
Abstract
Background
Tamm–Horsfall protein (also known as uromodulin) is the most abundant urinary protein in healthy individuals. Since initially characterized by Tamm and Horsfall, the amount of urinary excretion and structural mutations of Tamm–Horsfall protein is associated with kidney diseases. However, currently available assays for Tamm–Horsfall protein, which are mainly enzyme-linked immunosorbent assay-based, suffer from poor reproducibility and might give false negative results.
Methods
We developed a novel, quantitative assay for Tamm–Horsfall protein using reversed-phase high-performance liquid chromatography. A precipitation pretreatment avoided urine matrix interference and excessive sample dilution. High-performance liquid chromatography optimization based on polarity allowed excellent separation of Tamm–Horsfall protein from other major urine components.
Results
Our method exhibited high precision (based on the relative standard deviations of intraday [≤2.77%] and interday [≤5.35%] repetitions). The Tamm–Horsfall protein recovery rate was 100.0–104.2%. The mean Tamm–Horsfall protein concentration in 25 healthy individuals was 31.6 ± 18.8 mg/g creatinine. There was a strong correlation between data obtained by high-performance liquid chromatography and enzyme-linked immunosorbent assay (r = 0.906), but enzyme-linked immunosorbent assay values tended to be lower than high-performance liquid chromatography values at low Tamm–Horsfall protein concentrations.
Conclusions
The high sensitivity and reproducibility of our Tamm–Horsfall protein assay will reduce the number of false negative results of the sample compared with enzyme-linked immunosorbent assay. Moreover, our method is superior to other high-performance liquid chromatography methods, and a simple protocol will facilitate further research on the physiological role of Tamm–Horsfall protein.
Keywords
Introduction
Tamm–Horsfall protein (THP), also known as uromodulin, was first reported as a mucoprotein by Morner 1 and was characterized by Tamm and Horsfall 2 . The glycoprotein is synthesized by epithelial cells of the thick ascending limb of Henle's loop. THP is the most abundant protein in the urine of healthy individuals. Urinary excretion of THP is affected by salt intake 3 and urine volume, but it is excreted at an average rate of 50–100 mg/day.4–6
THP prevents urinary tract infection via its large carbohydrate moiety, which accounts for approximately 30% of its molecular weight.7,8 This carbohydrate moiety inhibits viral haemagglutination, 2 binds to uropathogenic bacteria and hinders the adherence of bacteria and viruses to glycoproteins and glycolipids in luminal cell membranes.9–11 In addition, a mutation in the uromodulin gene was recently implicated in the clinical manifestations of medullary cystic kidney disease type 2 and familial juvenile hyperuricemic nephropathy. 12 The mutation disrupts the tertiary structure of THP. Bleyer et al. 13 reported that this mutation also decreases urinary excretion. Therefore, the development of a sensitive method to quantify THP in the urine is essential for the diagnosis and classification of renal disease.
Currently, THP is measured using in-house or commercial enzyme-linked immunosorbent assay (ELISA)-based methods. However, it is difficult to quantify urinary THP because of its inherent gelation and instability. In solution, THP tends to form a gel; this process is accelerated by various factors found in the urine, such as sodium and calcium ions, 14 albumin 15 and Bence Jones proteins, 16 whereupon THP aggregates in the urine (Mr: 7 × 107 Da) and is implicated in the formation of urinary casts. 17 There are significant differences in the urinary THP concentrations measured using ELISA between studies in the range of 2.1–19.3 μg/mL for males and 12.9–45.4 μg/mL for females, 18 to 4 ± 1.8 μg/mL, 19 to 55–77.9 μg/mL for males and 70.7–96 μg/mL for females. 20 These data suggest that the gelation and instability of THP interfere with ELISA. Most ELISA-based methods require 10–1000-fold urine sample dilution to avoid THP gelation, leading to poor sensitivity and reproducibility associated with low concentrations.
The natural fluorescence of THP means that it can be measured with high sensitivity by high-performance liquid chromatography (HPLC). 21 Our protocol uses a pretreatment to avoid gelation-related interference and HPLC optimization based on polarity differences between THP and other major urine components.
The advantage of HPLC is that it can analyse THP both quantitatively and qualitatively. Moreover, HPLC is cost-effective, because it does not require special reagents, such as antisera, as compared with ELISA. We developed a novel HPLC protocol for the measurement of THP in urine samples that offers sensitive and reliable measurements even in the low-concentration range.
Materials and methods
Clinical samples and THP standard
Urine samples were collected from the Department of Clinical Laboratory at Kyushu University Hospital, Fukuoka, Japan. HPLC-grade acetonitrile was purchased from Kanto Chemical Co., Inc. (Tokyo, Japan). Water was purified using a Milli-Q system (EMD Millipore Corporation, Billerica, MA, USA). For spiking purified human serum albumin, gamma-globulin (γ-GLB), haemoglobin and transferrin were purchased from Sigma-Aldrich Co. LLC (Tokyo, Japan); α1-microglobulin and β2-microglobulin were purchased from Funakoshi Co., Ltd (Tokyo, Japan). All other chemicals were of analytic grade.
A standard THP solution was prepared from healthy human pooled urine using the diatomaceous earth filtration method 22 with slight modifications. 23 Isolated THP was lyophilized after dialysation against distilled water.
Sample preparation
Pretreatment procedure
THP was isolated from urine by sodium chloride precipitation as reported by Tamm and Horsfall. 2 The volume of each sample was adjusted to 1 mL by the addition of 0.58 mol/L sodium chloride (e.g. 800 μL of urine + 200 μL sodium chloride). This mixture was centrifuged at 20,000 g for 10 min. The supernatant (950 μL) was discarded and replaced with 750 μL of distilled water to yield a final volume of 800 μL. The samples were vortexed to dissolve the precipitates completely, and 10 μL aliquots were added to HPLC columns.
Sample storage
Stability of the THP in urine may affect its clinical applicability. However, Youhanna et al. 24 reported that urinary THP is stable at −80 ℃ for three months. Therefore, all urine samples were stored at −80 ℃ and analysed within one month.
