
Abstract
γ-glutamyltransferase plays a key role in the synthesis and metabolism of extracellular glutathione, a major antioxidant in several defence mechanisms in the body. γ-glutamyltransferase is affected by environmental and genetic factors, and is raised when there is depletion of glutathione. Hence, it is a marker of oxidative stress. There is robust evidence that γ-glutamyltransferase even when values are within the reference interval is associated with increased cardiovascular and all-cause mortality in both sexes, in normal subjects and subjects with coronary artery disease, in the middle-aged and the elderly after adjusting for confounding factors. γ-glutamyltransferase even within the reference interval is associated with future presentation of type 2 diabetes, and the longitudinal increase in γ-glutamyltransferase activity is associated with increased risk of type 2 diabetes and cardiovascular mortality. γ-glutamyltransferase is associated with cardiovascular risk factors and metabolic syndrome. It has a prognostic value after a previous acute myocardial infarction and may be an indicator of adverse outcome in acute coronary syndromes and other chronic cardiac disorders. There is limited data about γ-glutamyltransferase and any association with peripheral arterial disease and also whether knowing γ-glutamyltransferase activity improves cardiovascular risk prediction beyond conventional risk factors. γ-glutamyltransferase is present in atherosclerotic lesions in the coronary and carotid arteries, and has a prooxidant role leading to the production of reactive oxygen species and atherosclerosis. Current reference intervals for γ-glutamyltransferase are inappropriate and need to be addressed. Some laboratories still use non- International Federation of Clinical Chemistry methods for estimation of γ-glutamyltransferase which are associated with lower results. Such laboratories should review their method and consider changing to the International Federation of Clinical Chemistry method.
Keywords
γ-glutamyltransferase
γ-glutamyltransferase (GGT, EC 2.3.2.2) is a glycoprotein with a molecular weight of 68 KDa consisting of two proteins. The larger chain has a molecular weight of 46 KDa and the smaller chain 22 KDa.
GGT is found not only in the liver but also in several other organs including kidney, lung, pancreas and vascular endothelium. The primary role of cellular GGT is to metabolize extracellular reduced glutathione (GSH), enabling precursor amino acids to be assimilated and re-utilized for synthesis of intracellular GSH. Serum GGT is therefore a marker of oxidative stress which leads to depletion of GSH.1,2
The γ-glutamyl cycle
The γ-glutamyl cycle accounts for most of the de novo synthesis of GSH (L-γ-glutamyl-L-cysteinyl-glycine), a major antioxidant involved in several defence mechanisms in the body.
This cycle is also proposed as an amino acid transport system (Figure 1). Once there is sufficient cysteine, synthesis of GSH can proceed and is a two-step process, which initially involves formation of γ-glutamyl-cysteine from glutamic acid and cysteine catalysed by γ-glutamyl-cysteine synthetase (GCS). GSH is then synthesized from γ-glutamyl-cysteine and glycine catalysed by GSH synthetase.
The γ-glutamyl cycle (Obtained permission and adapted from Taylor and Francis Group LLC Books.).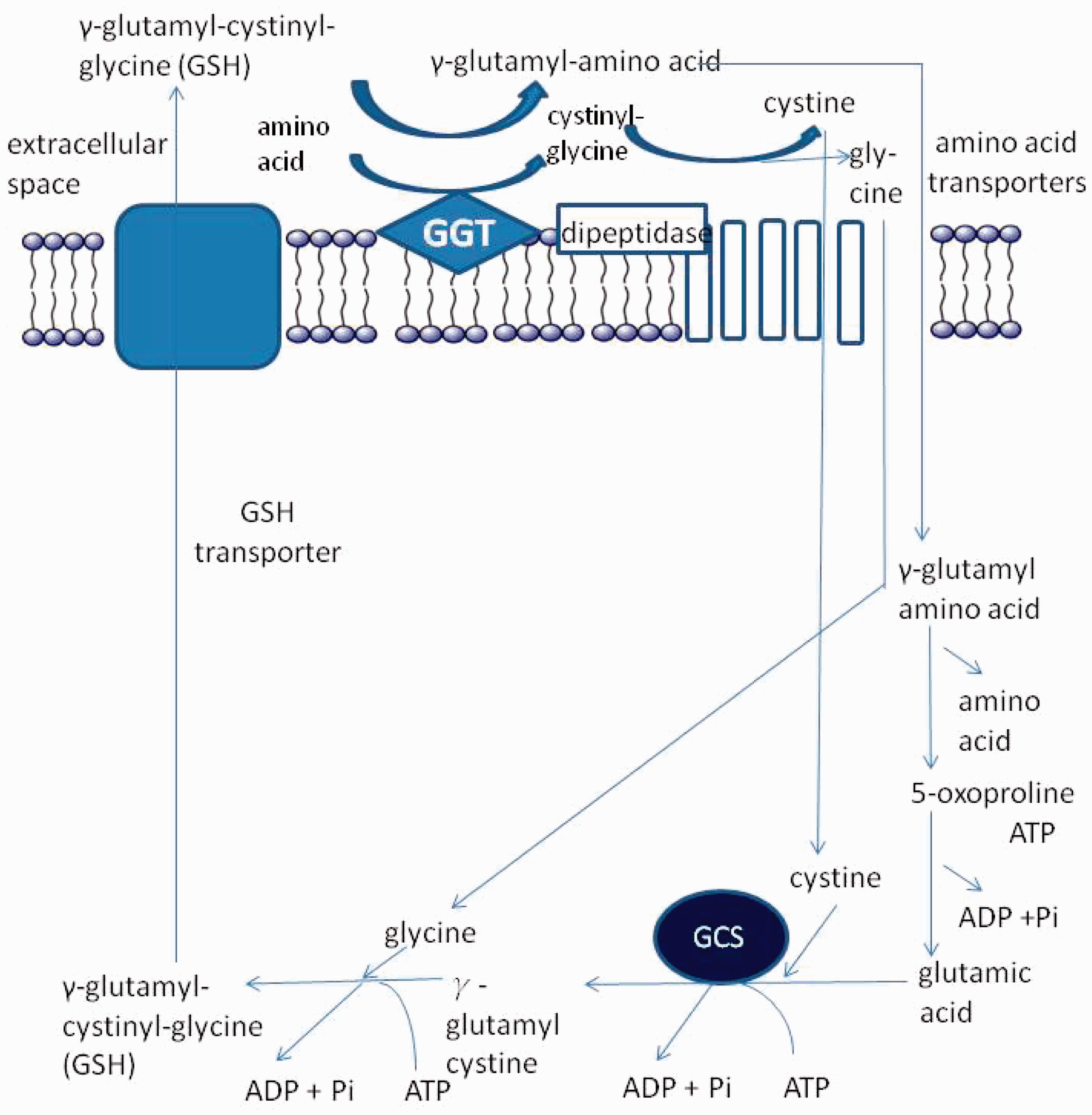
The cysteine required for GSH synthesis is obtained by most cells through degradation of circulating GSH catalysed by membrane bound GGT. The γ-glutamyl moiety of GSH is transferred by GGT to another amino acid forming the γ-glutamyl amino acid that is transported into the cell and metabolized to release the amino acid and 5-oxoproline, which can then be converted to glutamate.
