
Abstract
Background
Hypothyroidism affects 2–5% of the general population. Patients with uncorrected disease suffer significant morbidity and have an increased risk of cardiovascular disease and neurocognitive impairment. Levothyroxine, the treatment of choice, is inexpensive, easy to administer and in most cases restores well-being while normalizing thyroid function. However, 30–50% of individuals on levothyroxine are either over-treated or under-treated and others remain dissatisfied with treatment despite achieving thyroid hormone concentrations within the laboratory reference interval.
Methods
This review is based on a systematic search of the literature for controlled trials, systematic reviews, guideline papers and cohort studies addressing best practice in thyroid hormone replacement.
Results
Recent decades have seen improvements in patient management strategies driven by a better appreciation of levothyroxine pharmacokinetics. However, aspects of therapy such as the optimal timing of medication, strategies to overcome treatment non-adherence and target thyroid stimulating hormone concentrations in pregnancy and in patients with differentiated thyroid cancer remain challenging. Furthermore, there is now a substantial body of literature on common genetic variations in the deiodinases and thyroid hormone transporters and their role in the local regulation of thyroid hormone delivery. The benefits of combination therapy with liothyronine and levothyroxine are uncertain, and while it is theoretically probable that subsets of genetically predisposed individuals will benefit from combination therapy the existing evidence is as yet limited.
Conclusion
Despite the availability of thyroid hormone replacement for more than a century, there are still substantial challenges in practice and opportunities to improve treatment outcomes.
Introduction
Thyroid hormone replacement has been available for over a century and is considered one of the remarkable triumphs of endocrinology.1–4 Thyroid hormones have a range of diverse physiological roles that are essential for normal growth, neurological development and general well-being. 5 Deficiency of thyroid hormones or hypothyroidism is common, affecting about 2–5% of the general population.6–9 Patients with uncorrected disease suffer significant morbidity and have an increased risk of systemic complications including dyslipidaemia, atherosclerosis and neurocognitive impairment. 4 Recent decades have seen a growing recognition that these adverse consequences are not limited to individuals with overt disease but also occur in association with milder degrees of hypothyroidism.10,11 Although hypothyroidism is typically rewarding to treat, about 30–50% of individuals are either over-treated or under-treated6,7,12,13 and remain at risk of the adverse effects of thyroid dysfunction. 14 Furthermore, a proportion of individuals remain symptomatic despite appearing to be biochemically euthyroid. 15 The management of these patients is challenging and often unsatisfactory for patient and clinician alike. This review examines the current best practice in thyroxine replacement therapy and addresses strategies for optimizing outcomes based on existing evidence.
Methods
We searched Medline for articles published between January 1980 and August 2015, using various combinations of relevant key words: ‘hypothyroidism’, ‘treatment’, ‘levothyroxine (LT4)’, ‘triiodothyronine’, ‘antithyroid drugs’ and ‘liothyronine. Additional publications were sourced from references in individual papers, key review articles or in published society guidelines. Our preference was for moderate to high-quality recent studies or older studies that provided landmark contributions to current understanding and practice.
Historical overview
