
Abstract
Para-phenylenediamine is widely used as a chemical in hair dyes and in combination with henna. This dye is used to paint the body for decorative reasons, to speed the processing time of henna and to intensify the results. Para-phenylenediamine is widely used in the Middle East, North Africa and India.
Several reports have been published of the fatal ingestion of hair dye containing para-phenylenediamine. Here, we describe the case of a 14-year-old girl who ingested the compound but whose prompt treatment prevented her death. Ingestion of para-phenylenediamine produces a typical triad of angioneurotic oedema, rhabdomyolysis and acute tubular necrosis. Awareness of signs of these associated conditions in our patient, together with a comprehensive history, facilitated appropriate treatment to be instituted. We document the steps we took to enable her complete physical recovery.
Keywords
Introduction
Para-phenylenediamine (PPD) is widely used as a chemical in hair dyes and in combination with henna. This dye is used to paint the body for decorative reasons, to speed the processing time of henna and to intensify the results. PPD is used in the Middle East, North Africa and parts of India; this explains the higher prevalence of toxicity in these regions. 1 Toxicity with this compound has been previously reported, but infrequently.
Systemic toxicity of PPD occurs in two phases. The early acute phase occurs some hours following the ingestion. Burning and numbness of the mouth, tongue swelling, airways obstruction, angioedema and vomiting are common.2,3 The second phase occurs (after a few days) after more systemic damage has taken place, due to the absorption and distribution of the toxic metabolites throughout the body. Dark urine 4 (cola- or chocolate-like colour), oliguria or anuria, acute kidney injury, skeletal muscle pain with tenderness and rigidity, rhabdomyolysis, intravascular haemolysis5,6 and drowsiness 7 are seen.
PPD is chemically related to benzene and aniline compounds which have direct toxic effects on the renal parenchyma. 4 Exposure to these chemicals may lead to intravascular haemolysis, haemoglobinuria, methaemoglobinaemia and rhabdomyolysis all of which are implicated in the associated acute kidney injury.4,6,8
PPD poisoning is generally characterized by the triad of angioneurotic oedema, rhabdomyolysis and acute tubular necrosis. Diagnosis requires a high degree of suspicion and a comprehensive history. There is no specific antidote. Therefore, management is mostly supportive, so prompt identification of the unfortunate cases reduces mortality and morbidity rates.
Case report
A 14-year-old female presented with abdominal pain, vomiting, dizziness, progressive orofacial swelling and shortness of breath of 3 h duration. In the Accident and Emergency Department of Omdurman Military Hospital, Sudan, a lifesaving tracheostomy was performed with ventilation. A diagnosis of acute angioedema was made. Intravenous hydrocortisone sodium succinate, chlorpheniramine maleate and intravenous furosemide were administered. The patient admitted to ingesting the hair dye Tancho® in a suicidal attempt. After initial stabilization, a physical assessment was done: the patient was alert, Glasgow Coma Scale (GCS) 15/15, pulse rate 98 beats per minute with sinus rhythm, blood pressure 110/70 mm Hg, respiratory rate 18 breaths per minute. The patient was transferred to the intensive care unit where forced diuresis and urinary alkalinization were performed. Severe right upper quadrant pain with tenderness was noted. Cardiovascular, respiratory and full neurological assessment were unremarkable. The full blood count and coagulation profile were normal. Her ECG was normal. Thin layer chromatography of her urine was positive for PPD. Her urea and electrolyte concentrations were initially normal but started to rise on the third day. The patient was started on a fluid input–output chart to ensure that she was well hydrated.
Investigations.
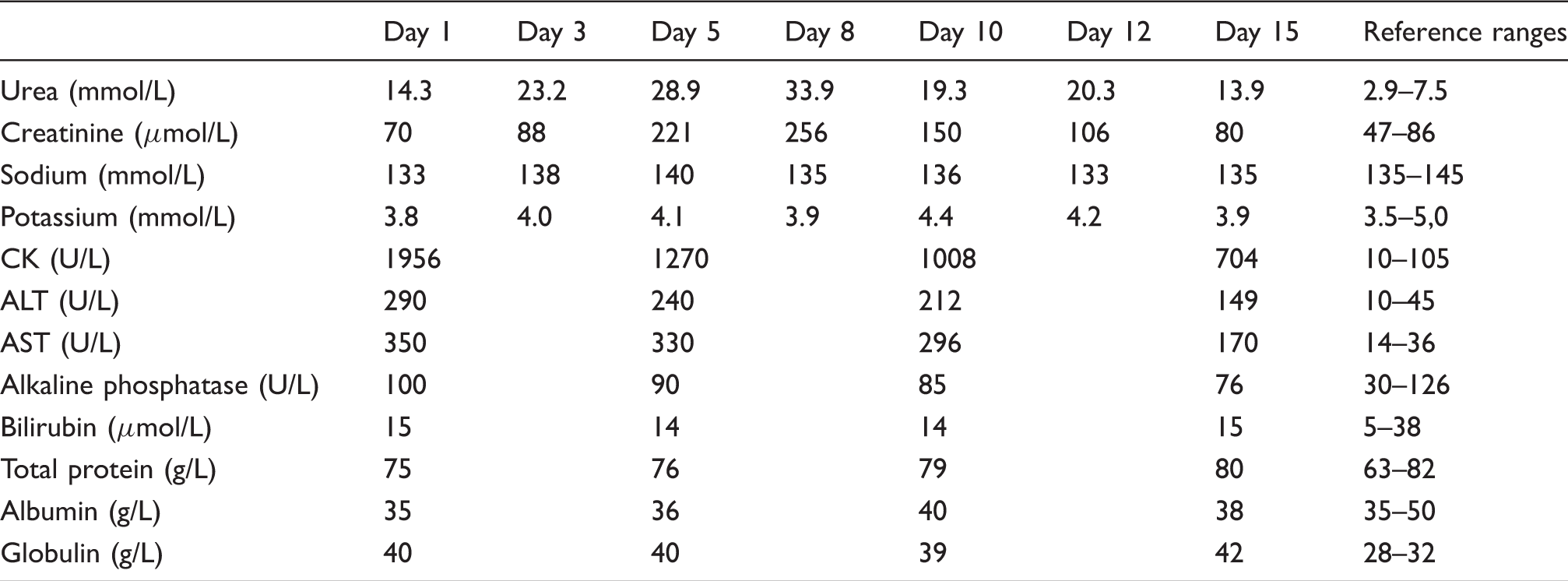
The patient was closely monitored with daily renal function tests and measurement of her urine output. Improvement was seen with supportive management and adequate hydration. Fifteen days after the initial ingestion, renal function, biochemical and haematological tests were repeated and showed substantial improvement. Urine output was also satisfactory.
