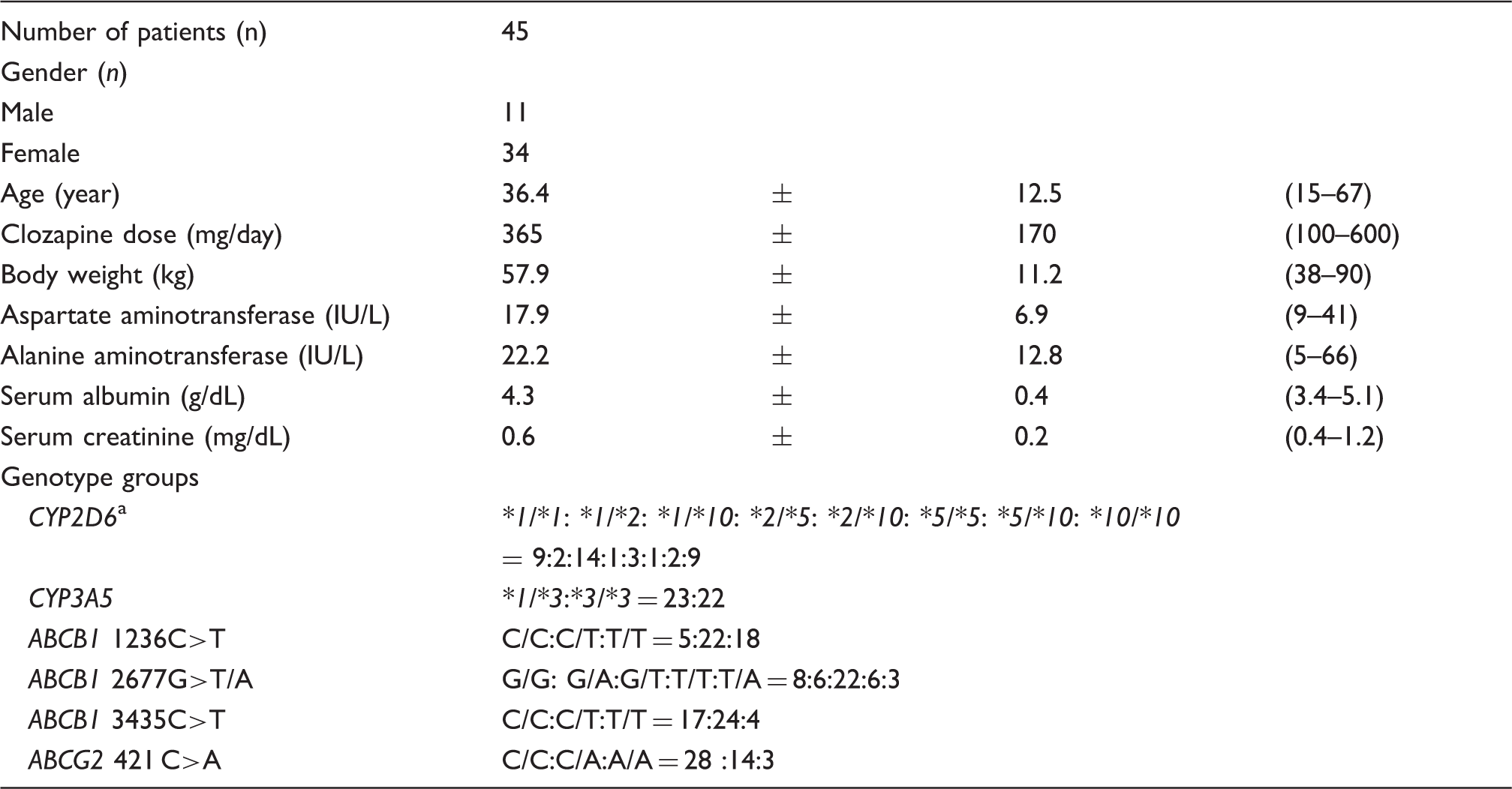
Note: Data are presented as the number or mean ± standard deviation (SD) (range).
The number of patients was equal to 41.
Comparison and correlation with dose-adjusted clozapine concentration and clinical characteristics.
