
Abstract
Background
Vascular endothelial growth factor A stimulates angiogenesis, but is also pro-inflammatory and plays an important role in the development of neurological disease. This study aimed to investigate whether vascular endothelial growth factor A mRNA expression could be used as a marker for the prediction of susceptibility to multiple sclerosis and relate vascular endothelial growth factor to the clinical phases of multiple sclerosis.
Methods
This was a cross-sectional study, consisting of a total of 60 subjects with multiple sclerosis and 20 healthy controls. Subjects were subjected to history taking, neurological examination and peripheral blood sampling for vascular endothelial growth factor A mRNA gene expression. Vascular endothelial growth factor A gene expression was measured by real-time polymerase chain reaction using the SYBR Green technique.
Results
Vascular endothelial growth factor A mRNA gene expression level was significantly lower in the multiple sclerosis group than in the healthy control group (P < 0.001). Vascular endothelial growth factor A mRNA gene expression level was higher in relapsing remitting multiple sclerosis (RRMS) patients than in those in remission (P < 0.001) and in relapsing remitting multiple sclerosis compared with secondary progressive multiple sclerosis (P < 0.001). There was no correlation between vascular endothelial growth factor A gene expression levels and duration of disease, multiple sclerosis progression index or expanded disability status scale.
Conclusions
A lower vascular endothelial growth factor A mRNA gene expression level was independently associated with a higher risk of multiple sclerosis.
Introduction
Multiple sclerosis (MS) is an autoimmune disease of the central nervous system (CNS) that in most cases is characterized by a relapsing-remitting (RR) disease course. With time, the disease progresses, with failure of repair mechanisms leading to gradual neurodegeneration and a continuous increase in disability. 1 Very little is known about the mechanisms underlying the transition to progressive MS disease, and the diagnosis of a progressive disease course is made solely on clinical grounds, since reliable supporting laboratory or neuro-radiological tests are lacking. This can cause problems clinically, when making treatment decisions. 2 The exact aetiology of MS is unknown, but it is thought to depend on a complex interaction between genetic and environmental factors. Vascular endothelial growth factor (VEGF) is an angiogenic and pro-inflammatory factor with neuroprotective effects on neuronal and glial cells.
Results from some studies have indicated a role for vascular endothelial growth factor-A (VEGF-A) in MS.3–7 Increased expression of VEGF-A has been detected in CNS tissue and serum in animal models and in patients with MS. 6 In addition, endothelial cell proliferation and increased blood vessel density have been documented in acute MS lesions, 8 and experimental autoimmune encephalomyelitis (EAE). 9 EAE is an animal model for MS. It can be induced by immunization using antigens derived from myelin. These antigens elicit an acute demyelinating process driven by T cells and macrophages which can have a chronic relapsing course quite similar to MS. 10 In EAE, VEGF-A is expressed by monocytes and activated T cells and is associated with a Th1 T-cell phenotype and increased severity of inflammation. 11
Some histopathological features of the MS lesions resemble hypoxic damage, perhaps because of metabolic disturbances. They also display an increased expression of hypoxia inducible factor 1 a (HIF1a), a transcription factor for VEGF-A. 12
The study by Holley et al. 13 demonstrated an increase in blood vessel density in MS lesions compared with normal healthy controls (HCs) and increased proliferation of endothelial cells within these blood vessels. These findings suggest that angiogenesis occurs in MS.
The aim of the present study was to determine VEGF-A mRNA expression profiles in the whole blood of subjects with MS and relate them to different disease subtypes. We also investigated a possible role of VEGF-A during transition from relapsing remitting multiple sclerosis (RRMS) to secondary progressive MS (SPMS). In addition, we sought to ascertain if there was any correlation between VEGF mRNA gene expression and brain magnetic resonance imaging (MRI) findings, age, multiple sclerosis severity score (MSSS), expanded disability status scale (EDSS) and disease duration.
Materials and methods
Subjects
A total of 60 MS patients (16 male and 44 female) at the Department of Neurology, Cairo University Teaching Hospital, Egypt were enrolled in this cross-sectional study in 2013. The HC subjects were blood donors (10 males and 10 females).