Although the ancient Chinese used chopped animal thyroid glands as a remedy for goitres, 16 specific correction of hypothyroidism with thyroid hormones was not described in the medical literature until the 1890s. 17 By the late 19th century, cases of cretinism were prevalent in the mountain valleys of Europe, and the link between thyroid hormone deficiency and cretinism was gradually being established. 17 In 1874, Sir William Gull described adult patients with features that bore striking similarities to cretinism and the term myxoedema was subsequently coined to describe such individuals. 18 In separate reports, two Swiss surgeons, Kocher and Reverdin, observed similar features following total thyroidectomy. 17 The link between the thyroid gland, cretinism and myxoedema was first proposed by Felix Semon, an English laryngologist in 1883, but this view was initially rebuffed. 18 In 1890, a pair of Portuguese physicians, Bettencourt and Serrano, treated a case of myxoedema by implanting a sheep thyroid gland under the patient’s skin. 19 The following year, the young English doctor, George Murray, reported in the British Medical Journal his successful treatment of myxoedema with hypodermic injections of sheep thyroid extracts. 1 These breakthroughs thus marked the birth of hormone replacement and modern endocrinology. Kendall would later isolate thyroxine in 1914, 20 while Gross and Pitt-Rivers isolated triiodothyronine (T3) in the early 1950s. 21
Synthetic LT4 has been commercially available since the late 1940s but up until the 1960s desiccated thyroid preparations, comprising dried powdered extracts, remained the principal source of thyroid hormone therapy. By the 70s, however, LT4 had replaced thyroid extracts as the main source of thyroid hormone therapy mainly due to difficulties with standardization of the marketed thyroid extract preparations.22,23 Furthermore, LT4 appeared to facilitate more precise dose adjustment and was shown to be peripherally converted to T3, the metabolically active hormone. 24 With the advent of modern thyroid hormone assays, it became apparent that LT4 treatment normalized thyroid hormone concentrations whereas thyroid extracts or combined liothyronine (LT3) and LT4 therapy more frequently led to supraphysiological T3 concentrations.25–27 Today, LT4 is prescribed to approximately 3% of the UK population and remains the treatment of choice for hypothyroidism. 28 Desiccated extracts are currently not licensed for the treatment of hypothyroidism, and only 0.30% of patients are prescribed LT3. 28
Overview of hypothyroidism
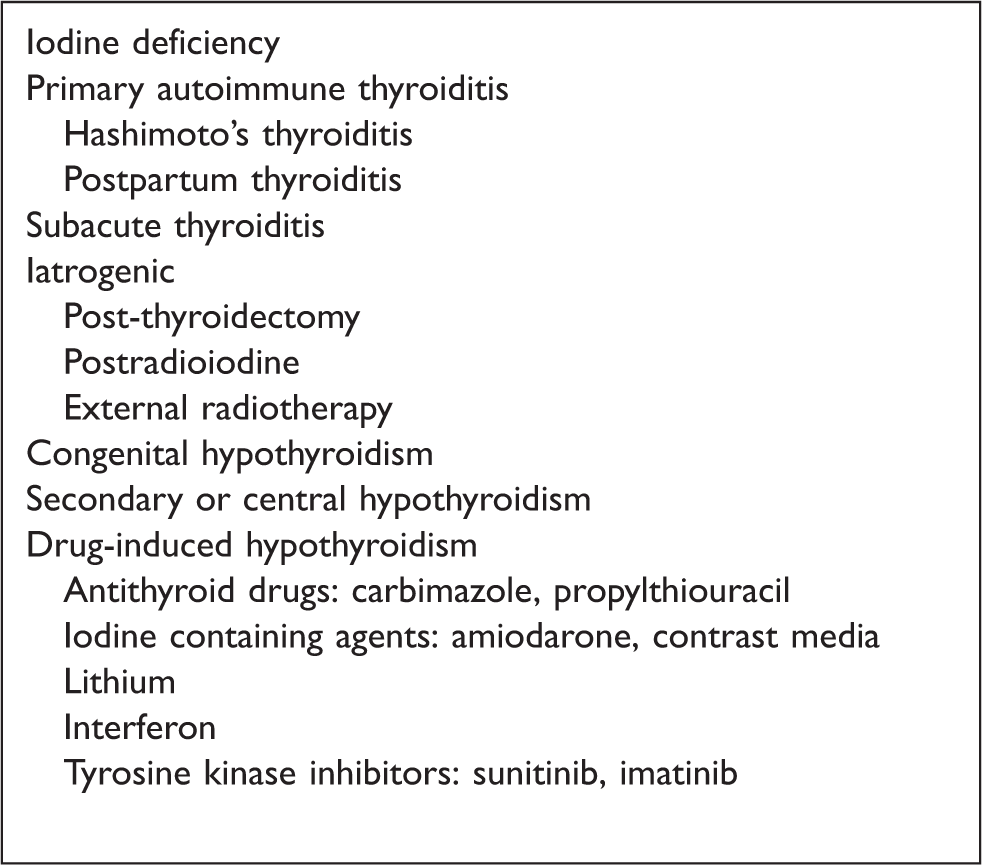
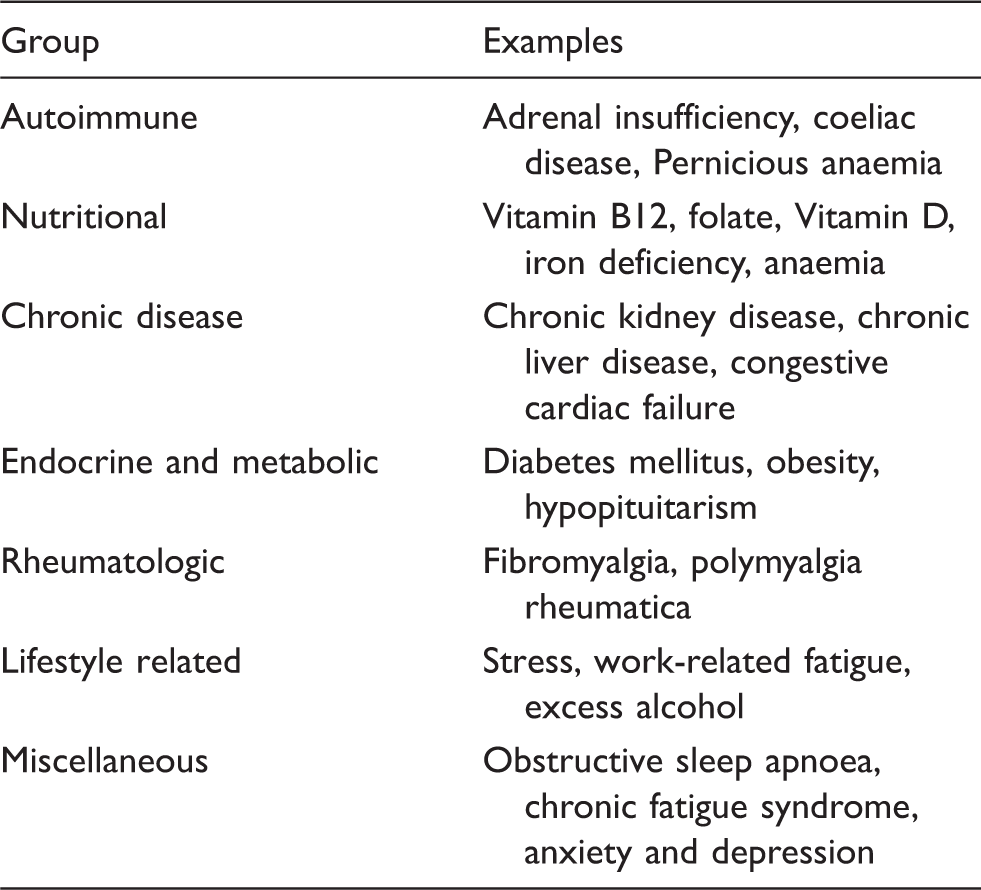
Aetiology
Causes of hypothyroidism.
Epidemiology
Hypothyroidism is common worldwide and affects more women than men. 33 The prevalence of spontaneous overt hypothyroidism in iodine sufficient populations ranges from 1 to 3.5% and rises with advancing age. 33 In a community survey in the northeast of England, the Whickham survey, the prevalence of overt and subclinical hypothyroidism was 7.5% in women and 2.8% in men. 8 Data from the United States National Health and Nutrition Examination Survey (NHANES) showed a prevalence of 4.6% for primary hypothyroidism with overt hypothyroidism in 0.3% of patients. 7 Annual incidence rates in the United Kingdom range from 3.5 to 5.0 per 1000 women and 0.6 to 1.0 per 1000 men.9,34 Hypothyroidism is even more common in particular groups of patients including those with other autoimmune conditions such as type 1 diabetes and Addison’s disease, in individuals with a family history of thyroid disease, women in the postpartum period, those over 65 years of age and in individuals with Down’s syndrome and Turner’s syndrome. 4
Diagnosis
The classic symptoms of hypothyroidism such as fatigue, cold intolerance and mental slowness are recognizable to most clinicians. However, many patients are asymptomatic or present with non-specific symptoms that are indistinguishable from a variety of other conditions.4,35 Indeed, the literature is rife with reports of atypical cases with a plethora of neurologic and psychiatric manifestations.4,36,37 The extreme state of myxoedema coma is less common nowadays but is still encountered in the elderly with neglected disease. 38 The diagnosis of primary hypothyroidism should always be confirmed by the finding of an elevated serum thyroid stimulating hormone (TSH) concentration. 4 In overt hypothyroidism, serum TSH concentration is raised together with a low serum concentration of free thyroxine (FT4), whereas in subclinical hypothyroidism, serum TSH is raised with normal serum FT4 and free triiodothyronine (FT3) concentrations.2,4 Positive thyroid antibodies are helpful in confirming autoimmunity. Mildly abnormal tests in patients with atypical or non-specific symptoms should be re-checked after six weeks as such abnormalities are commonly due to non-thyroidal illness rather than to intrinsic thyroid disease and will normalize with time.