Genetic heritability of GGT
Raised serum GGT activity has been reported in a family consisting of a number of healthy members in the absence of alcohol or drug abuse, liver disease and with other normal liver function tests (LFTs). 3 The GGT elevations were in the GGT-2 fraction. This was attributed to a predominantly autosomal dominant inheritance. Unexplained elevation of serum GGT activity should be an indication to investigate other family members to exclude a genetic inheritance, which if confirmed, can be reassuring and avoid unnecessary investigations.
The importance of genetic and environmental factors to variations in LFTs was investigated in 290 same sex twins. 4 Heritability was estimated using structural-equation analyses before and after adjustment for alcohol and body mass index (BMI). The effects of genetic factors on LFTs account for a third to two-thirds of the variation in elderly twins aged 73 to 102 and are equal for both sexes. 4 This was also confirmed by another study looking at twins in Australia, which concluded that both genetic and environmental factors affect liver enzymes. 5
This review will aim to highlight recent developments and outline our current understanding about GGT as a cardiometabolic risk marker.
GGT as a cardiometabolic risk marker
Serum measurement of serum GGT activity was introduced in the 1970s as a marker of alcohol intake and hepatic dysfunction. Conigrave et al. was the first to report that raised serum GGT activity was associated with cardiovascular (CV) mortality when working on alcohol-related research. 6
As a cardiometabolic risk marker, GGT must meet stringent criteria. 7 It must measure a single specific entity, either physiological or pathological, and offer additional information over currently used determinants. It must also add to the clinical assessment of a specific problem and correlate with known CV risk factors. It must be applicable to men and women, of all ages and of all ethnic groups. The assay must be easily standardized, and have high sensitivity and specificity and be readily automated. It was concluded that GGT appears to have met all accepted criteria as a cardiometabolic risk marker. 8
Cardiovascular mortality
Overview of the main prospective studies assessing the association between increased serum GGT activity and increased CV events.

AMI: acute myocardial infarction; GGT: γ-glutamyltransferase; CAD: coronary artery disease; CHD: coronary heart disease; CV: cardiovascular.
Serum GGT activity was first reported to be associated with CV disease and all-cause mortality in the British Regional Heart Study. 9 The highest quintile of GGT activity (>24 U/L), which is within the reference interval was associated with significant increase in all-cause mortality, compared to the other lower quintiles where there was little difference in mortality in the first four quintiles. The increased CV mortality was more apparent in men with known coronary heart disease (CHD), while in men without previous CHD, the increased mortality was due to non-CV causes. An Austrian study also found that elevated serum GGT activity was positively associated with conventional CV risk factors, and the highest GGT activity quintile was associated with increased CV mortality, but no association for acute myocardial infarction (AMI). 10 A Finnish prospective study reported that CV mortality was higher in the 90th percentile GGT activity category compared to the 25th percentile, and the mortality was greater in subjects less than 60 years of age. 11 The authors reported that elevated GGT activity also contributed significantly to the estimated risk of CV mortality as determined by a new CV risk scoring system in clinical practice in Europe developed by the SCORE project group, independent of conventional CV risk factors. 11 However, compared with risk factors like smoking or cholesterol, the strength of association of serum GGT activity with CV mortality was modest, and also weaker than the risk of developing type 2 diabetes. 11 Meisinger et al. reported that GGT was a strong predictor of acute coronary events in apparently healthy men independent of other CV risk factors. 12 A British study also confirmed that serum GGT activity is a predictor of increased risk of stroke and CV mortality in apparently normal men with no evidence of previous CV disease or diabetes, and with stronger association in men aged <55 years. 13 GGT activity significantly predicted CHD outcomes especially in those individuals at low (<10%) and medium (10–19%) CHD risk over 10 years based on Framingham risk score. 13 Results of the British Women’s Heart and Health Study combined with a meta-analysis examining the association of GGT activity with incidence of CHD, stroke and combined outcome of CHD or stroke showed that GGT activity was associated with vascular events independent of alcohol intake. 14 In patients scheduled for coronary angiography, serum GGT activity was predictive of all-cause and CV mortality independent of established and emerging risk factors. 15 In the presence of angiographic coronary artery disease (CAD), GGT activity was predictive and similar to the entire cohort. GGT activity also predicted mortality among older twins after adjusting for potential confounders in a Danish study, which could be explained by environmental and developmental origins in both monozygotic and dizygotic twins. 16
GGT was associated with increased all-cause and CV mortality in men, particularly in the presence of hepatic steatosis. 17 Hepatic steatosis requires hepatic ultrasound to confirm the diagnosis and cannot be diagnosed on clinical examination alone. This would highlight the importance of performing an ultrasound in the presence of a raised serum GGT activity to not only confirm the diagnosis, but also for further risk stratification.
The association of GGT activity with risk of only stroke in Caucasians was observed by two groups.18,19 Serum GGT activity was significantly associated with stroke, and in particular haemorrhagic stroke with no gender difference. 18 In a Finnish study, GGT activity was associated with the risk of total and ischaemic stroke in both genders. 19 There was also a significant association between GGT activity and risk of intracerebral haemorrhage in men, and between GGT activity and subarachnoid haemorrhage in women. 19 Both studies suggested that raised GGT activity was purely a marker of excessive alcohol intake that was associated with increased stroke because excessive alcohol intake can lead to hypertension.