The subjects with MS consisted of: 20 with SPMS, 22 with RRMS and 18 with primary progressive MS (PPMS). Of the 22 subjects with RRMS, 8/22 (36.4%) were in relapse, defined according to Schumacker et al. 14 and 14/22 (63.6%) were in remission. For RRMS, a relapse was defined as an increase with ≥1 point on the EDSS, with a duration of at least one week prior to sampling, where systemic infection had been ruled out. Remission was defined as a stable clinical status for three months prior to sampling. SPMS was defined as an initial RR disease course, followed by more than 12 months of continuous worsening of neurological function (≥ 0.5 EDSS point) not explained by relapse. 2 All subjects with MS were receiving treatment according to the clinical judgement of the assessing neurologist. Disease-modifying treatments included solumedrol (methylpredinsilone) (Pfizer Company, Belgium) – 36/60 subjects (60%), Endoxan (cyclophosphamide) (EIMC Company, Korea) – 10/60 subjects (16.7%) and solumedrol and Endoxan – 14/60 subjects (23.3%).
Inclusion criteria of MS subjects comprised the following: (1) definite MS according to the International Panel on Diagnosis of MS, McDonald's criteria 2010, 15 (2) all types of MS, (3) gender: both male and female subjects were recruited. Patients with clinical evidence of autoimmune disease, arthritis, or infections prior to or complicating the attack, or with clinical evidence of myocardial infarction were excluded from the study.
Subjects with MS underwent history taking, general and full neurological examination and MRI. Brain and cervical MRI was performed on a 1.5 Tesla Phillips Intera scanner. Diagnostic criteria incorporated MRI and evoked potential testing (visual, auditory and somatosensory). Parallel information was recorded on disease duration, type of MS, relapse status, disability measured by the EDSS 16 and medications. The MSSS was calculated from EDSS and disease duration. 17
The IgG-specific oligoclonal banding in serum, CSF and IgG CSF index were routinely analysed in the Chemical Pathology Department.
The study was approved by the local ethics committee of our Institute. Informed consent was obtained from all study subjects after the nature of the study was explained.
Specimen collection
Two millilitres of EDTA blood were collected for the determination of VEGF-A mRNA gene expression (RNA extraction followed by complementary (c) DNA generation and stored at −20℃).
Methods
Real-time polymerase chain reaction
mRNA levels of VEGF were assessed by a quantitative real-time polymerase chain reaction (RT-PCR) assay using glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as a housekeeping gene. Total RNA was extracted from 1 mL of fresh blood collected into EDTA tubes from patients and HC using an RNeasy mini kit (Qiagen, Germany). cDNA was synthesized by reverse transcription (RT) with the Thermoscript™ RT kit (Invitrogen, Berlin, Germany), using random hexamers as amplification primers. In detail, 2.5 μg of total RNA, 50 ng of random hexamers and 1 mM dNTPs were heated at 65℃ for 5 min. The final mix (20 μL) was incubated for 10 min at 25℃ for primer extension, and cDNA synthesis was conducted at 55℃ for 50 min. The reaction was terminated by heating at 85℃ for 5 min.