Sodium dodecyl sulphate polyacrylamide gel electrophoresis
Urine contains several proteins, so proteins other than THP may also be precipitated by the pretreatment. Therefore, we evaluated the purity of the precipitates using sodium dodecyl sulphate polyacrylamide gel electrophoresis (SDS-PAGE). Major urinary proteins (THP, albumin, γ-GLB, α1-microglobulin, β2-microglobulin, haemoglobin and transferrin) were added to the pooled urine, and pretreatment was performed. SDS-PAGE of the pretreated urine sample and several standard protein solutions was performed on a 12.5% homogeneous polyacrylamide gel (ATTO Corporation, Tokyo, Japan) according to Laemmli's method. 25 We incubated 20 μL of each sample at 100 ℃ for 5 min after the addition of 20 μL of sample buffer (0.125 mol/L Tris-HCl at pH 6.8, 4% SDS, 20% glycerol, 0.01% bromophenol blue and 10% β-mercaptoethanol). We applied 7 μL of the mixture to the gel, and SDS-PAGE was performed at 30 mA of constant current. Silver staining was performed using a silver staining kit obtained from Wako Pure Chemical Industries, Ltd (Osaka, Japan), according to the manufacturer's protocol.
Influence of salts in urine on HPLC assay system
We prepared pooled urine, which added several salts and nothing else. The HPLC pretreatment was performed against them and then compared the concentration of THP by HPLC. If the residual salts affect assay system, the measurement values between addition and non-addition should be different. The kinds of added salts are sodium chloride, potassium chloride, magnesium chloride hexahydrate, calcium chloride dihydrate, sodium hydrogen carbonate, sodium dihydrogen phosphate dihydrate, urea, disodium hydrogen phosphate 12-water, ammonium sulphate and trisodium citrate. The added concentrations are 0.1 and 0.25 mol/L.
Assessment of the loss of THP following pretreatment
It is expected that all of urinary THP is not precipitated by pretreatment. Hence, we evaluated how much of THP can collect by pretreatment procedure. Three different concentrations of THP standard solution (20, 40 and 60 μg/mL) were added to pretreated pooled urine samples. Three patterns of treatment were prepared: ‘None, Sodium chloride, Pretreatment’. ‘None’ means no treatment. It contains pretreated pooled urine and THP standard. ‘Sodium chloride’ means that sodium chloride was added intentionally in order to assess the effect of residual sodium chloride after pretreatment on the HPLC assay system. Therefore, it contains pretreated pooled urine, THP standard and sodium chloride, which is assumed to remain in the solution after pretreatment. ‘Pretreated’ means that the pretreatment was used. It contains pretreated pooled urine and THP standard. To measure each sample, we assessed the loss of THP caused by pretreatment procedure and evaluated the influence of residual sodium chloride on the HPLC assay system.
HPLC conditions
THP concentrations were measured using an HPLC system (Hitachi High-Technologies Corporation, Tokyo, Japan), comprising a pump equipped with a degasser (L-2130), an autosampler (L-2200), a column oven (L-2300) and a fluorescence detector (L-2480). Fluorescence detection was performed at an emission wavelength of 325 nm and an excitation wavelength of 280 nm. The urine components were separated on a COSMOSIL 5C18-MS-II Column (4.6 I.D. × 250 mm; Nacalai Tesque, Inc., Kyoto, Japan) using Eluent A (water + 0.12% formic acid) and Eluent B (acetonitrile + 0.12% formic acid). The column oven was maintained at 25 ℃, and the flow rate was 1 mL/min.
Validation of the HPLC method
Calibration standards for urinary THP were prepared at different concentrations (0, 4.5, 9.0, 18, 27, 36, 45, 54, 63, 72, 81 and 90 μg/mL) using lyophilized THP. Calibration curves were constructed by plotting the peak area of the diluted standards on HPLC against THP concentration. Intraday precision was determined by analysing the same urine samples 10 times on the same day. To the pooled urine samples, we added three different concentrations of standard THP solution (20, 40 and 60 μg/mL). Interday precision was determined by analysing aliquots of three urine samples (stored at −80 ℃) once a day for six consecutive days. The recovery rate was assessed by the addition of different concentrations (20, 40 and 60 μg/mL) of standard THP solution to the pooled urine.
Comparison of the HPLC and ELISA measurements
A correlation study was conducted with 28 clinical samples comparing the performance of HPLC with that of the Human Uromodulin ELISA Kit (BioVendor Laboratorní medicína a.s., Brno, Czech Republic), which was used according to the manufacturer's instructions. A Model 1575 ImmunoWash (Bio-Rad Laboratories, Inc., Hercules, CA, USA) was used to wash the microplates, and absorbance was measured with a Model 680 Microplate reader (Bio-Rad Laboratories, Inc.). Lyophilized THP was dissolved in distilled water, and 40 and 60 μg/mL quality control (QC) samples were prepared. The QC samples were analysed by HPLC and ELISA.
Measurement of urinary creatinine
Urinary creatinine was measured using an Automatic Biochemical Analyzer 7600−010S (Hitachi High-Technologies Corporation) with a commercially available reagent (Shino-Test Corp, Tokyo, Japan).
Results
Optimization of urinary THP separation
Purity of the precipitate after HPLC pretreatment
We evaluated the purity of the precipitate after pretreatment. Figure 1 shows the SDS-PAGE of pooled urine spiked with major urinary proteins (Lane 2), the precipitate of pooled urine spiked with major urinary proteins after pretreatment (Lane 3), the supernatant of pooled urine spiked with major urinary proteins after pretreatment (Lane 4) and the standard solution of THP (Lane 5). Since a single band was observed (Lane 5), the weight of lyophilized THP was measured and diluted with distilled water when used. Lanes 6–11 show major urinary proteins. In addition to THP, albumin, γ-GLB and transferrin were also present in the precipitate, indicating that those proteins co-precipitate with THP. However, the other proteins were not detected in the precipitate or supernatant.