Stroke was one of the outcomes studied by Ruttman et al., 10 and their observations and conclusions regarding the relationship of stroke and GGT were not consistent with that of Bots et al. 18 and Jousilhati et al. 19 Raised GGT activity was significantly associated with haemorrhagic and ischaemic stroke in men but not in women. 10 The reason for the gender difference in stroke was not clear. The authors suggested that any association of a raised GGT activity with increasing trend of mortality, is unlikely to simply reflect the effects of alcohol because most studies have shown a ‘U’ or ‘J’ shaped relationship of alcohol drinking to CV20,21 and all-cause mortality, 22 and concluded that serum GGT activity was independently associated with CV mortality. 10
There is limited data about the association of serum GGT activity and mortality from CHD, stroke and overall CV disease in Asians. The data from one Japanese study showed a strong positive association of serum GGT activity with CV mortality in women in whom the prevalence of chronic drinkers is very low. 23 The authors did not find any significant relationship in men, unlike most other studies, largely in Caucasians, that did not report a gender difference. The reason for the gender difference is not clear, and the authors suggested that the difficulty in controlling for the effects of alcohol consumption in men might partly account for the gender difference. Further studies are required to clarify if serum GGT activity correlates with CV mortality in Japanese men.
Another Japanese study with 15-year follow-up also confirmed the association of serum GGT activity and CHD that was non-significant in men but significant in women. 24 However, there was no association with stroke in both sexes. The non-association with stroke is inconsistent with the findings of another Japanese study that reported a positive association between GGT activity and incidence of stroke. 25 The reason for this inconsistency is unclear, and it is possible that stroke includes aetiologically heterogeneous conditions with different fatality risk. Therefore, factors that influence stroke incidence may be different from those that influence death from stroke. Secondly, stroke is more common in Asia compared to Europe and the US, 26 and the prevalence of stroke subtype can be different in Asians and Caucasians. This may therefore lead to differences in association between GGT activity and stroke.
The association of GGT with stroke is still far from clear and requires further data to clarify differences if any, between Caucasians and Asians and differences in gender and stroke subtype.
The association of GGT activity and stroke in the presence of diabetes is unclear at present. While Bots et al. suggested that the association with haemorrhagic stroke was stronger in subjects without diabetes compared to diabetes, 18 this was not confirmed by another study. 27 This reported that there was no evidence that the presence of diabetes modified the strength of the serum GGT activity and CV and all-cause mortality relationship. 27 Kengne et al. also examined the predictive ability when GGT was added to a CV risk algorithm in subjects with and in subjects without diabetes. 27 Adding GGT to a model with conventional risk predictors, only marginally enhanced the prediction of CV disease in subjects both with and without diabetes.
A meta-analysis of seven prospective cohort studies consisting of 273,141 participants showed that serum GGT activity is associated with increased CV and all-cause mortality with no gender difference (Table 1). 28 Light to moderate alcohol intake (5 to 25 g/day) was significantly associated with lower CV and all-cause mortality as opposed to an increased mortality. 29 The predictive ability of GGT activity was higher in the presence of CHD independent of confounders. The robustness of serum GGT activity as an independent risk factor was reinforced by the relationship of GGT as a continuous variable (per log unit increase) with CV mortality. GGT does not appear to be associated with CV mortality in Asians, which could be due to the difference in the prevalence of non-alcoholic fatty liver disease (NAFLD); this is higher in the west; 30 34% in the USA, 31 compared to 16.1% in Korea 32 and 15% in China. 33 This could suggest that the metabolic syndrome and NAFLD might be the key to the association of raised serum GGT activity and CV and all-cause mortality. Most studies had no Asian populations. Further studies are required to clarify the relationship between serum GGT activity and CV mortality in Asian populations before these findings are generalized to all populations.
Several researchers have reported that serum GGT activity is associated with a higher mortality in subjects aged less than 60 years.10,11,13,34–36 However, recent reports in the elderly where the mean age was 70 years, suggest GGT may also be associated with increased CV and all-cause mortality.37,38 Hence, data in younger individuals were not available, and so do not exclude a stronger association in younger subjects.
Longitudinal increase in serum GGT activity and CV mortality
The longitudinal change in serum GGT >9.2 U/L over 7 years compared to stable GGT (−0.7 to 1.3 U/L) was significantly associated with an increase in CV mortality, even when values were within the reference interval, in men with less pronounced effects in women, and independent of baseline GGT activity. 36
CHD and implications of measuring serum GGT activity in clinical practice
Recent studies have given us greater insight into the role of GGT in CHD and its implications in clinical management.
Serum GGT activity is not only associated with higher CV mortality but also has a prognostic value after a previous AMI; no such association was observed in the absence of a previous AMI. 39 In a prospective study of 469 consecutive subjects with angiographically proven CAD, serum GGT activity showed an independent prognostic value after adjustment for confounding factors. 39 Coronary revascularization abolished any prognostic value of GGT activity, probably counteracting the possible influence of GGT on plaque stabilization.
The same authors published a similar prospective study in subjects undergoing angiography with documented CHD to determine the prognostic value of GGT, CRP and fasting glucose. Serum GGT activity showed an independent prognostic value after adjustment of confounding factors. 40 Patients having GGT >25 U/L, CRP >8 mg/L and fasting glucose >6.6 mmol/L had the highest mortality of 26.6% vs. no event or 2.7% with no or only one risk factor (P < 0.0001).
In patients presenting with acute coronary syndrome (ACS), serum GGT was found to be an independent predictor of major adverse cardiac events (MACE). 41 Patients with serum GGT <23 U/L had significantly fewer MACE compared to patients with GGT >23 U/L.
The measurement of GGT can be a useful marker in the follow up of patients with coronary artery ectasia (CAE), a condition characterized by localized or diffuse non-obstructive lesion of the epicardial coronary arteries with a dilated lumen exceeding 1.5-fold of adjacent segment that is associated with high mortality. 42 GGT activity was significantly higher in patients with CAE compared to its activity in controls (P < 0.001). The authors suggested that further studies are required before concluding that measurement of serum GGT can be used as a follow-up marker in patients with CAE.
Coronary artery calcification (CAC) is a marker of atherosclerotic plaque burden and is an independent risk factor for CAD. In a prospective study of 272 patients, those subjects in the higher GGT quartiles had an elevated CAC score (P < 0.001), and were predominantly males with increased CV risk factors. 43 The authors concluded that serum GGT was an independent risk marker of CAC.