The primer sequences for GAPDH and primer sequences for VEGF were designed with online software Primer3 (http://www-genome.wi.mit.edu/cgi-bin/ primer/primer3www.cgi) and were purchased from Qiagen (Australia). VEGF was determined using SYBR Green chemistry. Diluted (1/20) cDNA (4 μL) was added to a PCR mix containing 2.4 μL sterile water, 10 μL 2 × SYBR mix (Qiagen, Clifton Hill, Victoria, Australia) and 1.5 μL each of forward and reverse primers to make up a final volume of 20 μL. Cycling conditions for amplification were 95℃ for 10 min, followed by 40 cycles of 95℃ for 15 s, 60℃ for 30 s and a final step of 95℃ for 15 s, 60℃ for 15 s and 95℃ for 15 s in a StepOne™ thermal cycler (Applied Biosystems). The calculations of relative gene expression were done using the ΔΔCT method. Because the amount of product doubles in each cycle, the relative gene expression was calculated using the formula 2 -ΔΔCT. 18
Statistical analysis
Statistical analyses were performed using SPSS (Statistical Package for Social Sciences), version 17. 19 Data were subjected to the Kolmogorov-Smirnov test to determine the distribution and method of analysis. Normally distributed quantitative variables were presented as the mean (SD), and therefore the comparisons age between groups were performed using the Student’s t-test. The following data, i.e. disease duration, EDSS, MSSS and VEGF-A mRNA gene expression level showed skewed distributions and were expressed as medians (ranges). VEGF-A mRNA gene expression levels between groups were compared using the Mann-Whitney test. Stratified analysis based on forms of MS was performed by the Kruskal-Wallis H test. Categorical variables are cited as percentages. A chi-square test was used to compare gender. The effect of demographic and clinical variables (age, disease duration, MSSS and EDSS) on VEGF-A mRNA gene expression was determined individually with the Spearman Rank correlation coefficient (r). A P value (two-tailed) <0.05 was considered statistically significant.