Thyroid hormone physiology
Thyroid hormones are secreted from the human thyroid gland at a molar T3:T4 secretion ratio of approximately 1:14. T3, the biologically active hormone, is predominantly derived from peripheral T4 mono-deiodination24,39 (Figure 1). The process of T4 conversion accounts for roughly 80% of T3 production and is facilitated intracellularly by a series of tissue deiodinases which are sensitive and responsive to T3 concentrations (Figure 1). Thyroid hormone secretion is regulated through classic feedback on the hypothalamo-pituitary-thyroid axis (Figure 1). In individuals with thyroid dysfunction, the relationship between T4 and TSH is inverse logarithmic such that small changes in T4 are reflected in large inverse changes in TSH. Accordingly, TSH is a sensitive and early biochemical marker of thyroid gland failure and is elevated in the face of normal FT4 and FT3 concentrations in individuals with subclinical hypothyroidism.10,40
Thyroid hormone regulation and action.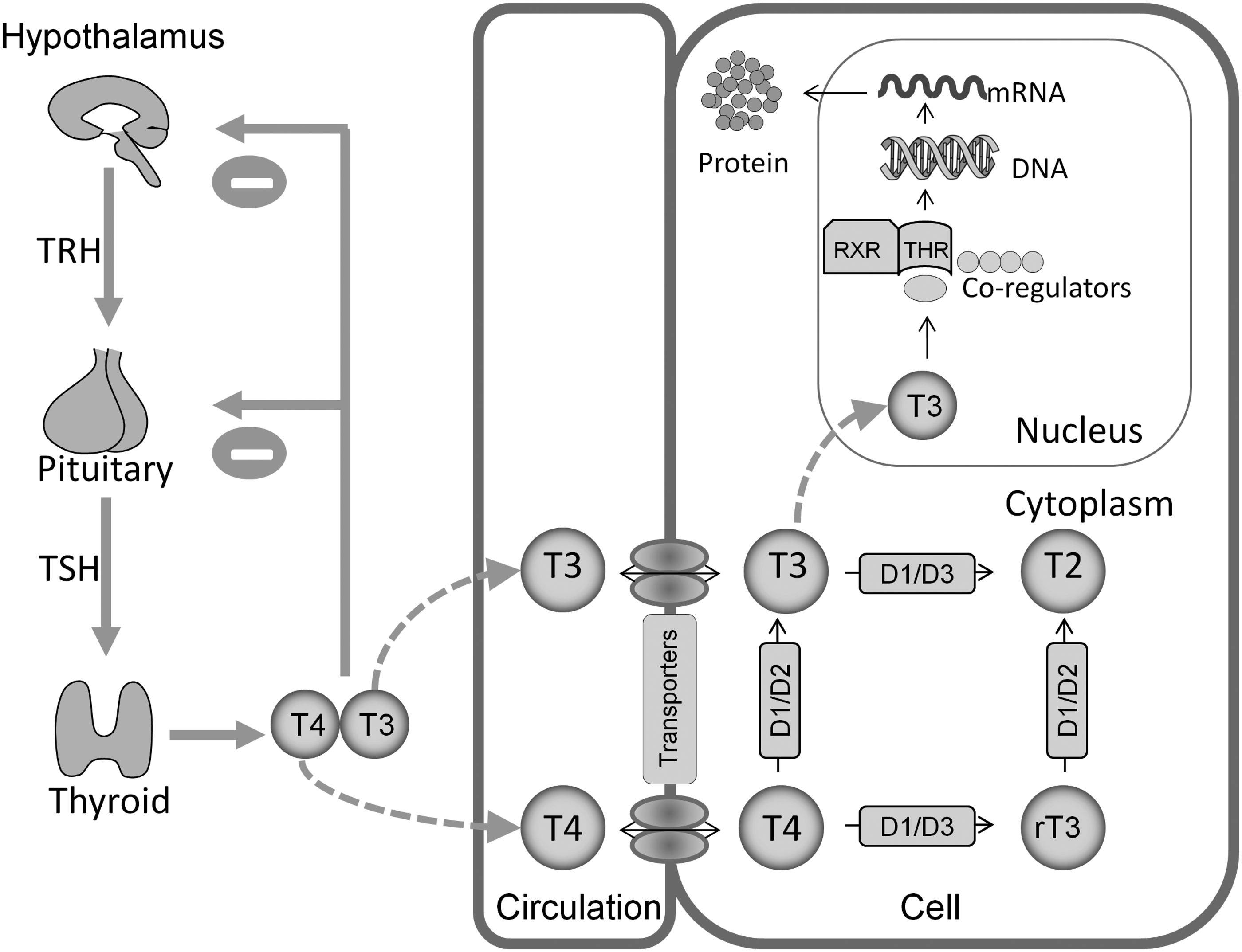
The relevance of thyroid hormone abnormalities may, however, differ according to the individual. Longitudinal studies in healthy subjects show narrow intraindividual variation in serum FT3 and FT4 concentrations despite wide interindividual variation. 41 Thus, each individual may be considered to have a ‘set point’ for thyroid hormones, which is constant for that individual but varies widely from one person to the next. 41 Consequently, some individuals with a biochemical diagnosis of subclinical hypothyroidism may already have established thyroid failure depending on the degree of FT4 deviation from their set point, whilst for others it may be their norm.