Serum GGT activity has also been associated with impaired coronary microvascular function leading to reduced coronary flow reserve (CFR), an independent predictor of subsequent cardiac events, in patients with dilated cardiomyopathy. 44 After adjusting for potential confounders, Ciftci et al. found that GGT activity was a good predictor of low CFR even in normal subjects without concomitant risk factors. 45
GGT has also been shown to be a predictor of adverse outcomes in patients with ST-segment elevation myocardial infarction (STEMI) undergoing percutaneous coronary intervention (PCI).46,47 The inpatient mortality and MACE rates were significantly higher in subjects with STEMI who underwent PCI with serum GGT >37 U/L (7.2% vs. 1.7%, P < 0.001). 46 Serum GGT >37 U/L was identified as an effective cut-off point in STEMI for inpatient CV mortality (area under the curve = 0.71, CI 0.59–0.82, P < 0.001). 46 There were, however, no differences in the long-term adverse outcomes between the two groups.
In patients with STEMI who underwent a PCI, the phenomenon of ‘no-reflow’ is defined as the unsuccessful restoration of epicardial coronary artery patency leading to no improvement in tissue perfusion. Increased serum GGT across the tertiles was associated with higher number of patients with such a ‘no-reflow’ phenomenon and one-year mortality rates. 47 Measurement of serum GGT may therefore be useful in identifying high-risk patients with STEMI undergoing PCI.
Future development of type 2 diabetes
Overview of the main prospective studies assessing the association between increased serum GGT activity and increased incidence of type 2 diabetes.

GGT: γ-glutamyltransferase; CARDIA: coronary artery risk development in young adults.
There was an increased risk of type 2 diabetes, associated with increasing serum GGT activities with graded response, even if activities were within the reference interval in British, 48 Finnish, 49 German 50 and Chinese 51 prospective studies after adjustment for confounding factors. Unlike in men where obesity was associated with diabetes irrespective of whether GGT was below or above the median, in women obesity was more strongly associated with diabetes when GGT was equal or greater than the median. 50 The Coronary Artery Risk Development in Young Adults (CARDIA) study, a longitudinal study to assess the impact of lifestyle and other factors on the evolution of CHD risk factors during young adulthood, showed GGT values even when within the reference interval were a predictor of diabetes and hypertension that increased across the quartiles. 52 Furthermore, the finding of a GGT activity within the reference interval predicted the future risk of microalbuminuria in subjects with diabetes or hypertension in the CARDIA study in young white and black men and women. 53 Serial measurements of serum GGT activity could therefore be useful to predict the risk of complications in diabetic patients.
A prospective study in healthy Korean men also confirmed a strong graded relationship between GGT activities at baseline and the incidence of diabetes. 54 The effects of age and BMI for diabetes risk were different depending on the baseline GGT concentrations. Among those individuals with a GGT activity in the low end of the reference interval, the associations of age and BMI with the development of diabetes were small, but among those with GGT activities in the higher end, or elevated, the associations of age and BMI were very strong. However, both the CARDIA study 52 and the Finnish study 49 failed to show an interaction between GGT and age, which could be either due to chance, ethnic differences or leanness of Korean men.
Raised serum GGT and alanine aminotransferase (ALT) activities have been shown to be associated with type 2 diabetes by several researchers.55–61 In one report, in order to determine if GGT and ALT activities are independent predictors of type 2 diabetes or merely surrogate markers for fatty liver, non-diabetic subjects without fatty liver or liver dysfunction confirmed by ultrasonography were studied. 62 The authors reported that increased serum GGT and ALT activities are independent and additive risk factors for development of future type 2 diabetes in subjects without fatty liver or liver dysfunction.
A cross-sectional study from the third National Health and Nutrition Examination Survey (NHANES) data showed that increased BMI was not associated with prevalent diabetes when serum GGT activity was towards the low end of the reference interval. 63 However, a raised BMI was associated with prevalent diabetes in subjects with serum GGT activities towards the high end of the reference interval, suggesting that obesity itself may not be a sufficient risk factor for type 2 diabetes, but that in addition, there is a strong interaction between serum GGT activity and obesity with the risk for developing diabetes. 63 This finding is consistent with the three earlier prospective studies that investigated GGT activity and BMI groups.49,52,54 A possible explanation for this is that obese individuals with GGT activities in the high end of the reference interval already have subclinical pathological changes attributable to obesity, whereas individuals with activities in the low end are at an earlier stage of pathogenesis.
A recent report from China suggests that the association between raised GGT activity and diabetes could be due to β-cell dysfunction as a result of the raised GGT in young obese subjects. 64 Measurement of GGT activity might therefore be a simple biomarker of early insulin secretion deficit in type 2 diabetes especially in young obese subjects.
Longitudinal increase in GGT and type 2 diabetes
The association of an increase in serum GGT activity with the development of future type 2 diabetes has also been investigated. An unchanged GGT activity, or an increased GGT activity of 5 U/L over three years, even if values remain within the reference interval, compared to a fall in GGT activity of >5 U/L over a similar period, is associated with a risk of type 2 diabetes, independent of baseline GGT after adjusting for confounding factors. 65 This was based on an intraindividual biological variability of GGT of 12.2%. 66 A Japanese study also reported that an increase in GGT activity of >1 U/L, over a period of three years, was a risk factor for type 2 diabetes, impaired fasting glucose, raised triglycerides and hypertension after adjustment for confounding factors and baseline GGT activity. 67
GGT and mortality in known type 2 diabetes
Reports about mortality associated with raised serum GGT activity in known type 2 diabetic subjects are not consistent. While some studies reported increased CV mortality in diabetic subjects,68,69 one study observed only an increase in all-cause mortality but not CV mortality. 70 In contrast, another did not observe a difference in all-cause and CV mortality in diabetic and non-diabetic subjects, and suggested that GGT activity may not enhance CV risk prediction based on traditional risk factors in subjects with and without diabetes. 27
Peripheral arterial disease
The data regarding serum GGT activity and peripheral arterial disease (PAD) are very limited. In a cross-sectional study, serum GGT activity was positively associated with PAD in men but not in women. 71 Another cross-sectional study could not confirm a linear relationship between serum GGT activity and PAD in type 2 diabetic subjects. 72 Further prospective studies are required to clarify the relationship between GGT and PAD.
CV risk factors
There has been considerable interest to determine the relationship of serum GGT activity and CV risk factors with a view to explain the increased CV-risk and mortality associated with increased GGT.