Bands of major urinary protein by SDS-PAGE (silver staining). Lane 1,12: molecular markers; Lane 2: pooled urine spiked with major urinary proteins; Lane 3: the precipitate of pooled urine spiked with major urinary proteins after pretreatment; Lane 4: the supernatant of pooled urine spiked with major urinary proteins after pretreatment; Lane 5: standard solution of THP; Lane 6: albumin; Lane 7: γ-GLB; Lane 8: α1-microglobulin; Lane 9: β2-microglobulin; Lane 10: haemoglobin and Lane 11: transferrin.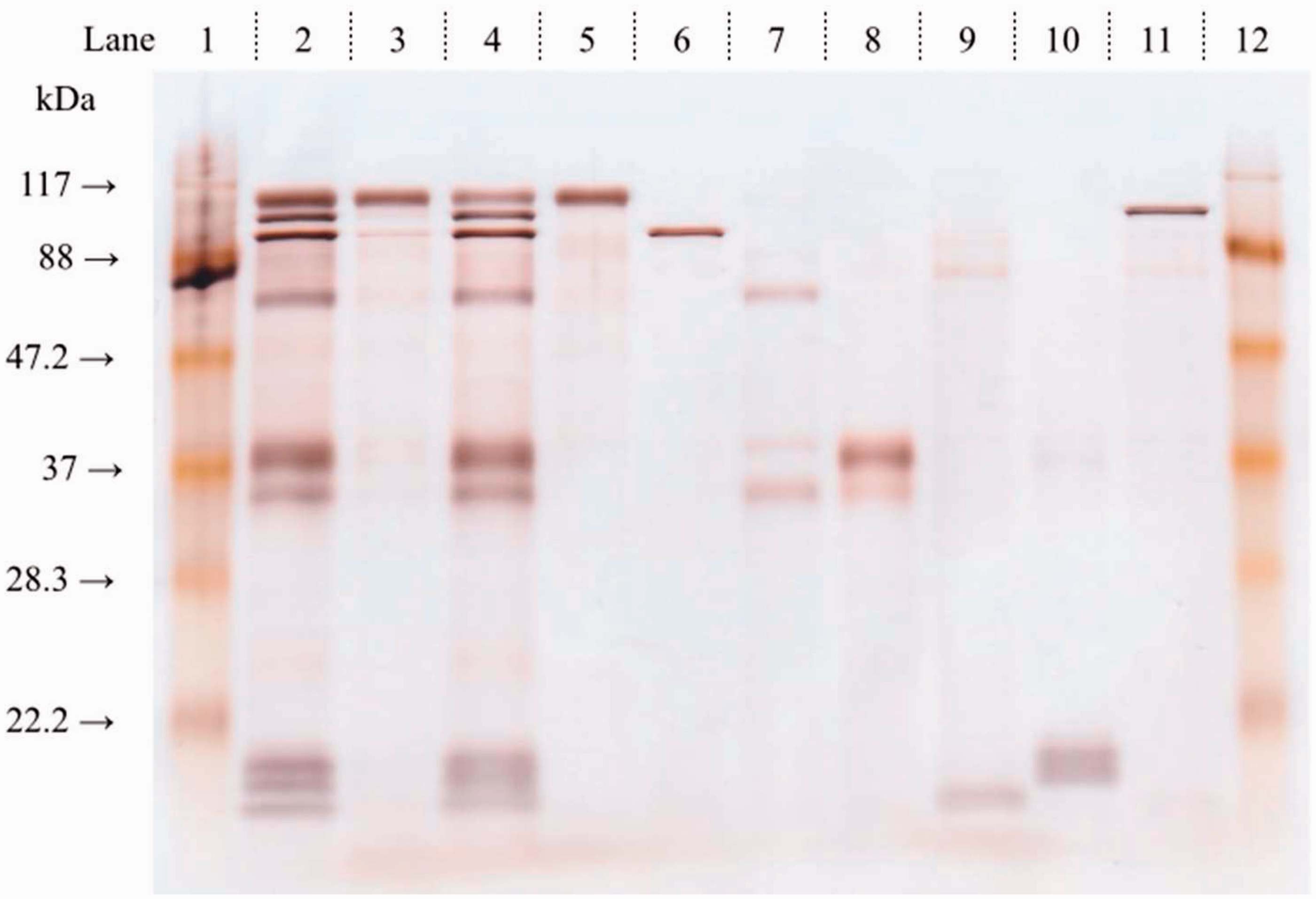
Establishment of optimum HPLC conditions for the separation of urinary THP
HPLC peak area and chromatographic parameters at different column temperatures.
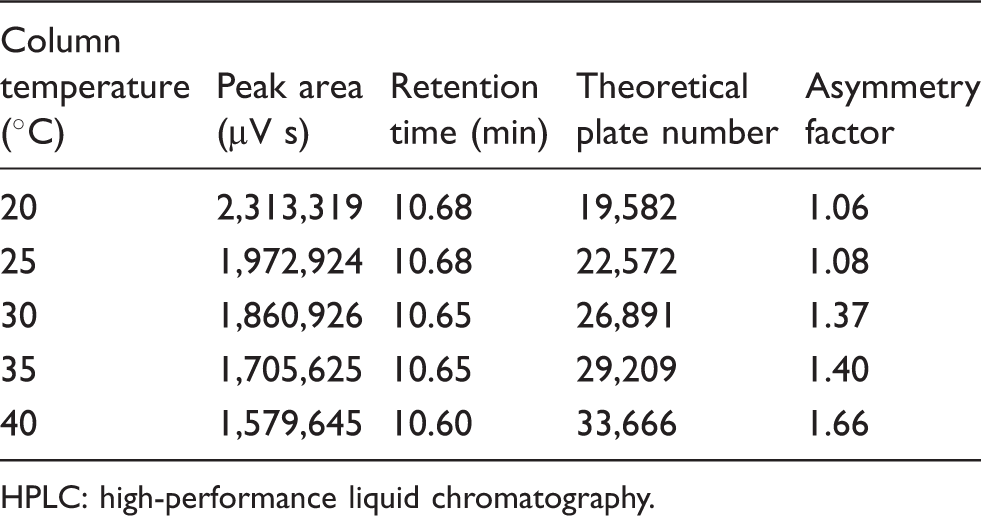
HPLC: high-performance liquid chromatography.