Therapy and targets
Primary hypothyroidism
In primary hypothyroidism, the goal of therapy is to achieve well-being and restore serum TSH concentrations to normal values.2,3 LT4 is inexpensive and easy to administer, and most patients report symptomatic relief within weeks of initiating therapy and are able to continue lifelong therapy without adverse effects. LT4 is effective in oral formulation and about 70–80% of the administered dose is absorbed, primarily from the small intestine. 3 Tablets should be taken with water at least 30 min before food or beverages and should be taken apart from other medications, ideally first thing in the morning or at bed time. Treatment should be initiated with full replacement doses (0.8–1.6 µg/kg/day) except in the elderly or in patients with cardiac disease for whom smaller starting doses may be required due to the small risk of inducing cardiac ischaemia. For patients with adrenal insufficiency, LT4 should be delayed until steroids have been initiated as LT4 therapy may worsen adrenal insufficiency. TSH should be re-checked six weeks after initiation, and the dose adjusted to achieve concentrations within the reference interval.2,3 Further adjustments may be required and once stable, TSH can be monitored annually. Some patients may feel better with the TSH in the lower half of the reference interval but deliberate TSH suppression below the lower limit of the reference interval, certainly below 0.1 mU/L, should be avoided due to the risk of the cardiac and skeletal complications associated with over-treatment. 14
Subclinical hypothyroidism
The optimal management of subclinical hypothyroidism remains uncertain. This biochemical diagnosis affects about 5–10% of the general population, 10 and while it may represent a state of early thyroid failure, not all individuals develop overt disease. Approximately 2–5% of patients per year progress to overt hypothyroidism, especially those with positive thyroid antibodies or a TSH concentration > 10 mU/L. 10 Cohort studies show conflicting data on the association between coronary heart disease and subclinical hypothyroidism.42,43 A meta-analysis of 11 prospective studies reported an increased risk of coronary heart disease and mortality in patients with subclinical hypothyroidism. 44 However, others have shown that this association appears only to reach significance in individuals aged < 65 years 45 or those with a TSH concentration > 7 mU/L. 44 Most authorities now recommend therapy for subclinical hypothyroidism in individuals with positive antibodies, TSH concentrations > 10 mU/L, goitre or symptoms of hypothyroidism and increased cardiovascular disease risk. 10 Treatment is also recommended in pregnancy or in women who are planning conception in order to avert the risk of fetal hypothyroidism. 46 In recent years, the UK has seen an increasing trend towards LT4 initiation at lower TSH thresholds, but the benefits of this practice remains unproven. 47
The elderly
Several important considerations apply in the approach to hypothyroidism in older individuals. In the healthy population, an upward shift in TSH distribution is seen with advancing age, a phenomenon that is considered part of normal physiology but inadvertently leads to over-diagnosis of subclinical hypothyroidism in older persons. There is no evidence that correcting such cases of subclinical hypothyroidism in the elderly confers any advantages on cardiovascular or neurocognitive function.45,48 In fact, a high-normal serum TSH concentration appears to be protective and has been shown to be associated with reduced mortality in older euthyroid individuals. 49 Furthermore, over-treatment in the elderly increases the risk of atrial fibrillation and osteoporosis, complications which are exceedingly common in this age bracket.14,50,51 Age-related reference intervals may thus be required, and an upper reference limit of up to 6 mU/L in the elderly may be more appropriate. 52 Likewise, a monitoring policy is advisable in older individuals with subclinical hypothyroidism and less stringent TSH targets may suffice in older LT4-treated individuals. 40
Secondary hypothyroidism
Secondary or central hypothyroidism due to hypothalamic or pituitary disease is characterized by deficient TSH production and as such serum TSH measurement is of no value in monitoring LT4 replacement. The primary therapeutic target is to maintain serum FT4 concentration in the upper half of the reference interval, 40 an approach which has been shown to improve metabolic parameters such as body weight and lipid profile. 53
Pregnancy
Uncorrected gestational hypothyroidism carries an increased risk of adverse pregnancy outcomes including miscarriages and low birth weight.46,54–56 Women with hypothyroidism require an increase in LT4 dose on conception since thyroxine requirements increase in pregnancy. This requirement is most critical in the first trimester when the developing fetus wholly depends on maternal thyroid hormone supplies for its optimal brain development. 3 Accordingly, international society guidelines recommend stringent gestational TSH concentration targets of < 2.5 mU/L in the first trimester and < 3.0 mU/L in subsequent trimesters.46,54 Hypothyroid women who are planning pregnancy should adjust their LT4 dose to attain normal thyroid status and on conception the dose should be increased by approximately 30% of the baseline dose, roughly equivalent to two days extra tablets weekly. 46 Further dose adjustments may be required to attain the recommended targets. It is noteworthy that almost half of women of child-bearing age established on LT4 have a TSH > 2.5 mU/L, indicating a high risk of high TSH in the first trimester. 56
Differentiated thyroid cancer
In differentiated thyroid cancer (DTC), the aim of thyroid hormone therapy is to correct postablative hormone deficiency as well as optimize outcomes via TSH suppression. TSH is a thyroid growth factor and high TSH levels stimulate malignant growth and may worsen prognoses in patients with DTC. 57 Studies show that LT4-induced TSH suppression improves outcomes in DTC patients with high risk malignancies, but this benefit is unproven for individuals with low-risk disease.58,59 International guidelines recommend that serum TSH concentrations should be suppressed in all patients in the immediate postablative period and then subsequent targets determined according to the postablation risk stratification.60,61 Patients with a satisfactory treatment response can be maintained at a low-normal TSH concentration (0.3–2.0 mU/L). A serum TSH concentration in the range 0.1–0.5 mU/L is recommended for individuals with indeterminate response whereas patients with high risk or incomplete response should aim for serum TSH concentrations < 0.1 mU/L.60,61 These therapeutic targets must, however, be balanced against the risk of harm from iatrogenic hyperthyroidism in individual patients. 59
Patients with abnormal TSH concentration
Prevalence
Cross-sectional studies show that 30–50% of LT4 users have an abnormal serum TSH concentration either due to under-treatment or over-treatment.