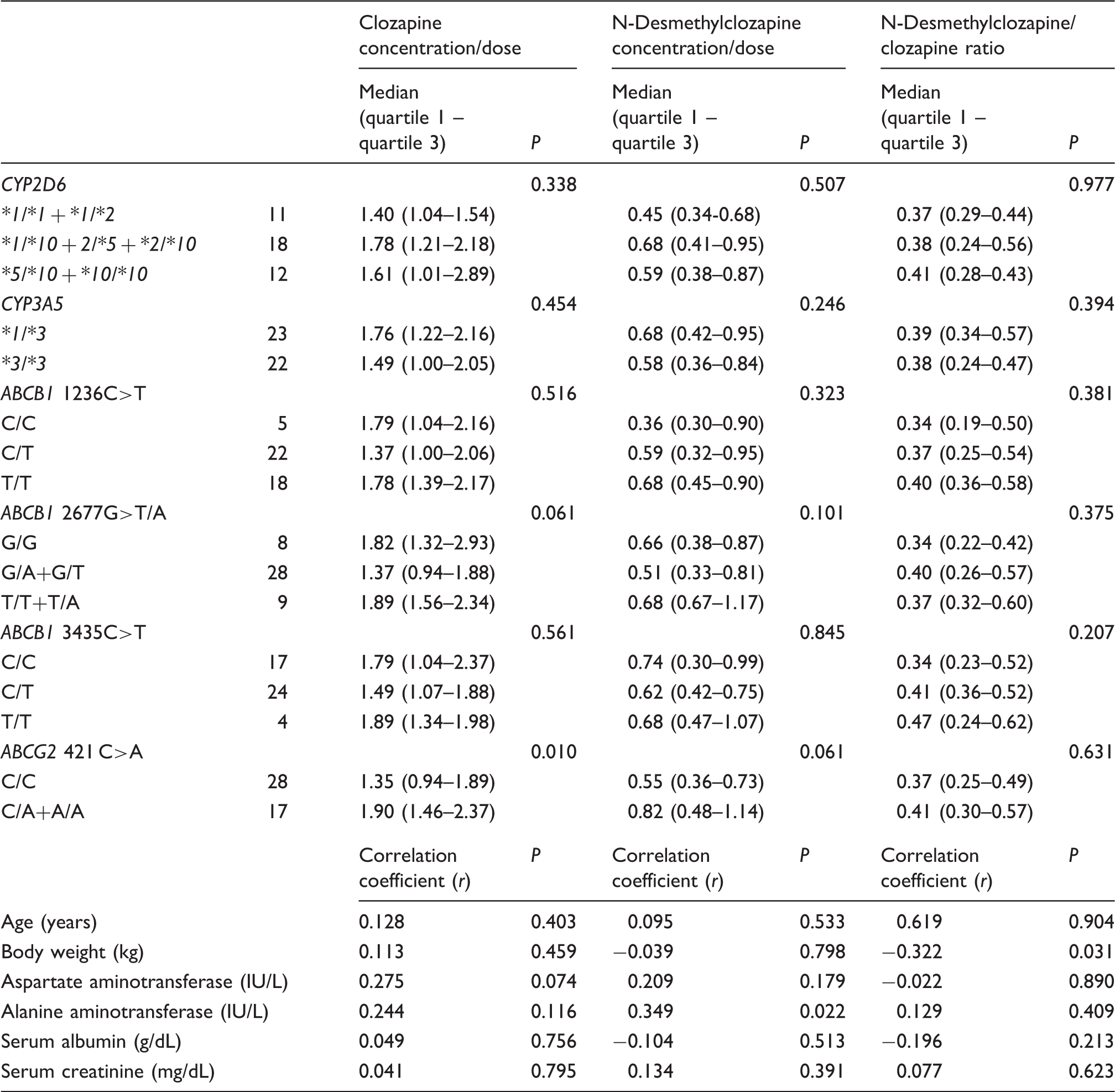
Note: The values are expressed as median (quartile 1 - quartile 3) or correlation coefficient.
Moreover, ABCB1 genotypes (1236C > T, 2677G > T/A, 3435C > T) were not associated with the mean C0/D ratio of clozapine and N-desmethylclozapine (Table 3). There was also no significant difference in the N-desmethylclozapine/clozapine ratio among each ABCB1 genotype (Table 3).
Influence of CYP genotypes
Patients with the CYP2D6 genotype were divided into three genotype groups based on the number of mutated alleles. There was no significant difference in the median C0/D ratios of clozapine and N-desmethylclozapine among the three genotype groups (P = 0.338 for clozapine, P = 0.507 for N-desmethylclozapine; Table 3). Similarly, there were no significant differences in the median C0/D ratios of clozapine and N-desmethylclozapine between patients with the CYP3A5*1 allele and those with the CYP3A5*3/*3 allele (P = 0.454 for clozapine, P = 0.246 for N-desmethylclozapine; Table 3). No differences were found in the N-desmethylclozapine/clozapine ratio among each CYP genotype (Table 3).
Multiple regression analysis
Stepwise forward selection multiple regression analysis of explanatory variable for concentration/dose of clozapine.