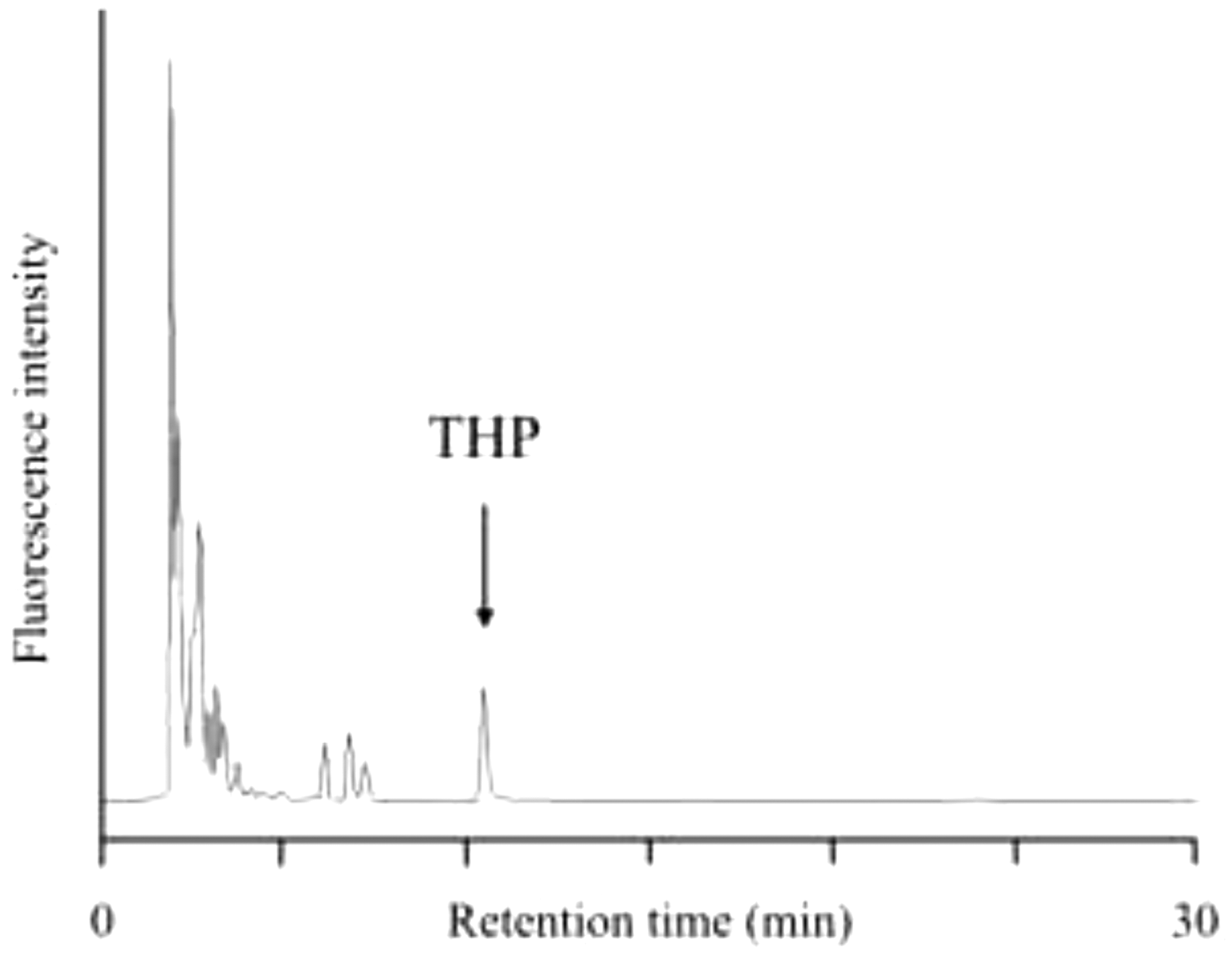
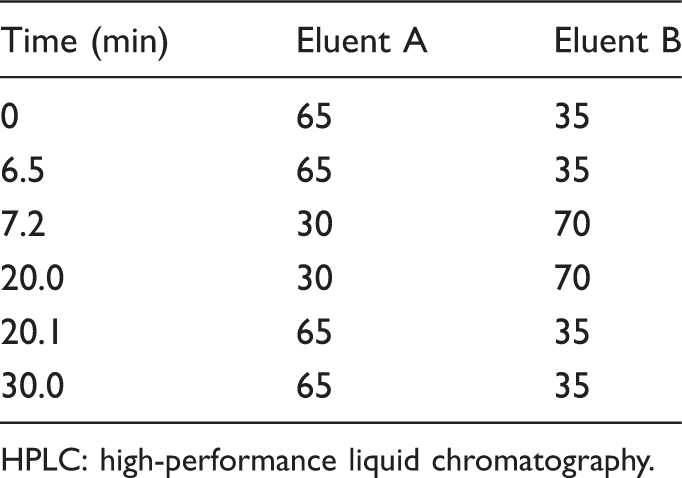
To keep the mobile phase acidic, 0.12% of formic acid was added to the eluent. Therefore, the optimum conditions were determined as follows: Eluent A comprised a water:formic acid ratio of 100:0.12 (v/v); Eluent B comprised an acetonitrile:formic acid ratio of 100:012 (v/v); stepwise elution was used (Table 2); and column temperature was maintained at 25 ℃. This approach yielded excellent separation of THP from albumin, γ-GLB and transferrin (Figure 2). Figure 3 demonstrates the efficient separation of THP from pretreated pooled urine samples by HPLC.