In a cross-sectional study of hypertensive subjects and age- and sex-matched controls, serum GGT activity was an independent predictor of the metabolic syndrome after adjustment for confounding factors 73 using the WHO criteria for the metabolic syndrome. 74 Serum GGT activity also predicted future metabolic syndrome in a prospective study defined by two different criteria: The International Diabetes Federation (IDF) and The American Heart Association/National Heart, Lung and Blood Institute (AHA/NHLB). 75 The odds ratio for the metabolic syndrome by both criteria increased across the GGT activity quartiles. Other prospective studies have also reported GGT as a predictor of metabolic syndrome.76–82 Scott in his editorial suggested that activities of serum GGT and aminotransferases are biomarkers of the metabolic syndrome. 83 A raised serum GGT activity at baseline was independently associated prospectively, with an increase in the index of homeostasis model assessment of insulin resistance (HOMA-IR).51,84
A cross-sectional study examining the relationship between serum GGT activity across all deciles, and serum CRP concentration, showed a positive relationship after adjustment for confounding factors. 85 In the CARDIA study, serum GGT activity predicted future CRP concentration measured after 15 years and concentrations of other biomarkers of inflammation and lipid peroxidation like fibrinogen, uric acid and F2-isoprostanes. 52 In a prospective study of Japanese men, serum GGT activity was an independent predictor of future development of hyperuricaemia, 86 which is a known CV risk factor.
A meta-analysis to evaluate the association between serum GGT and the risk of metabolic syndrome compared the top GGT category with the lowest category of nine prospective cohort studies and showed a pooled RR of 1.63 (CI 1.42–1.82, P < 0.000). 87 Most of the studies were from Asian populations, and hence further studies are required to generalize the findings. A meta-analysis of 13 prospective cohort studies to evaluate the association of serum GGT activity with hypertension comparing the top GGT category with the lowest showed RR was 1.94 (CI 1.55–2.43, P < 0.001). 88 The risk of hypertension increased by 23% (RR 1.23, CI 1.13–1.32, P <0.001) per 1 SD log GGT activity increment.
Longitudinal increase in GGT activity and metabolic syndrome
A longitudinal increase in GGT activity of 8 U/L or more was associated with an increased risk of metabolic syndrome compared to a reference group of men with a GGT activity of <17 U/L at baseline and with a change of −3 to 1 U/L (stable) over 1.7 years after adjusting for confounding factors. 82 It was concluded that a longitudinal increase in GGT activity even within the reference interval, may be an independent predictor for the metabolic syndrome. 82
Pathogenesis of GGT-related atherosclerosis and CV disease
Several epidemiological studies mentioned above suggested a relationship between circulating GGT and the evolution of atherosclerosis.
GGT has been shown to be present in the atherosclerotic lesions in coronary and carotid arteries.89–91 Histochemical studies have shown that GGT is present in CD68 macrophage-derived foam cells.92,93 GGT-positive cells were found to co-localize with immunoreactive oxidized LDL, 94 and catalytically active GGT was also detected in microthrombi adhering to the surface of atheromas. 95 It is not clear at present if GGT present in plaque tissue is an active participant in the disease or simply an epiphenomenon. Serum GGT arises mainly from liver but platelets 96 and granulocyctes 97 are thought to be additional sources of the circulating enzyme.
β-lipoprotein includes LDL, ILDL and VLDL but not HDL, and so the serum GGT associated with β-lipoprotein is an indicator of the LDL associated with GGT. The amount of serum GGT associated with β-lipoprotein is assumed to be directly proportional to total serum GGT activities in both controls and patients with CAD. 89 However, in subjects with CAD, the amount of GGT associated with the β-lipoprotein fraction is significantly lower. Furthermore, serum GGT activity is known to increase with age, and while serum GGT activity increases in the control group, by contrast significantly lower total serum GGT activity was detected in older CAD patients although the ratio between β-lipoprotein bound and total serum GGT activity remained constant. 98 The reasons for this are yet unclear.89,99 A possible explanation could be enhanced uptake of LDL–GGT complexes within atherosclerotic lesions leading to the appearance of significant deposits of active GGT within the lesions. 89 This could explain the correlation between higher serum GGT levels and adverse clinical outcomes reported in several epidemiological studies. This hypothesis would imply a role of GGT in plaque instabilization, as the prognosis of GGT disappears in patients undergoing revascularization and angioplasty is regarded as a procedure capable of stabilizing plaque tissue.89,90