3
These figures remain constant over time and have been reported across all ages and in different health-care systems including community as well as specialist clinic settings6,7,12,14,62–66 (Figure 2). For example, abnormal serum TSH concentrations were detected in 40% of participants on thyroid medications (n = 1525) in the Colorado thyroid disease survey,
6
while a third of individuals with self-reported thyroid disease (n = 820) in the NHANES III survey had thyroid dysfunction.
7
In another American study, only 43% of thyroxine-treated patients aged over 65 years were biochemically euthyroid.
62
Data from more recent cohorts are comparable.12,14,64–66 An analysis of a large dataset of thyroxine users in Tayside showed that 38.4% had out of range TSH results,
14
findings that were similar to general practice data from South Wales.
12
In the Welsh study, the frequency of thyroid dysfunction remained constant over a median duration of six years despite regular annual testing.
12
However, hospital clinic data from Spain demonstrated that thyroid status can be improved in patients with inadequate therapy by optimizing the dose and administration of LT4.
63
Inadequate LT4 administration was also a factor in a Brazilian cohort with suboptimal LT4 replacement.
64
For example, about half of the cohort did not receive appropriate instructions on avoiding simultaneous intake of other medications with LT4.
64
Thus, taken together, these studies suggest that thyroid hormone under-replacement or over-replacement is prevalent and challenging to manage but could be overcome, at least for some patients, by optimizing the dose and administration of LT4.
Prevalence of abnormal TSH in LT4 treated patients.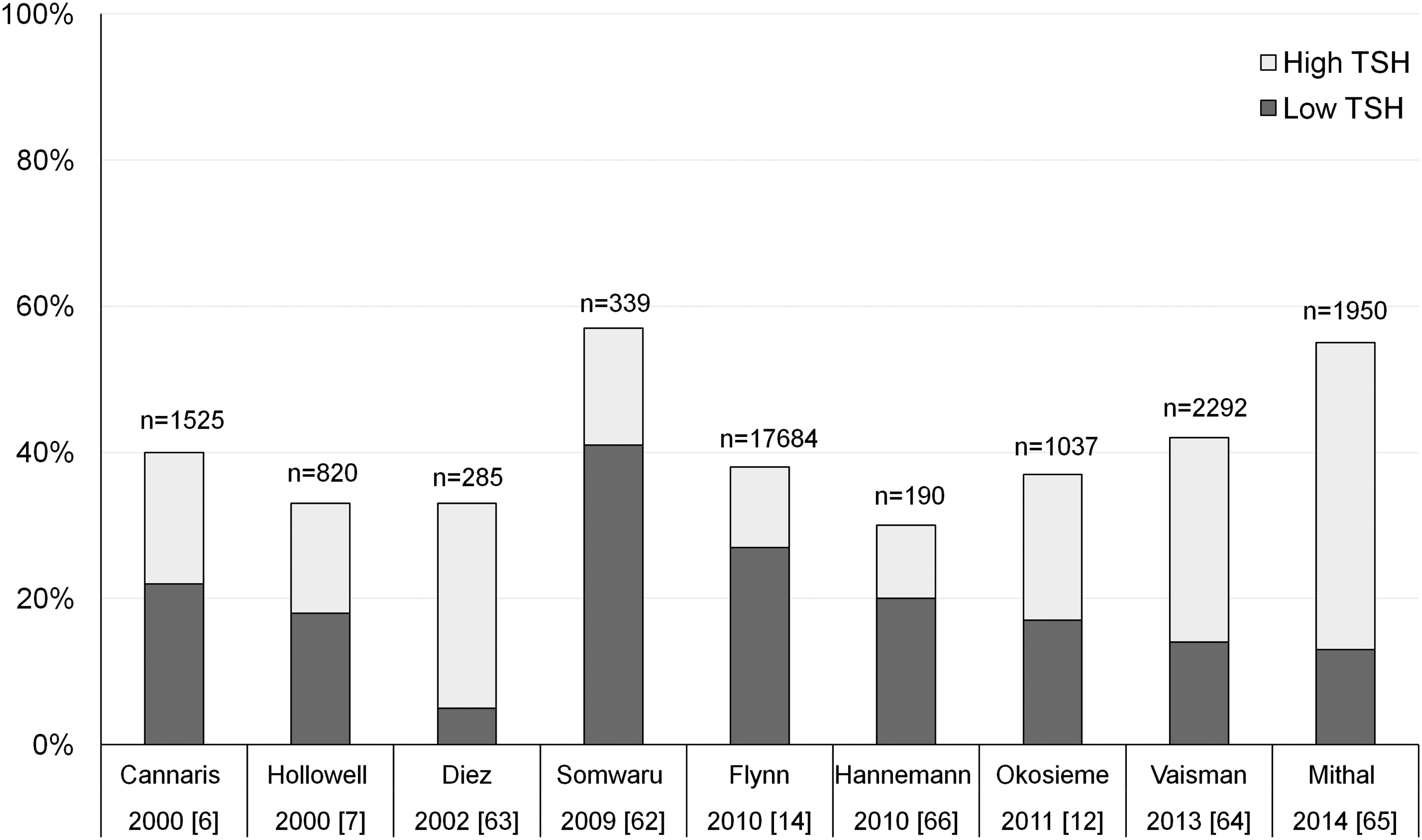
Impact of over-treatment
Over-treatment of hypothyroidism has adverse consequences. Thyrotoxicosis due to over-treatment increases the risk of atrial fibrillation, osteoporosis and fractures.14,50,67–69 Flynn et al. showed that LT4-treated patients with a suppressed serum TSH concentration (<0.04 mU/L) had an increased risk of cardiovascular disease, arrhythmias and fractures compared to those with a serum TSH value within the laboratory reference interval. These risks were not present for patients with a low but non-suppressed serum TSH concentration (0.04–0.4 mU/L). 14 In a register-based time-resolved cohort analysis of over 8000 patients with hypothyroidism, the risk of osteoporotic fractures was shown to be related to the cumulative duration of treatment-induced hyperthyroidism. 70 Furthermore, a case-controlled study in older adults showed a significant dose-related association between LT4 use and the risk of fractures (adjusted odds ratio 1.88, 95% confidence interval 1.71, 2.05). 50 Taken together, these studies would suggest that the adverse effect of over-treatment, at least on bone health, is dependent on the duration and extent of such over-treatment.