Peaks indicated with the arrow in the chromatogram show (a) Tamm−Horsfall protein, (b) albumin, (c) gamma-globulin and (d) transferrin. Details on the HPLC conditions are described in the text. Chromatogram of pooled urine samples showing the elution peak of Tamm–Horsfall protein. THP: Tamm–Horsfall protein. Optimal stepwise HPLC elution protocol for Tamm–Horsfall protein in urine samples. HPLC: high-performance liquid chromatography.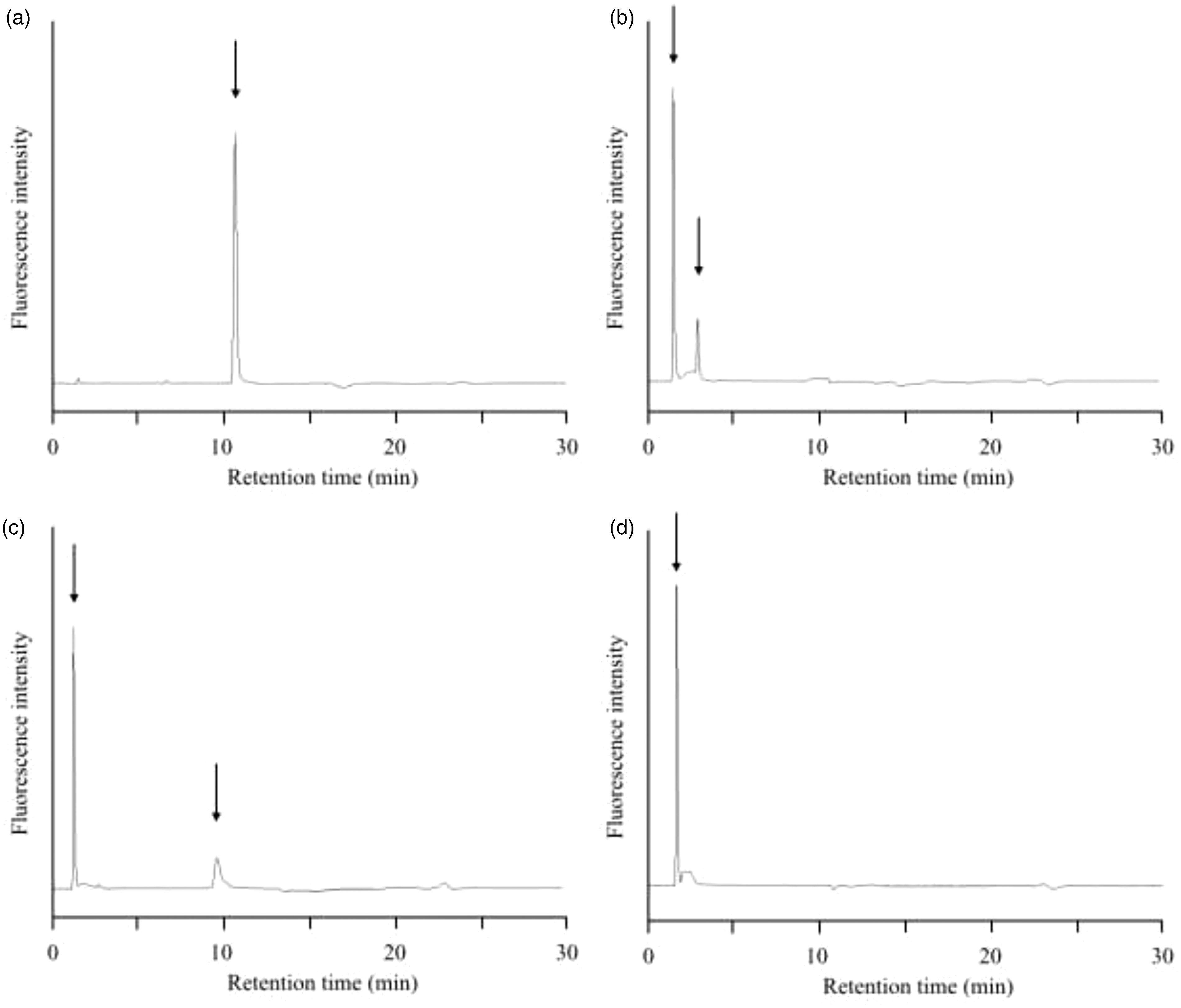
Influence of salts on the assay system
Comparison of THP concentration between salts added urine and non-added urine (100%).
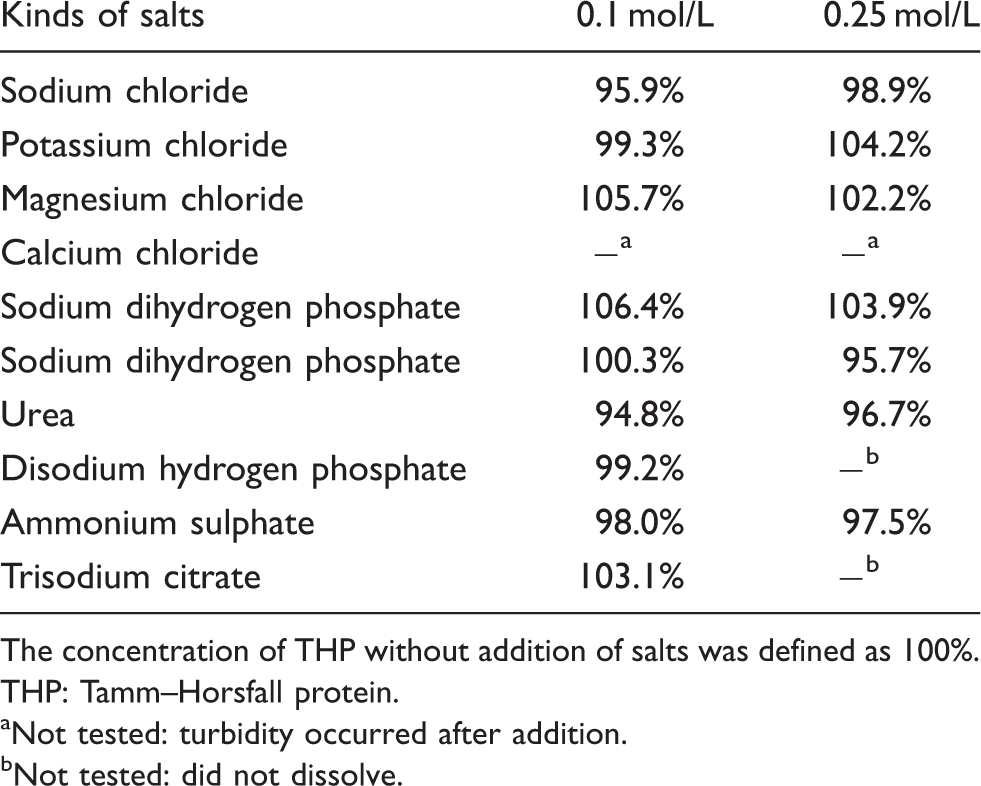
The concentration of THP without addition of salts was defined as 100%.