GGT dependent generation of reactive oxygen species and other free radicals
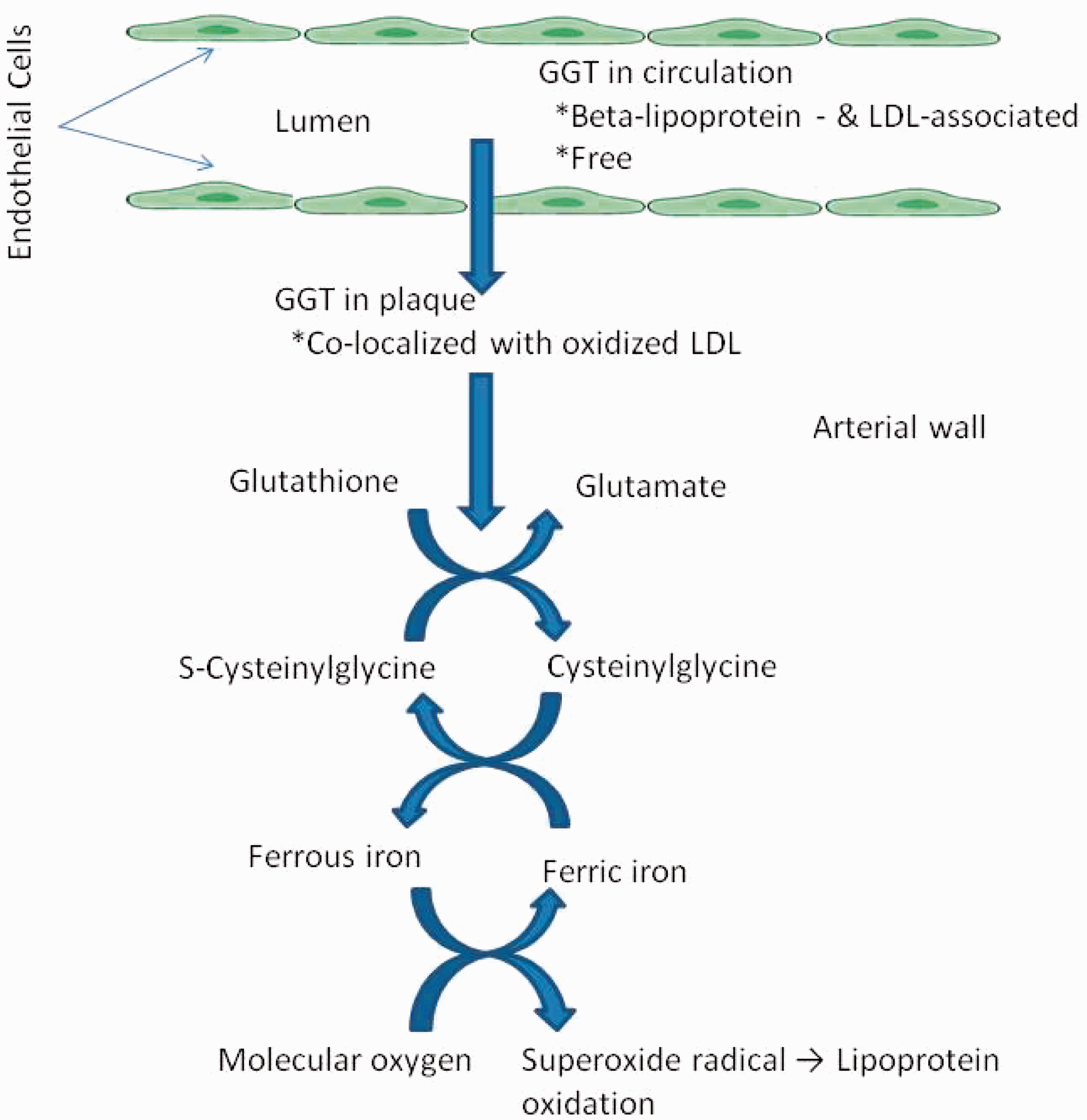
The primary role of cellular GGT is to metabolize extracellular reduced GSH enabling precursor amino acids to be assimilated and reutilized for intracellular GSH synthesis. GGT has a prooxidant role during the catabolism of extracellular GSH because of the generation of the more reactive thiol, cysteinyl-glycine, that reduces ferric ions to ferrous ions leading to production of reactive oxygen species (ROS) (superoxide and hydrogen peroxide).
100
Paradoxically, the ‘reducing’ properties of thiols are eventually turned into overall ‘oxidizing’ effects. The following reactions are believed to occur during the process of generation of ROS:





Oxidative reactions play an important role in plaque progression and instability, and the oxidation of LDL is the main event in the pathogenesis of atherosclerosis. Iron-dependent LDL may become critical when the progression of atheromas towards end-stage plaques leads to the liberation of iron ions, which mediate LDL oxidation by GSH hydrolysis products. This could explain how serum GGT correlates more with risk of fatal re-infarction than with occurrence of the primary episode of ischaemia, suggesting a possible role of iron reactions in late events such as plaque ulceration and vessel re-occlusion. The role of GGT in the formation of atheromatous plaque is shown in Figure 2.
101
Role of GGT in the formation of atheromatous plaque (Obtained permission from Turgot and Tandogan
101
).
The relationship between GGT, cysteinyl-glycine and oxidized LDL (o-LDL) with AMI in a case-cohort study nested within the EPIC-Potsdam cohort was investigated. 102 Although cysteinyl-glycine was positively associated with AMI-risk after controlling for risk factors, plasma concentrations of cysteinyl-glycine and o-LDL unexpectedly, accounted for only 2.3% of the association between plasma GGT activity and AMI risk. Considering the antioxidant properties of plasma, this would suggest that the hypothesized pathway has probably only a minor relevance in plasma, whereas GGT-mediated cleavage of GSH may still promote LDL oxidation in the intima.
The GGT-dependent prooxidant reactions have been shown to be important in several other processes such as the transduction of proliferative/apoptotic signals, due to their ability to interact with redox-sensitive regions of growth factor receptors, protein kinases and transcription factors. They also interact with critical targets in the intracellular signal transduction cascade, such as poly (ADP-ribose) polymerase (PARP), and the nuclear transcription factor NF-kB, which is the best known and studied redox-sensitive target.95,103
More recently, it has been shown that the oxidants and redox reactions have even wider implications in the diseased vessel wall like smooth muscle proliferation, activities of matrix metalloproteinases and their inhibitors, impairment of nitric oxide production and other functions that have a major effect on atherosclerosis and its progress that can lead to a fatal event. 89
Potential mechanisms involved in the association of GGT and type 2 diabetes
There are several mechanisms involved in the association of GGT and type 2 diabetes.
GGT is a marker of visceral fat, hepatic steatosis and hepatic insulin resistance. 104 Serum GGT activity is raised to maintain intracellular GSH when it is depleted, and is a marker of oxidative stress. Although serum GGT activity is conventionally regarded as a marker of liver disease, it has high activity in the kidney and other organs. 105 In addition, GGT leaks into the serum, possibly as a result of normal cell turnover and cellular stress. Thus, increased serum GGT activity may identify subjects with a persistent increase in oxidative and cellular stress. Furthermore, under physiological conditions, especially in the presence of Fe3+ and Cu2+, GGT is directly involved in the generation of ROS, and induce or perpetuate oxidative stress in cells.