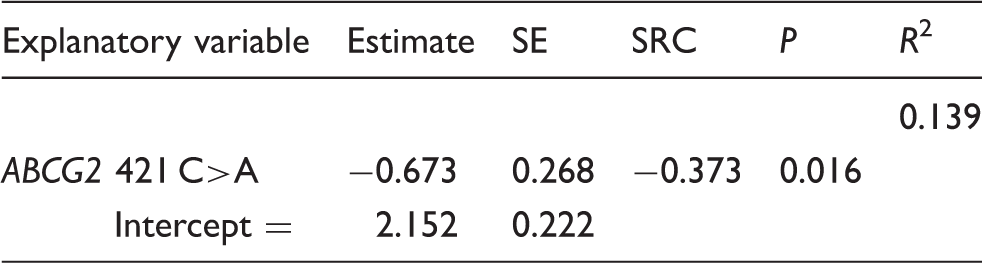
Note: The estimate is the fitted constant associated with each independent variable or intercept.
SE: standard error; SRC: standardized regression coefficient.
Discussion
In the present study, we described a simple, sensitive, specific HPLC-UV method for the simultaneous determination of concentrations of clozapine and N-desmethylclozapine in human plasma. Our method required small sample volumes (200 μL), assays required less than 9 min, the time from blood sampling to the calculation of plasma concentrations was only 30 min, and the measurements were highly sensitive, with LOQ values of 10 ng/mL for both clozapine and N-desmethylclozapine. Satisfactory validation data were achieved for linearity, precision and recovery. This HPLC method grade (LOQ and accuracy) was equivalent to the results of previous reports32–35; however, the solid-phase extraction procedure described here was simple and quick compared with that in other methods reported by Avenoso et al. and McCarthy et al. using liquid–liquid extraction.33,35 Indeed, only a small amount of plasma (200 μL) was required for one complete analysis. The HPLC-UV method reported by Weigmann and Hiemke 32 used solid-phase extraction to extract 1000 μL of plasma, and the LOQ for clozapine was 5 ng/mL. This method requires relatively large sample volumes to achieve sensitivity. 32 In the typical clinical setting, assays that require small sample volumes are desirable for routine drug monitoring of patients. The HPLC-UV method reported by Freeman et al. 34 used a solid-phase extraction method that only required a small amount of plasma (200 μL) and found an LOQ of 25 ng/mL for clozapine. The imprecision and inaccuracy of our developed HPLC assay described here are suitable for routine TDM applications.
By using this new HPLC method, we investigated the associations of polymorphisms (CYP2D6, CYP3A5, ABCB1 and ABCG2) on the C0/D ratios of clozapine and N-desmethylclozapine in Japanese patients with schizophrenia. In the present study, the pharmacokinetic properties of clozapine were affected by the ABCG2 421 C > A polymorphism. Patients with the ABCG2 421 A allele had significantly higher median C0/D ratios for clozapine than those with the 421 C/C genotype. Imai et al. showed that ABCG2 421 C > A polymorphisms are associated with lower expression levels in vitro compared with that of the wild-type gene. 36 In our present study, patients with ABCG2 421 C/A and A/A genotypes exhibited higher systemic exposure of clozapine as compared with those having the 421 C/C genotype. This finding indicated that clozapine pharmacokinetics were affected by the activity of the BCRP transporter and provided evidence that the ABCG2 421 C > A polymorphism played a crucial role in the pharmacokinetics of clozapine. Similar to our analysis of clozapine, the ABCG2 421 C > A polymorphism has been shown to be associated with variable pharmacokinetics and responses in certain ABCG2 substrates, such as leflunomide, diflomotecan, imatinib and topotecan.37–40 These BCRP substrate plasma concentrations were also significantly higher in patients with the ABCG2 421 A allele compared with those having the 421 C/C genotype. Therefore, it is likely that patients with mutated ABCG2 may be at risk of experiencing the concentration-dependent adverse effects of clozapine, even at the same dose of clozapine. In particular, since the allele frequency of ABCG2 421C > A is approximately three-fold higher in Japanese populations (26.6–35.0%) than in Caucasian populations (8.7–11.3%), 36 clozapine plasma concentrations in Japanese populations may be higher than those in other populations; this should be considered by physicians. Knowledge of the ABCG2 421 C > A genotype may be useful when making dosing decisions aimed at achieving optimal clozapine exposure. However, further studies using larger sample sizes are necessary.