A full psychiatric assessment was done. A diagnosis of depression was made. Meticulous history revealed a positive family history of psychiatric illnesses and suicide attempts by two older siblings that resulted in death using the same substance. The patient was discharged with a plan for follow-up.
Discussion
Hair dyes are widely available and contain a large variety of chemicals. The commonest and cheapest form in North Africa and the Middle East is known as stone dye, which contains the highest concentration of PPD (70 to 90%). Other branded hair dyes are available in the form of both liquid and powder but contain lower concentrations of PPD, typically 2 to 10%. 9
PPD is a derivative of p-nitroaniline. 5 The product formed on complex reactions of oxidation of PPD is Bandrowski's base, which is highly toxic and allergenic.4,6 PPD is readily absorbed through dermal contact so poisoning may occur without oral ingestion of the hair dye. The extent of symptoms and toxicity are related to the dose when PPD is ingested. The lethal dose of p-phenylenediamine is still uncertain, although estimates range from 7 g upwards. The lethal dose also depends upon individual susceptibility. Death has been reported at a reported dose of 2 g. 9
There is no antidote known to PPD, and there is no experience regarding active toxin removal. Treatment is mainly supportive. Management remains a challenge and requires early identification of cases. Due to the allergenic nature of Bandrowski's base,4,6 patients present with orofacial swelling, difficulty in breathing and upper airway obstruction due to laryngeal oedema. The latter features together with a dark-coloured urine strongly point towards a diagnosis of PPD poisoning, even in the absence of a frank history of hair dye ingestion and also if confirmatory laboratory investigations are lacking.
Other features are of muscle tenderness due to rhabdomyolysis, and acute renal failure as a result of acute tubular necrosis and myoglobinuria. Skeletal and cardiac muscle necrosis have been experimentally induced by N-methylated PPD in rats. 10 Hepatitis, vasculitis, anaemia, vertigo and elevated blood pressure have also been reported. Ocular manifestations in the form of conjunctivitis, chemosis (conjunctival oedema), lacrimation, exophthalmos and even irreversible blindness have been described in humans. 9 Methaemoglobinaemia may occur due to some corrosive component present in the dye. 11 This corrosive component also contributes to rhabdomyolysis and renal toxicity. Skin exposure may result in contact dermatitis, dermatitis exfoliativa and asthma. 12
Long-term use of henna hair dye with a p-phenylenediamine base has been associated with chronic renal disease. 13 PPD may also cause myocarditis, arrhythmia and ventricular tachycardia that may lead to sudden death. Bowen et al. 7 described fatal cardiac arrest in a 22-month old child 3 h after incidental ingestion of the dye. Jatav et al. 14 reported a case of myocardial damage in a 22-year-old female who presented with angioneurotic oedema, arrhythmia, ST elevation in anterior chest leads and a clearly elevated serum troponin, providing evidence of myocardial damage. Chugh et al. 5 reported two patients who developed acute oliguric renal failure following PPD intoxication. The presentation also included angioneurotic oedema and respiratory distress, rhabdomyolysis and acute renal failure. 15
In North Africa and the Middle East, hair dye poisoning is becoming a common cause of intentional self-harm and suicide. It is a life-threatening condition that requires prompt resuscitation. The triad of upper airway obstruction, rhabdomyolysis or renal impairment and chocolate = brown urine should point towards a possible diagnosis of PPD poisoning. A detailed history is very helpful in confirming the diagnosis. Treatment must ensure the airway is unobstructed; early tracheostomy as well as alkaline diuresis and dialysis are the main strategies of management. Treatment is mainly supportive and should be started early to ensure a full recovery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written assent and Informed consent were obtained from the patient and her legal guardian.
Guarantor
LB.
Contributorship
LB wrote first manuscript, researched literature and conceived the study, reviewed and edited the last draft of manuscript; BK was involved in patient recruitment and management, research and review of manuscript; DY structured manuscript, wrote and revised manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.