Finally, subclinical inflammation as a manifestation of oxidative stress could play a role in the pathogenesis of diabetes. Fat accumulation can stimulate cytokine production, and inflammatory cytokines such as tumour necrosis factor-α and interleukin-6 can influence fatty-acid metabolism in the liver and predispose to formation of fatty liver. 106 The raised white blood cell count51,107 and serum CRP concentration108,109 associated with GGT suggest inflammation. Serum GGT activity could be raised before elevation of serum CRP concentration. 52
Potential mechanisms in GGT-associated increased CV mortality
The first mechanism mediated by GGT may be due to the CV risk factors mentioned above including CAC. The second mechanism is likely to be due to oxidative processes leading to LDL oxidation. The third proposed mechanism is subclinical chronic inflammation as shown by raised CRP concentration. 85 Leukotriene metabolism could be another possible mechanism behind the association of GGT and inflammation in CV disease. 110 Leukotrienes are lipid mediators of inflammation derived from the 5-lipoxygenase pathway of arachidonic acid metabolism. GGT uses leukotrienes as substrates. Recent studies have provided evidence of a strong genetic link between this pathway and an increased risk of AMI. 110
Measurement of GGT activity and performance in UK laboratories
Measurement of serum/plasma GGT is readily automated and the assay is undertaken in the majority of UK laboratories. Szasz published the first kinetic method for GGT using L-γ-glutamyl-p-nitroanilide (GGPNA) as substrate and glycylglycine as acceptor in 1969, 111 then 1974, 112 and again in 1976. 113 These are very similar and the latter two are based on the original publication. In order to circumvent the poor solubility of GGPNA, Persijn and van der Slik found that L-γ-glutamyl-3-carboxy-4-nitroanilide (GGCNA) was superior in terms of stability and solubility, and modified the original Szasz method, with results correlating with the original substrate. 114 The International Federation of Clinical Chemistry (IFCC) published a method for measurement of serum/plasma GGT activity at 30℃, 115 and later a revised method at 37℃ using GGCNA and optimized for stability, performance, substrate concentrations and use of NAOH, glycylglycine buffer and sample start. 116
When GGPNA is used as the substrate, GGT catalyses the transfer of a gamma-glutamyl group from the colourless substrate, GGPNA, to the acceptor glycylglycine, with production of the coloured product p-nitroaniline. The change in absorbance is directly proportional to GGT activity in the sample. In methods where GGCNA is the donor substrate, GGT catalyses the transfer of the γ-glutamyl group to the glycylglycine acceptor to yield 3-carboxy-4-nitroaniline and 5-amino-2-nitrobenzoate. The change of absorbance at 410 nm is related to the concentration of 5-amino-2-nitrobenzoate and is proportional to GGT activity.
The three key method groups for GGT using the different substrates that are used in the UK are: (1) GGCNA and acceptor glycylglycine recommended by the IFCC; 116 (2) the Szasz method modification by Persijn and van der Slik also using GGCNA 114 and (3) the original Szasz method using GGPNA and glycylglycine. 113 Roche Diagnostics have standardized the GGT method against both the IFCC method, 116 and the method by Persijn and van der Slik using GGCNA 114 on the Cobas Modular system. The Vitros dry slide method incorporates GGPNA as the donor substrate and glycylglycine as the acceptor, and calibrated with results traceable to the IFCC method. Beckman Coulter has different methods on their two main groups of analysers, with the IFCC method 116 on the AU series, and the original Szasz method using GGPNA and glycylglycine 113 on the Synchron CX series.
Most laboratories in the UK use the IFCC recommended method but some still use the Szasz method. The UK NEQAS returns in 2014 show that the Szasz method on the Roche Cobas Modular and the Beckman Synchron CX have about 10% and 15% negative bias, respectively, compared to the mean IFCC GGCNA method. However, as users are compared to their own method mean, the absolute differences in results can be difficult to identify. The Siemens Dade Behring is an IFCC method but still seems to have about 4% positive bias than the mean IFCC method, the precise reason for which is not clear. The EQA samples contain added GGT extracted from bovine intestine, and it may be that this form of GGT behaves differently under the conditions of the Siemens Dade Behring assay.
The finding of lower GGT results is clinically significant because of the associated lower risk for CV and all-cause mortality and lower risk for type 2 diabetes. This could lead to misinterpretation of results by clinicians and failure to give correct advice to reduce overall CV and diabetes risk. Similarly, high serum GGT results can overestimate risk and lead to unnecessary anxiety in patients and clinicians. It would therefore be prudent for laboratories to use only methods that are recommended by IFCC, so that measurements made in the laboratory are traceable to national and international standards of measurement, where possible, and results comparable between laboratories. 117
Implications to clinicians and the laboratory
It is clear from the above that serum GGT is more than a mere marker for hepatobiliary disease and excess alcohol intake. It has far reaching implications than initially recognized in the 1970s when the test was first introduced, and the research during the last 25 years has improved our understanding considerably about the significance of GGT.
The two immediate questions arising from this are firstly, how should the test be used by clinicians, and secondly, how should it be handled in the laboratory?
While it may seem reasonable for measurement of serum GGT to be used to assess total CV risk along with other conventional CV risk markers, there is limited evidence at present that measuring it improves CVD risk prediction beyond conventional risk factors.27,118 The strength of association of serum GGT with CV risk is only modest compared to smoking or cholesterol. 11 While serum GGT activity predicted CV outcomes in low and medium CHD risk based on Framingham risk score in one study, 13 it only marginally enhanced CVD prediction in subjects with or without diabetes in another study. 27 A recent cross-sectional study in Korea showed that measuring serum GGT activity could be useful in predicting CV risk. 119 The odds ratio for 10-year CV risk >20% was significantly increased across the GGT quartiles even after adjustment for confounders. 119 The role of measuring serum GGT in CV risk assessment at present is still not clear, and furthermore, it is not known whether this is more effective than conventional risk assessment.
Interpretation of serum GGT results should take into account any medication, notably anticonvulsants, that increase serum GGT activity. Raised serum GGT activities in patients receiving anticonvulsants without co-morbidities did not correlate with oxidized LDL, and hence could be ‘benign’. 120 However, there is no data at present about the long-term CV and all-cause mortality in patients with raised serum GGT activity due to anticonvulsant therapy.
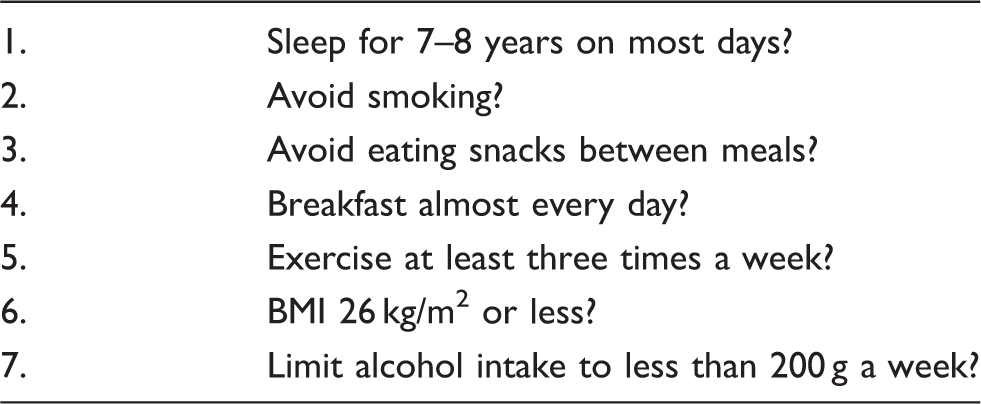
Questionnaire for estimation of lifestyle status based on Breslow’s life style index. 121
The association of serum GGT activity and incidence of diabetes would suggest that measuring serum GGT is easy and inexpensive, and could be useful in the prediction of diabetes in obese and high-risk individuals. It could also be useful in predicting complications such as microalbuminuria in known diabetic patients. 53
The value of monitoring of serum GGT activity in patients with both normal and raised values could be useful in patients as longitudinal increases in serum GGT of >9.2 U/L over 7 years, >5 U/L over 3 years and >8 U/L over 1.7 years are associated with increased CV mortality, 36 increased risk of future type 2 diabetes 65 and increased risk of metabolic syndrome, respectively. 82 This could motivate patients to embrace lifestyle changes more aggressively. So how should this possible increased work load in the future be handled in the laboratory? It could be included as part of the serum LFT profile or carried out as an individual test. Including serum GGT estimation as part of the serum LFT profile would increase the cost and workload considerably, as these profiles are repeated frequently both in, inpatients and in outpatients. Unless evidence obtained in the future indicates that frequent monitoring is of clinical value, this elevated cost would come with no real benefit in terms of clinical care and outcomes.