Impact of under-treatment
Hypothyroidism, on the other hand, exerts well-recognized adverse effects on lipid metabolism and cardiovascular function, some of which are reversible following adequate thyroid hormone replacement.10,71 Negative effects of thyroid hormone deficiency on vascular function include increased systemic vascular resistance, diastolic hypertension, central arterial stiffness and endothelial dysfunction. 10 For patients on thyroxine with a raised serum TSH concentration, the risks were at least as great as they were for those individuals with a suppressed TSH, with a two-fold increased risk of cardiovascular disease and arrhythmias. 14 The evidence of risk for endogenous subclinical hypothyroidism is less clear. 10
Management of patients on LT4 with persistently high TSH
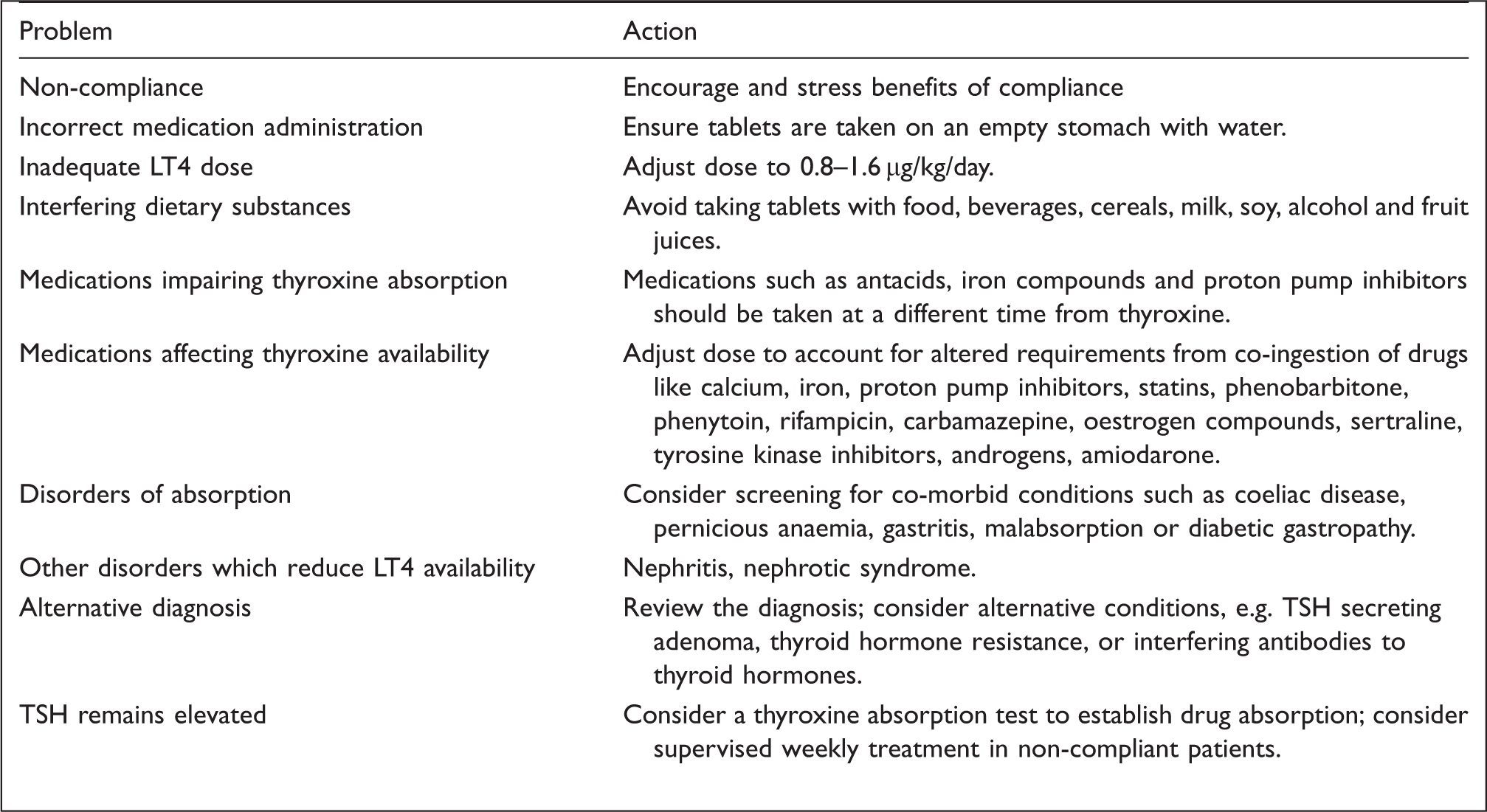
Approach to the levothyroxine-treated patient with persistent TSH elevation.
Medication dosage
It is important that the dose of LT4 is adequate for the patient’s body weight, i.e. 0.8–1.6 µg/kg/day. Infants and children require higher doses than adults and the elderly may require even less as thyroxine requirements decline with advancing age. 73 In addition, premenopausal women have higher thyroxine binding globulin concentrations and therefore require higher doses than men or postmenopausal women. 73 Relatively higher doses of LT4 are also needed for patients who have undergone total thyroidectomies compared to those with residual thyroid tissue following partial thyroidectomy. 73 Other causes of increased requirements include concomitant medication use and the presence of co-morbidities (Box 2).
Medication administration
LT4 absorption is enhanced in the fasting state and its availability is reduced by most food and beverages including milk, fruit juices, tea, coffee, alcohol and soy products. Thus, clear instructions should be given for LT4, indicating that it should be taken on an empty stomach, with water, at least an hour before a meal. 74 The tablets should ideally be administered first thing in the morning or at bedtime depending on convenience. Controlled trials have shown that fasting LT4 administration regimens, whether prebreakfast or bedtime, are more effective than non-fasting regimens.75–77 Although LT4 is conventionally administered daily, it can be taken at longer intervals due to its elimination half life of approximately seven days. A handful of small controlled trials have confirmed the efficacy and safety of weekly thyroxine treatment, at doses of 700–1000 µg weekly.78–80
Medication adherence
There is sparse published information on LT4 adherence rates. One survey reported that 22% of LT4-treated patients admitted to non-compliance, 81 while in another study, non-compliance was identified as a contributory factor in 82% of LT4 users with persistently high serum TSH concentrations. 82 Inconsistent compliance will cause fluctuations in serum TSH values and to avoid over-treatment it is vital that compliance is addressed before dose increases in patients with elevated TSH. One clue to non-compliance is a discordant serum thyroid hormone pattern, e.g. high TSH and high FT4 concentrations, which are indicative of pretest medicating in the non-compliant patient. Optimal strategies to improve compliance are still unproven. An educational booklet did not improve adherence in a general practice setting. 83 Potential contributing factors such as busy schedules or memory impairment should be sensitively addressed and timing of medications should be adjusted to suit individual needs. Supervised weekly dosing may be considered in difficult cases.