Our results showed that ABCB1 genotypes were not associated with the median C0/D ratios of clozapine and N-desmethylclozapine. No differences were found in the N-desmethylclozapine/clozapine ratios among ABCB1 genotypes. These findings suggested that ABCB1 polymorphisms do not influence the pharmacokinetics of clozapine and/or related metabolites. In contrast, two previous studies reported that ABCB1 polymorphisms (3435C > T) affected the pharmacokinetic parameters of clozapine in Caucasian patients.16,19 One report suggested that patients having the ABCB1 3435C/C genotype require higher doses of clozapine to achieve the same plasma clozapine concentrations as patients having the 3435C/T or T/T genotype. 19 However, the observations reported for this ABCB1 polymorphism are inconsistent even with the same probe drugs and among the same disease/racial populations. Numerous studies have also investigated the influence of these polymorphisms on the side-effects of and clinical responses to psychotropics. 41 In fact, recent pharmacogenetic research has demonstrated that responses to fluvoxamine and paroxetine are significantly affected by ABCB1 polymorphisms, including 3435C > T genotypes.42,43 Fluvoxamine plasma concentrations are significantly higher in patients with the ABCB1 3435T/T genotype compared with those having the 3435C/C genotype. 42 In the case of paroxetine treatment, patients with the haplotype combination 3435C-2677G-1236T in the ABCB1 gene show minimal improvement in their Hamilton Rating Scale for Depression scores. 43 However, some studies have failed to find a significant association between ABCB1 3435C > T polymorphisms and treatment outcomes, either for antidepressant plasma concentrations or clinical efficacy.42,44,45 Thus, additional studies are needed to evaluate the effects of ABCB1 polymorphisms on the pharmacokinetics of clozapine.
We also found that the CYP2D6 and CYP3A5 polymorphisms were not associated with the C0/D ratios of clozapine and N-desmethylclozapine. To the best of our knowledge, this is the first study to investigate the relationships between CYP2D6 and CYP3A5 polymorphisms and the metabolism of clozapine in Japanese patients. Data have suggested that CYP2D6 does not have a relevant role in determining the pharmacokinetics of clozapine. There are some plausible explanations for this negative finding. Haloperidol, a known CYP2D6 inhibitor, does not affect the plasma concentration of clozapine. 46 Therefore, CYP2D6 plays a minor role in the pharmacokinetics of clozapine. In contrast, for CYP3A, the most common SNP is the CYP3A5*3 allele 6986A > G within intron 3 of CYP3A5. 47 The CYP3A5*3 allele eliminates the activity of the enzyme. However, no differences were observed in the median C0/D ratios of clozapine and N-desmethylclozapine between CYP3A5 genotype groups. Moreover, one report showed that there are no significant differences in the steady-state concentrations of clozapine or N-desmethylclozapine between Swiss patients with the CYP3A5*1 allele and those with the CYP3A5*3/*3 genotype [16]. Our results were consistent with these previous results. Thus, CYP3A5 polymorphisms did not seem to influence the pharmacokinetics of clozapine.
In addition, CYP1A2 has been reported to be a key determinant for clozapine pharmacokinetics; nevertheless, it is unclear whether CYP1A2 polymorphisms affect the steady-state concentrations of clozapine or N-desmethylclozapine. Therefore, our results are limited because we did not determine the associations between CYP1A2 polymorphisms and steady-state concentrations of clozapine and N-desmethylclozapine. However, because clozapine is metabolized in multiple CYPs, including CYP1A2, and generates an active metabolite similar to the pharmacological effects of the parent drug, the effects of one polymorphism in a CYP gene on steady-state concentrations and therapeutic efficacy may be limited. Furthermore, compared with the polymorphic effects of CYP2D6, CYP2C9 and CYP2C19, reduced activity by CYP1A2 mutated alleles may not cause major variations. Hence, further studies of the effects of polymorphisms in multiple CYPS on clozapine metabolism in larger-scale clinical trials are needed.
Conclusion
HPLC-UV with solid-phase extraction was found to be simple, highly sensitive and rapid. This method was applied to TDM for patients taking clozapine. In addition, the findings of this study suggested that ABCG2 genotypes played an important role in controlling the steady-state C0 of clozapine in Japanese patients. Among the various CYPs and drug transporters, BCRP appeared to most strongly influence clozapine exposure. Knowledge of the patient’s ABCG2 421 C > A genotype before initiating therapy may be useful when making dosing decisions aimed at achieving optimal clozapine exposure and, in conjunction with TDM, may facilitate improved patient management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Japan Society for the Promotion of Science, Tokyo, Japan (grant 15H00475) and grants from the Japan Research Foundation for Clinical Pharmacology, Tokyo.
Ethical approval
The ethics committee of Akita University School of Medicine approved this study, Ref 1258.
Guarantor
MM.
Contributorship
YA, YS-K, and MM researched the literature and conceived the study. YA wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.