Results
Demographic characteristics, laboratory and MRI findings and clinical features, of subjects with MS compared with healthy controls.
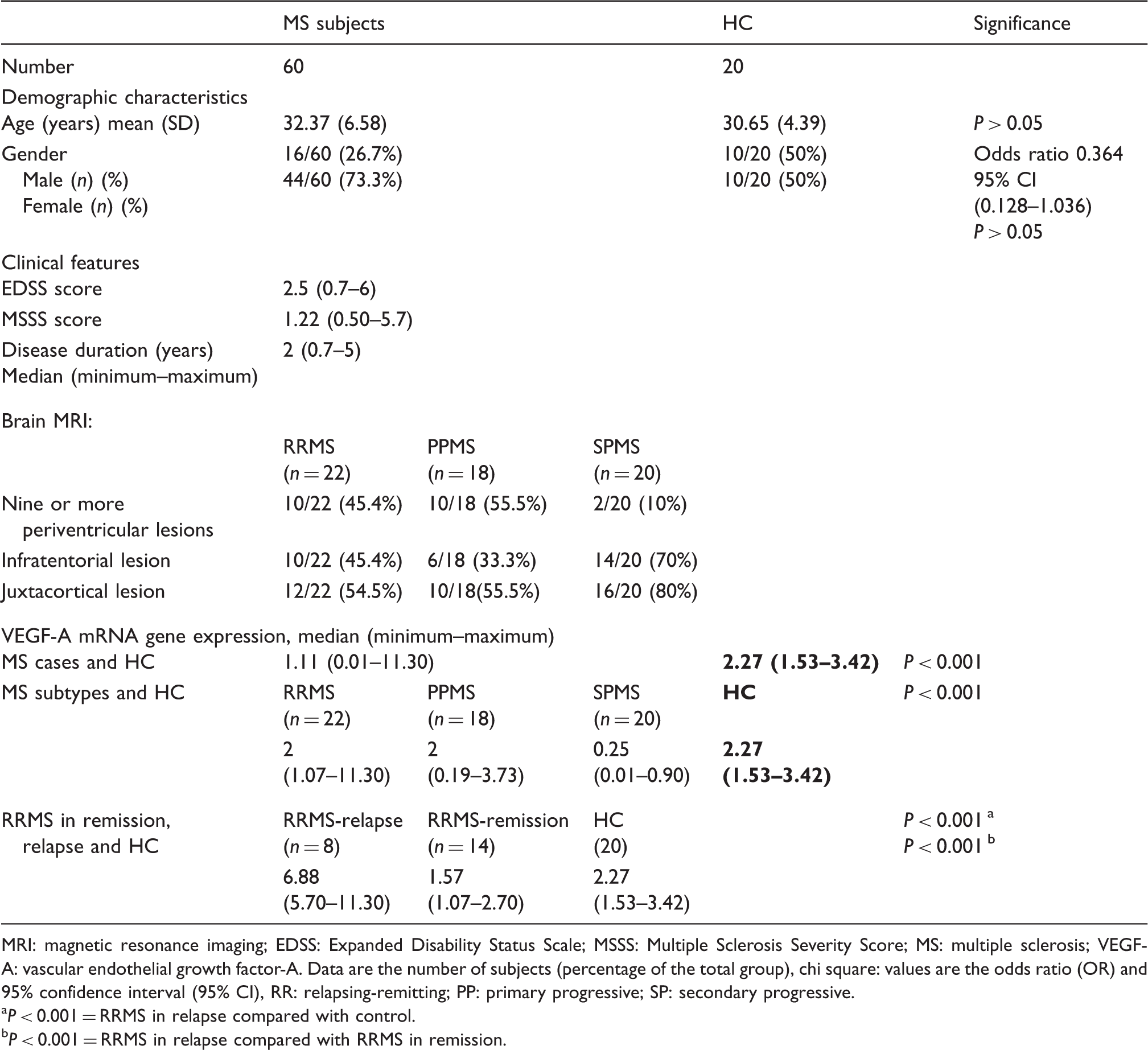
MRI: magnetic resonance imaging; EDSS: Expanded Disability Status Scale; MSSS: Multiple Sclerosis Severity Score; MS: multiple sclerosis; VEGF-A: vascular endothelial growth factor-A. Data are the number of subjects (percentage of the total group), chi square: values are the odds ratio (OR) and 95% confidence interval (95% CI), RR: relapsing-remitting; PP: primary progressive; SP: secondary progressive.
P < 0.001 = RRMS in relapse compared with control.
P < 0.001 = RRMS in relapse compared with RRMS in remission.
The gender and mean (SD) age did not differ significantly between patients with MS and HC (P > 0.05). There was a statistically significant difference in median mRNA VEGF expression level between the HC 2.27 (range: 1.53–3.43) compared to subjects with MS 1.11 (range: 0.01–11.30) (P < 0.001). There was a statistically significant difference in median mRNA VEGF expression between HC and subjects in each of the MS clinical types, RRMS, SPMS and PPMS (P < 0.001). Similarly, median mRNA VEGF expression in subjects with RRMS in relapse was significantly different to the median expression observed in subjects with RRMS in remission and to that observed in HC (P < 0.001), with the highest value found among those subjects with RRMS in relapse.
Correlation between VEGF-A mRNA gene expression level among subjects with MS and age, disease duration, EDSS and MSSS.
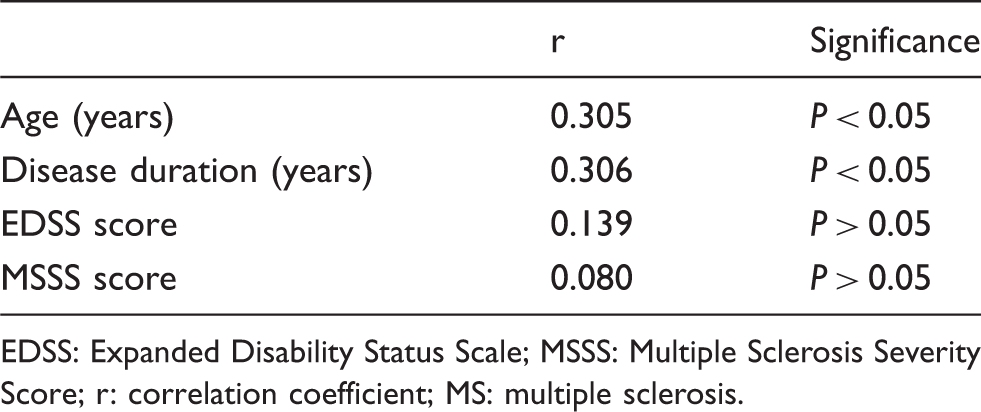
EDSS: Expanded Disability Status Scale; MSSS: Multiple Sclerosis Severity Score; r: correlation coefficient; MS: multiple sclerosis.