Co-morbid conditions
LT4 availability may be affected by a variety of conditions which reduce its absorption or increase its clearance (Box 2). Notable examples include coeliac disease, autoimmune gastritis and diabetes mellitus, conditions which often co-exist with hypothyroidism.3,84–87 Coeliac disease and gastritis impair LT4 absorption, while diabetes exerts variable effects on LT4 requirements via multiple mechanisms including obesity, gastroparesis and polypharmacy. 87 Patients with nephritis have increased thyroxine requirements due to urinary losses of free and protein-bound thyroid hormones. 88 Screening for these disorders should be considered even in asymptomatic LT4 users with unexplained high serum TSH concentration, since they may be clinically silent or masked by features of hypothyroidism.
Concomitant medications
Thyroxine requirements may be affected by concomitant ingestion of medications; the most common examples of which are: iron compounds, antacids, proton pump inhibitors and statins 89 (Box 2). Increased LT4 requirements have been reported in hypothyroid patients receiving tyrosine kinase inhibitors used to treat solid and haematological malignancies. 90 The precise mechanisms by which these molecular-targeted therapies modify thyroid function are still unclear but possibly include induction of a destructive thyroiditis, impairment of iodine uptake and reduced thyroid peroxidase synthesis. 90
Tablet stability and potency
Different tablet preparations may exhibit minor differences in bioequivalence which may have clinically relevant effects when switching preparations. 91 As much as possible, the same preparation from the same manufacturer should be used and the clinician should be made aware when a product switch occurs. Brand or named supplier prescribing is not considered necessary in the UK but may be considered in exceptional cases of difficult control or intolerance to generic preparations. 92
The euthyroid symptomatic patient
Alternative causes of ill-health in the euthyroid LT4-treated patient.
Yet it is apparent that despite a thorough evaluation of all physical and psychosocial factors some individuals will continue to suffer symptoms which cannot be explained by a plausible alternative aetiology. The management of such individuals is challenging and frequently frustrating to both clinician and patient alike. An open, empathic and patient-centred approach is essential. Symptoms should be acknowledged rather than dismissed even where these symptoms are discordant with biochemical thyroid status. Recent international society guidelines by the European Thyroid Association (ETA) and the British Thyroid Association (BTA) would now consider a trial of combination therapy with LT4 and LT3 in individuals who unambiguously fail to respond to LT4 alone.92,93 Such a trial should be undertaken under strict specialist supervision with clear communication of the uncertain risks and unproven benefits of combination therapy and should be discontinued if there is no evidence of response. 92
LT3 and LT4 combination therapy
The LT3 debate
The role of combined LT3 and LT4 therapy is contentious and has continued to generate debate. 94 Proponents of combination therapy argue that LT4 monotherapy fails to meet the needs of a proportion of patients, many of whom respond better to LT3. Furthermore, some individuals express a preference for combination therapy, whether in anecdotal accounts or in controlled trial settings.95–99 These observations are supported by experiments in thyroidectomized rats which show that adequate tissue T3 concentrations are only attained when LT3 is administered in combination with LT4. 100 In addition, T3 is the metabolically active hormone which exerts effects at tissue level. Thus, the efficacy of LT4 will depend on its efficient conversion to T3, and it is plausible that individuals who do not respond to LT4 lack the capacity to generate T3 at the tissue level whether for genetic or other unexplored reasons.
Arguments put forward to defend LT4 monotherapy include the fact that the vast majority of hypothyroid patients appear satisfied with LT4, the safety of which is supported by decades of clinical experience. In contrast, long-term safety data on LT3 are lacking, and LT3 formulations that mirror human physiology are unavailable. Furthermore, findings in thyroidectomized rats are not applicable to humans who exhibit more efficient peripheral synthesis of T3 than rodents and maintain adequate tissue T3 concentrations on LT4 alone post-thyroidectomy. 101 Lastly, dissatisfaction with LT4 may arise for a variety of reasons other than the hypothyroid state including the presence of co-morbid conditions, the natural bias towards thyroid testing and diagnosis in inherently polysymptomatic individuals and the inevitable effect of the hypothyroid disease label on symptom awareness.102,103
Randomized controlled trials
Summary of key outcomes in LT3 + LT4 vs. T4 trials.