THP: Tamm–Horsfall protein.
Not tested: turbidity occurred after addition.
Not tested: did not dissolve.
The principle of the pretreatment method for urine samples is salting out. We examined how much urinary THP could be collected by this method. Furthermore, precipitates of THP were diluted by distilled water, but sodium chloride, which was added in the process of pretreatment, remained in this solution. We also evaluated the influence of residual sodium chloride on the HPLC assay system.
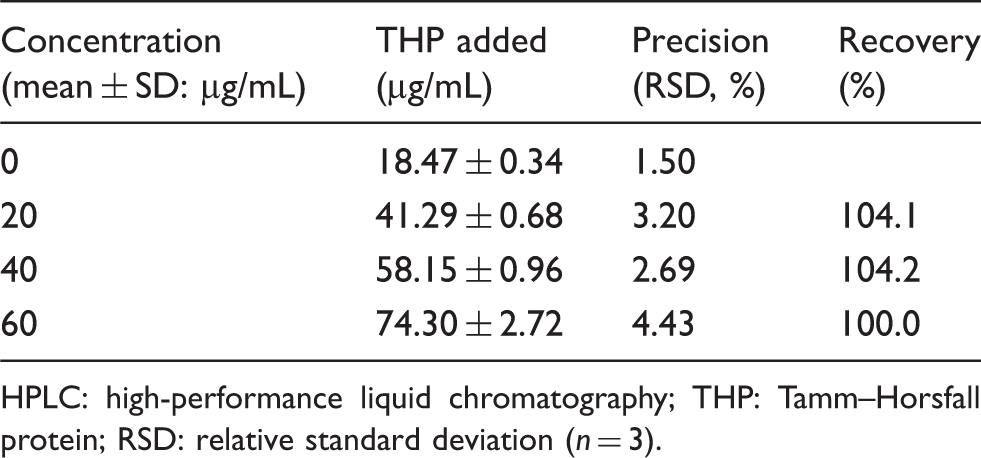
Influence of HPLC pretreatment on the recovery rate of the Tamm−Horsfall protein.
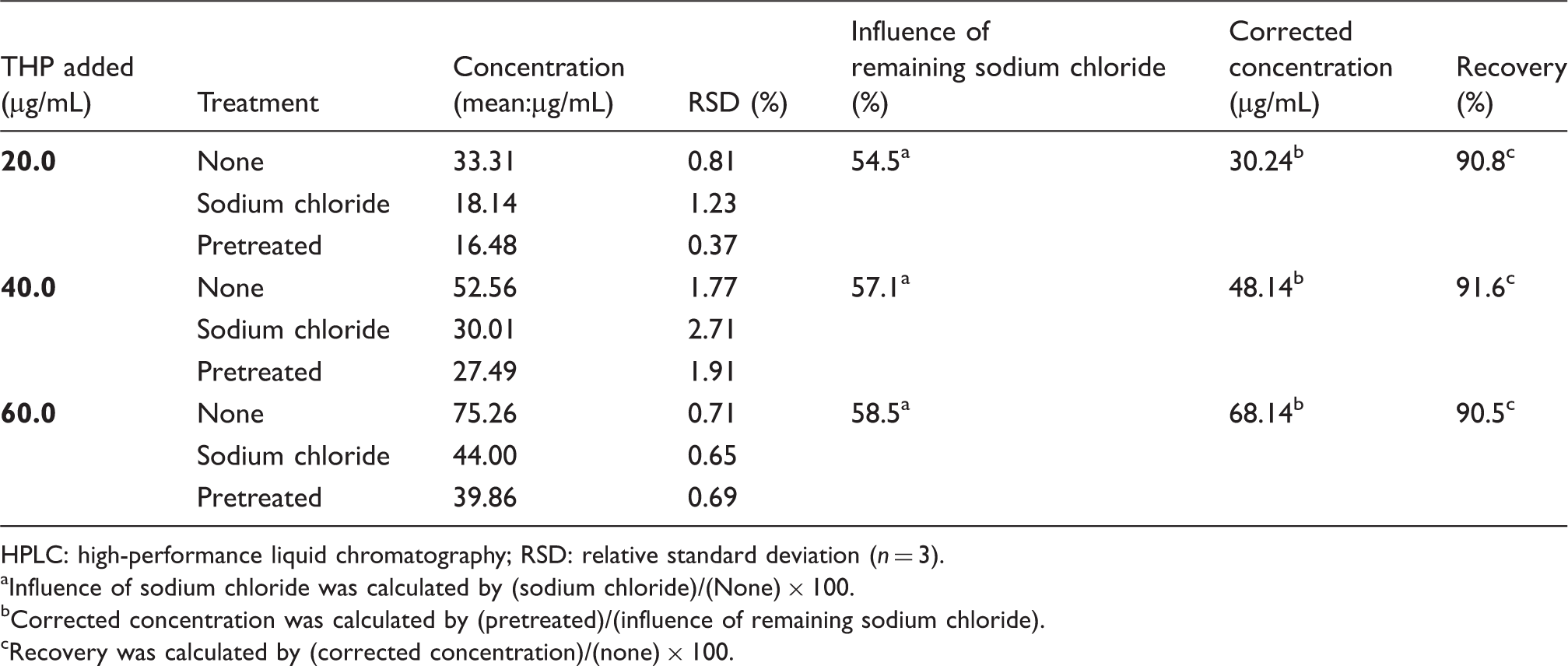
HPLC: high-performance liquid chromatography; RSD: relative standard deviation (n = 3).
Influence of sodium chloride was calculated by (sodium chloride)/(None) × 100.
Corrected concentration was calculated by (pretreated)/(influence of remaining sodium chloride).
Recovery was calculated by (corrected concentration)/(none) × 100.
Validation of the HPLC analytical method
Precision of the HPLC method for the measurement of the Tamm–Horsfall protein in human urine samples.