Discussion
The exact role of VEGF-A in cerebral injury and inflammation is still unclear. There is substantial evidence that VEGF-A is a pro-inflammatory factor and can cause CNS damage. Inhibition of endogenous VEGF-A can lead to decreased brain lesion size, whereas administration of VEGF-A can exacerbate CNS damage and up-regulate immunomodulatory adhesion molecules and cytokines. 20
The aim of this study was to quantify the expression of VEGF-A mRNA from patients with MS in Egypt. The median value of VEGF mRNA expression in the HC was significantly different to the median value observed in subjects with MS, and also to the median value in those subjects stratified by MS clinical type, RRMS, SPMS and PPMS. There was also a statistically significant difference in median mRNA VEGF expression between subjects with RRMS in relapse compared with those in remission and also with HC, with the highest level of expression found among those subjects with RRMS in relapse. The number of brain MRI lesions did not influence median mRNA VEGF expression. mRNA VEGF expression showed a positive correlation with age and also with disease duration. There was no correlation between mRNA VEGF expression and other measures of disease severity: EDSS and MSSS. VEGF mRNA gene expression can distinguish RRMS from SPMS.
The results of the present study showed a down-regulation of mRNA VEGF gene expression in whole blood of subjects with MS compared with HC.
Results from studies performed on VEGF gene expression, protein level and CSF level have been controversial. Iacobaeus et al. 2 demonstrated that the expression of VEGF-A is down-regulated in CSF cells irrespective of disease course, but that only patients with SPMS display a down-regulation of VEGF-A expression in peripheral blood mononuclear cells (PBMCs) as compared to both subjects with RRMS and to HC. These authors also measured VEGF-A protein levels, using an ELISA technique, in a small subset of patients and demonstrated a non-significant trend towards decreased levels in those patients with SPMS compared to both those with RRMS and also to HC. 2 Seabrook et al. 21 also, using ELISA, found a decreased level of VEGF in subjects with MS. The expression of VEGF during EAE is controversial, with both increased as reported by Roscoe et al. 22 and Proescholdt et al. 4 and decreased expression as reported by Tham et al. 3
Data from the study by Proeschold et al. 4 have shown that chronic administration of VEGF to normal brain causes blood–brain barrier (BBB) breakdown of small and large molecules in vivo. Impairment of BBB integrity is an early and consistent diagnostic finding in MS, and could be an important aspect of the pathogenesis of the disease. Chronic over-expression of VEGF in reactive/gliotic astrocytes could contribute to the permanent BBB breakdown within an MS plaque. 23 In addition to the induction of increased microvascular permeability, the studies by Ferrara, 24 Melder et al. 25 and Proescholdt et al. 26 reported the up-regulation of adhesion molecules on capillary endothelial cells by VEGF in vivo. The expression of adhesion molecules plays an important role in the process of lymphocyte trafficking and homing during CNS inflammation.
The present study found that there was a significant difference in VEGF mRNA expression in whole blood among MS subtypes compared with HC. Meanwhile, a study by Iacobaeus et al., 2 performed using PBMC, stated that patients with SPMS are characterized by a prominent decrease of VEGF-A mRNA expression in PBMC compared with both subjects with RRMS and with HC, who display comparable levels of VEGF-A expression. These authors suggested that down-regulation of VEGF-A mRNA expression in PBMC reflects an underlying disease mechanism that operates specifically in patients with progressive MS, which was of interest in the context of emerging evidence that connects dysregulation of VEGF-A with neurodegenerative processes. 2
In this study, we observed a significant difference in VEGF mRNA expression level in the whole blood of patients with RRMS and who were in remission, compared with those with RRMS and who were in relapse.
The study by Iacobaeus et al. 2 using PBMC, found no significant difference in expression, between patients with RRMS, whether in relapse or in remission. In addition, there was a trend towards higher levels of VEGF-A expression in PBMC from RRMS sampled during a relapse as compared with patients in remission. The study by Su et al. 6 suggested that an increase in serum VEGF concentration might be involved in MS relapse.