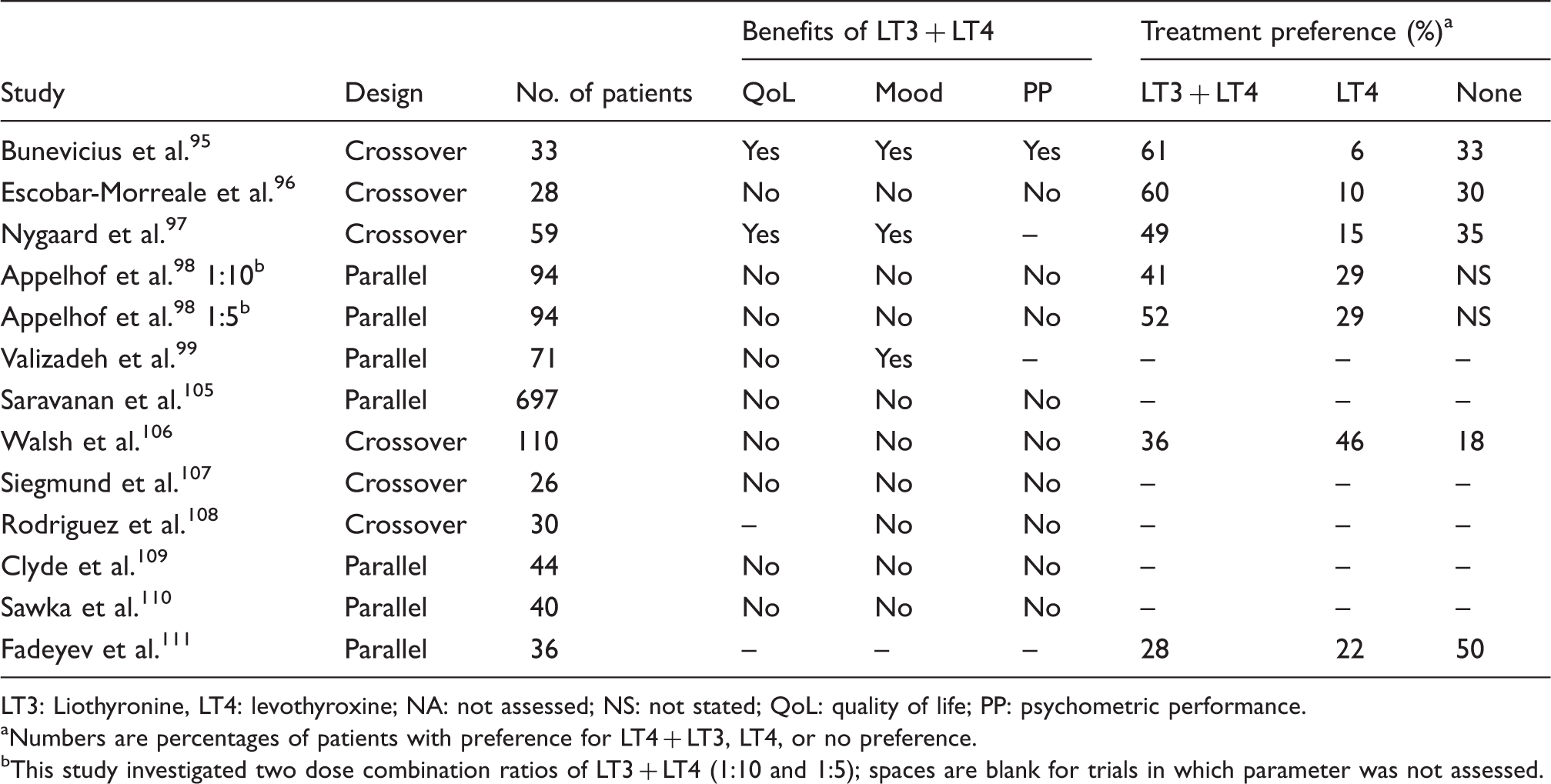
LT3: Liothyronine, LT4: levothyroxine; NA: not assessed; NS: not stated; QoL: quality of life; PP: psychometric performance.
Numbers are percentages of patients with preference for LT4 + LT3, LT4, or no preference.
This study investigated two dose combination ratios of LT3 + LT4 (1:10 and 1:5); spaces are blank for trials in which parameter was not assessed.
International society recommendations
A number of international society guidelines and position statements have, in recent years, addressed the role of LT3 therapy in hypothyroidism.40,92,93,116 Although all recommend against the routine use of LT3, there is acknowledgement that not all individuals are satisfied with LT4 alone. The proportion of patients disaffected by conventional treatment is still unclear, and the approach to their management is evolving. In a clinical practice survey in the United States for example 3.6% of practitioners indicated that they would prescribe LT3 to symptomatic LT4 users who were biochemically euthyroid. 117 The ETA and BTA would consider a trial of LT3 therapy under strict specialist supervision after a careful evaluation for an alternative aetiology and a period of chronic disease and lifestyle support.92,93 Such a therapeutic trial would be preceded by an open discussion of the uncertainty of the risks and benefits of the treatment and discontinued if benefit is not evident.92,93 The American Thyroid Association would also consider a trial of LT3 in individuals who have unambiguously failed to respond to LT4 but only in the setting of a formal clinical trial supported by appropriate governance safeguards. 40 However, the authors of the guidelines highlight the ethical responsibility inherent on clinicians to avoid potentially harmful unapproved therapies where there are safe and tested conventional therapies. 40 Finally, there is universal agreement that further controlled trials are needed.
Common genetic variations in deiodinases
One group of individuals who may exhibit a variable response to LT4 therapy are those with genetic variations in the deiodinase and transport proteins that facilitate intracellular thyroid hormone delivery and action.118–120 In a retrospective study, Panicker et al. 121 observed an association between the Thr92Ala polymorphism in the D2 deiodinase gene and impaired psychological well-being in LT4-treated patients. 122 Furthermore, those patients with the polymorphism, who constitute about 16% of the population, had an enhanced response to combination T4 + T3 therapy. Since the D2 deiodinase is the main deiodinase present in the brain, these findings would suggest that T3 delivery to the brain might play a role in the response to LT4 therapy. Another study, albeit in a much smaller cohort, did not confirm an association between the Thr92Ala substitution and well-being or response to combination therapy. 121 Thus, adequately powered prospective studies will be needed to clarify the role of common genetic variations in the deiodinases in the response to thyroid hormone therapy.
Conclusions
Synthetic LT4 remains the treatment of choice in hypothyroidism supported by extensive clinical experience on its efficacy and safety. For the vast majority of patients, a daily dose of LT4 transforms a debilitating and potentially fatal condition into one that is easily treatable. Yet for a minority, a state of well-being on LT4 appears an impossible ideal. The percentage of individuals disenfranchised with conventional therapy is unclear but will include a proportion with unrelenting symptoms and discordant serum biochemistry. Such individuals provide a powerful opportunity to improve our understanding of thyroid hormone action, but the approach to their management must remain rooted in scientific evidence and principles of good medical practice. While there is insufficient evidence to support routine combination therapy, a trial may be considered in settings where the efficacy and safety of such therapy can be audited. Future research should now seek to understand whether there are characteristics that distinguish subsets of individuals that benefit from combined therapy including genetic features and baseline psychological morbidity. Lastly, efforts should be channelled towards improving drug delivery through the design and production of LT3 formulations that best mirror human physiology.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
OKE.
Contributorship
All authors contributed equally to this review.