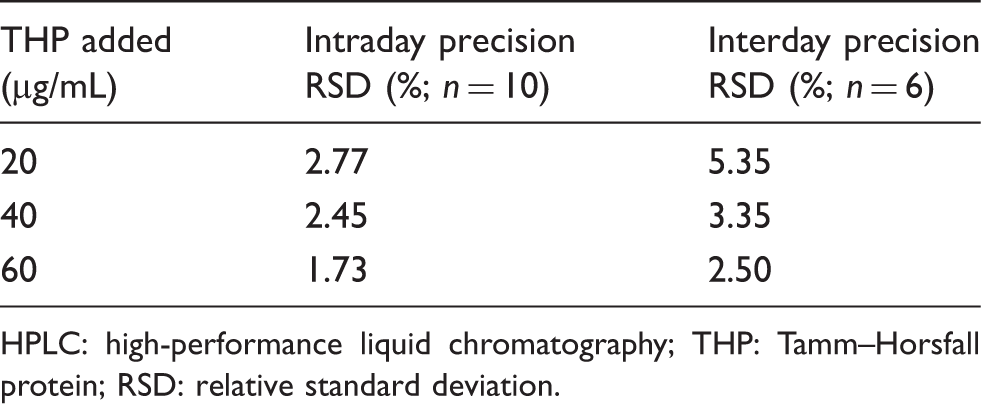
HPLC: high-performance liquid chromatography; THP: Tamm–Horsfall protein; RSD: relative standard deviation.
Accuracy of the HPLC method for the measurement of the Tamm–Horsfall protein in human urine.
HPLC: high-performance liquid chromatography; THP: Tamm–Horsfall protein; RSD: relative standard deviation (n = 3).
Correlation between HPLC and ELISA measurements of urinary THP in clinical samples
The measured value of HPLC was compared with those of a commercially available ELISA kit using urine samples from 28 clinical subjects. The HPLC values were corrected by correction factor calculated from the influence of sodium chloride. The QC samples (40 and 60 μg/mL standard THP solution) indicated that the HPLC values were about 3.4 times higher than the ELISA values (HPLC:ELISA = 39.37:11.99; 60.73:17.91 μg/mL). Therefore, the HPLC measurements were also corrected with this ratio. There was a strong correlation between the HPLC and ELISA values (y = 0.993x−0.8312; r = 0.906; Figure 4(b)).
Correlation between Tamm−Horsfall protein concentrations measured by present method (y) and ELISA (x). (a) Before correction, (b) the HPLC values were corrected in order to equalize the QC values of HPLC with the values of ELISA. ELISA: enzyme-linked immunosorbent assay.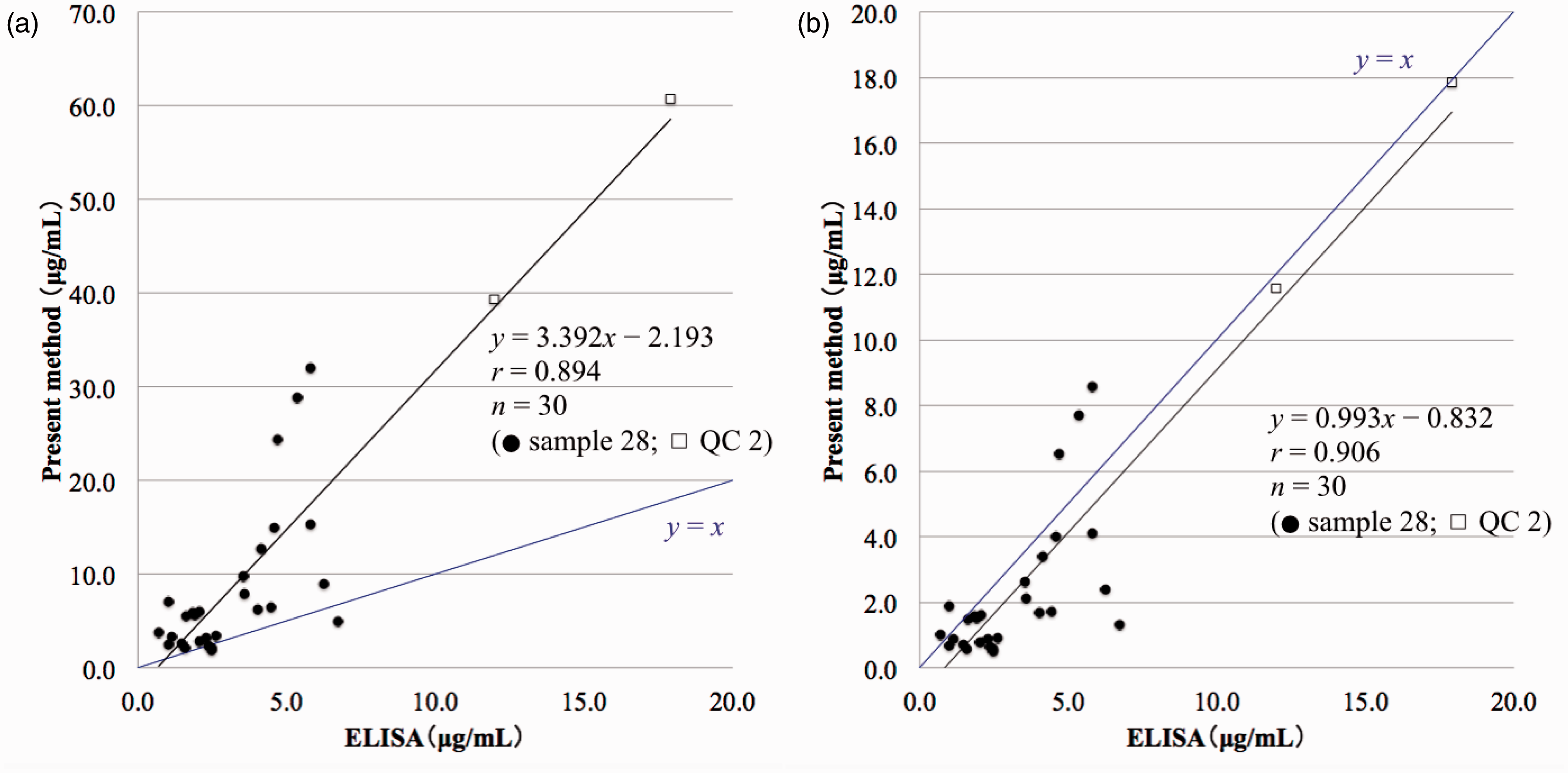
THP concentration in the urine of healthy individuals
When quantifying urinary proteins, it is better to use 24-h urine. However, there are many complicating factors. In general, the concentrations of compounds are expressed relative to the creatinine concentration. Therefore, we measured urinary creatinine in addition to THP. The mean THP concentration relative to the concentration of creatinine in 25 healthy volunteers with no history of kidney disease was 31.6 ± 18.8 mg THP/g creatinine.