Reference intervals for GGT
The more difficult question about reference intervals for serum GGT activity should be addressed as a matter of urgency. It is clear that the current reference intervals used in most laboratories are inappropriate as numerous studies have confirmed increased mortality in patients with serum GGT activities even within the current reference intervals. These reference intervals were derived originally in subjects who were apparently normal with no evidence of chronic disease. GGT should be treated like cholesterol, glucose and HbA1c where the upper limit of the serum reference interval is derived from the level above which the risk increases. It would appear from the several studies mentioned above that the upper serum activity limit above which the CV risk increases (taking a more conservative value) in women is around 9 U/L and in men around 14 to 20 U/L.10,12,13,23,24,35 While there is no current evidence that measuring serum GGT activity is useful to assess CV risk beyond conventional CV risk factors, it is nevertheless important to establish correct reference intervals that are likely to be lower as for example for serum ALT, 122 than are currently used in most UK laboratories. A raised serum GGT activity should alert physicians and prompt follow up to reinforce vigorous lifestyle changes to reduce CV risk. Using current reference intervals is likely to give a false sense of security to clinicians that all is well, and no further action is required, which may not be the situation in most cases.
A UKNEQAS study of reference intervals in 2013 showed that in addition to the expected difference in results obtained between method groups, differences were also obtained within the same method group (information supplied by UKNEQAS). The differences observed between results obtained by different methods in females appeared to be smaller, possibly because the absolute results in females were lower.
Establishing reference intervals for serum GGT would require care in selecting normal subjects because of the ramifications serum GGT activity has on the development of various chronic disease states including CV 123 and non-CV disorders. 124 Subjects should be screened for hepatobiliary disease including NAFLD, excess alcohol intake, unhealthy lifestyles, chronic CV and other diseases, long-term medication and with BMI <25 kg/m2, normal glucose tolerance test and/or normal fasting plasma glucose concentration, HbA1c, lipids, blood pressure and waist circumference. Regular follow-up for at least five years with repeat blood tests would be necessary to assess any change in clinical status including change in serum GGT activity to determine the clinical impact of longitudinal change in serum GGT. It would be essential to include individuals of Asian origin as there could be a difference between those of Caucasian and those of Asian descent. It would appear desirable that reference intervals are determined at a national or international level to minimize the problems associated with the identification and long term follow-up of patients at low and high risk of disease and who may have GGT measured in different laboratories.
The upper reference limit for serum GGT would be the 95th sex-specific percentile from the population at lowest risk of disease and mortality, as serum GGT activity shows a skewed distribution. The lower reference limit would be the 5th percentile as there is no evidence at present to suggest either a ‘U’ or ‘J’ shaped relationship between GGT and adverse events, unlike for ALT.37,125,126 Until then, like the situation for cholesterol, a policy should be pursued that recommends the lower the GGT result, the better it is for the patient, unless there is evidence in the future for a J- or U-shaped relationship. Lifestyle modifications are still the corner stone for primary prevention of CV morbidity and mortality.
Conclusions
The primary role of GGT is to metabolize extracellular reduced GSH, enabling precursor amino acids to be assimilated and re-utilized for synthesis of intracellular GSH, and is a marker of oxidative stress. Increased serum GGT activity is associated with increased CV and all-cause mortality, even if within the reference interval. Serum GGT activity is a marker for future type 2 diabetes including the longitudinal increase in GGT over time, and is associated with conventional CV risk factors and the metabolic syndrome. Histochemical and biochemical data suggest that GGT activity in atherosclerotic lesions may play a role in precipitation and progression of atherosclerotic disease.
The Szasz method produces lower results compared to the IFCC method, and laboratories should consider switching to the IFCC method to make results comparable across laboratories.
There is no evidence at present that measuring serum GGT improves CV risk prediction beyond conventional risk factors. Nevertheless, the issue of reference intervals for GGT needs to be addressed as soon as possible, as current intervals are inappropriate and can be misleading and underestimating CV risk. A raised serum GGT activity should be regarded as an alert sign to reinforce lifestyle changes vigorously to reduce CV risk.
Future developments
The reasons for mild elevation of serum GGT activity apart from cholestasis and liver disease need to be clarified. Important insights might be provided by the genetic analysis of GGT proteins expressed in patients, possibly identifying associations between GGT and specific polymorphisms.
Circulating GGT is a heterogeneous entity consisting of several molecular complexes. 127 Detailed analysis of lipoprotein complexes with GGT could improve the ability to screen patients at high risk in the future. Interventions to remove these circulating GGT complexes or to prevent their formation might eventually lead to therapeutic applications.
Other aspects that need to be determined are factors favouring accumulation of GGT in the intimal space, the extent to which GGT-dependent redox reactions can affect progression of atherosclerosis and ways to reduce inflammation secondary to oxidative stress. 89
Elucidation of these aspects promises an exciting future, and is likely to provide the basis for advances in diagnosis, risk stratification and treatment of atherosclerosis-related CV diseases including diabetes in the future.
Footnotes
Acknowledgements
The authors would like to thank Rhona Inocco for help with the figures and Finlay Mckenzie from NEQAS for information about methods and performance of GGT assays.
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SB.
Contributorship
SB wrote the manuscript and MS collected information about GGT methods and performance. Both authors reviewed and approved the manuscript.