These authors 6 found that serum VEGF concentrations were significantly elevated in patients with MS in relapse compared with both HC and those in remission, irrespective of clinical subtype. An increase of VEGF-A concentration in the initial phases of relapse is compatible with its role as a pro-inflammatory factor that attracts monocytes and lymphocytes, up-regulates immunomodulatory adhesion molecules, stimulates secretion of pro-inflammatory cytokines and increases BBB permeability.3,20 Stockhammer et al. 27 measured serum VEGF in 19 patients with MS and with unspecified clinical phases and found no elevation of VEGF. Proescholdt et al. 4 reported the up-regulation of VEGF in MS lesions as well as in acute lesions in rats with EAE, an animal model of MS. Croll et al. 20 demonstrated decreased levels of VEGF-A protein in rat spinal cord tissue during EAE relapse and a reduced expression in neurons following immunohistochemistry. Iocobaeus et al. 2 found no significant difference between relapse and remission in CSF. Seabrook et al. 21 demonstrated that neuronal expression of VEGF was present during acute EAE, whereas during the relapse phase, neuronal VEGF decreased.
Manoonkitiwongsa et al. 28 stated that the discrepancy in their results could be related to the timing of sampling in relation to the onset of relapse symptoms or the occurrence of subclinical disease activity in the remission group. It is known that the net effect of VEGF-A can vary depending on the target tissue, the timing and the concentration.
VEGF has been shown to be associated with age-associated diseases, such as neovascular age-related macular degeneration.29,30 In the present study, there was a correlation between VEGF and age and disease duration, in agreement with the findings reported by Mould et al. 31 However, there was no correlation between VEGF mRNA expression and EDSS and MSSI, a finding consistent with those of others.2,6 The lack of correlation between VEGF and EDSS scores could be explained by the fact that the latter are determined by dysfunction in various parts of the CNS.
Although angiogenesis is probably not the first event in the pathogenesis of MS, its changing role in the different phases of disease progression makes it an important and underestimated target in therapeutic options. The current concept of the natural history of MS refers to a combination of two phenomena underlying the two phases of MS, namely an inflammatory process in the remitting phase and a neurodegenerative process in the progressive phase. The secondary progressive phase of MS is primarily caused by axonal degeneration following demyelination. The potential advantages of inhibiting angiogenesis in the early phase of MS could stem from reducing the vascular supply of nutrients and inflammatory cells to the demyelinating lesions, halting the production of endothelial-derived pro-inflammatory molecules. This approach should be proposed only in aggressive acute relapsing MS, where immunosuppression could be associated with specific antiangiogenic therapy. Considering the central role of VEGF signalling in pathological angiogenesis during the early MS phase, anti-VEGF therapy should be highly beneficial in the aggressive MS-subtype. 10
In conclusion, we have demonstrated that expression of VEGF-A is down-regulated in subjects with MS compared with HC. Thus, VEGF-A mRNA expression may reflect an underlying disease mechanism that operates specifically in progressive MS. In contrast, there was a significant increase in expression in those subjects with RRMS and who were in relapse, compared with expression in HC and in those patients with RRMS who were in remission. mRNA VEGF gene expression level did not correlate with any of the parameters of disease severity.
Since genotypes encoding higher VEGF production are reportedly associated with diabetic microvasculopathy 32 and acute renal allograft rejection, 33 and since significant ethnic differences in polymorphisms of the VEGF gene have also been reported, 34 we believe such polymorphisms warrant future investigation in patients with MS, especially those of African origin. Further studies in larger clinical settings are needed to address the question of whether dysregulated VEGF-A expression in MS is a cause or a consequence of a progressive disease phenotype.
Footnotes
Declarations conflict of interest
None.
Funding
None.
Ethical approval
This study was approved by the local ethics committee of Faculty of Medicine, Fayoum University and Faculty of Medicine, Cairo University, with informed consent.
Guarantor
HA.
Contributorship
HA, HE and MA carried out the molecular genetic studies. HA was involved in protocol development, gaining ethical approval and data analysis. She wrote the first and final draft of the manuscript. HH and SE were involved in patient recruitment. All authors reviewed and edited the manuscript and approved the final version of the manuscript.