Discussion
THP is the most abundant protein in urine (50%), followed by albumin (20%) and immunoglobulin (5%). 26 Urine samples were pretreated using the traditional salting-out method. This pretreatment method enables the isolation of the precipitate (urinary THP) from other proteins and compounds and its desalting. However, due to electrophoresis, the pretreated precipitates included other proteins in addition to THP. Albumin and γ-GLB exhibit a high affinity for THP.15,27 Hence, it was necessary to improve the ability of HPLC to separate the THP peak from those of other proteins to establish a quantitative method.
To determine the optimum HPLC conditions for separating urinary THP, we designed an elution method to retain only THP on the column by changing the concentration of acetonitrile. Furthermore, when column temperature rises, the viscosity of the mobile phase decreases and number of theoretical plates usually rises. However, we found that THP behaved in an opposing manner, which may be explained by an increase in peak width caused by THP aggregation inside the column due to temperature increase. Regarding the concentration of formic acid, the isoelectric point (pI) of THP (pI = 3.5) 28 is more acidic than those of albumin (pI = 4.7), γ-GLB (pI = 7.4) and transferrin (pI = 5.8). Therefore, the mobile phase was acidified with formic acid to decrease the polarity of THP, thereby increasing its adsorption by the stationary phase. These HPLC conditions enabled us to obtain a specific THP peak by separating it from those of urinary proteins that might co-precipitate and other urinary compounds.
Using our method, urine samples could not be injected directly into the HPLC column, because salts precipitate in the acetonitrile of Eluent B and obstruct the column. Thus, the salts in the samples must be removed as much as possible. Although dialysis is often used for sample desalting, it is unsuitable for many samples simultaneously. However, the pretreatment by salting out adopted in our method is simple and suitable for a large number of samples. Moreover, because the pretreated precipitate was dissolved in distilled water, the influence of the matrix was drastically reduced.
However, residual sodium chloride in the solution after pretreatment had a negative influence of approximately 50% on the measurement of the THP concentration using our method. We used pooled urine to evaluate the loss of THP and the influence of residual sodium chloride caused by pretreatment procedure. However, the influence might vary, because individual urine would contain different sodium chloride concentrations. A high concentration of sodium chloride was added to the urine in the process of pretreatment. This concentration is higher than that of the sodium chloride concentration originally existing in urine (4–14 g/L). Moreover, the precipitates were separated from the supernatant, which contains affluent sodium chloride and other unidentified influencing factors. For this reason, it is considered that sodium chloride, added in the process of pretreatment, has a greater influence than several salts included in the precipitate (originally existing in the urine). We also performed the same experiment using distilled water in place of pooled urine, and almost the same correcting factor was provided. Hence, these influences could be avoided by using a correcting factor.
On the other hand, as shown in Figure 1 Lane 4, the band of THP was observed in the supernatant after pretreatment. This means not all urinary THP precipitates by the pretreatment process. Actually, about 10% of urinary THP was uncollectible. Therefore, it is necessary to improve the pretreatment method to more accurately quantify urinary THP.
In the validation study, our method demonstrated high sensitivity and good linearity, precision and accuracy. A similar precipitation and HPLC protocol was found to be less sensitive (detection limit = 1 μg/mL) and less precise (intraday RSD = 10.4%) 21 than our protocol. Therefore, we developed a more sensitive and accurate HPLC method to measure urinary THP concentrations in clinical samples.
A strong correlation was observed between our HPLC-based method and ELISA. However, at low THP concentrations, the ELISA values tended to be lower than those obtained by HPLC. Actually, a few samples were below or near the detection limit of ELISA, which is likely due to the fact that ELISA samples were diluted 2000 times. Lau et al. 20 reported that 20% of their healthy individuals exhibited low THP concentrations on ELISA but not on SDS-PAGE. The false negatives reported by ELISA may have been due to the excessive sample dilution required to avoid the THP aggregation and urine matrix interference, by salts and acidic urine, 29 that prevents antigen recognition. However, our HPLC-based method avoided the need for sample dilution, allowing the detection of low THP concentrations over-looked by ELISA. The advantage of HPLC is that it can analyse THP both quantitatively and qualitatively. Moreover, HPLC is cost-effective, because it does not require special reagents, such as antisera, as compared with ELISA.
The concentrations of THP and other proteins in urine are affected by 24-h urine volume, urine flow rate and the degree of dehydration. 30 Hence, to eliminate these effects, we used the urinary creatinine concentration as a correction factor and expressed the THP excretion value as a THP:creatinine ratio (mg/g). A similar mean value (31 mg THP/g creatinine) was reported after THP precipitation and HPLC analysis in 42 healthy individuals. 21 Therefore, our HPLC-based method for the measurement of urinary THP is reliable, more sensitive and more accurate than previous HPLC-based methods.
Footnotes
Acknowledgements
We appreciate the technical support provided by the Research Support Center of the Graduate School of Medical Sciences at the Kyushu University.
Declaration of conflicting interests
None.
Funding
None.
Ethical approval
This study was approved by the Institutional Review Board of Kyushu University (Permission Number: 25-189).
Guarantor
YK.
Contributorship
MA researched the literature, conceived the study, completed the entire experiment, analysed the data and wrote the first draft of the manuscript. EH, EO and TT were involved in protocol development and assisted with data analysis. YK supervised MA and assisted with data analysis and manuscript drafting. All the authors reviewed and edited the manuscript and approved the final version of the manuscript.