
Abstract
Objectives
Fibronectin (FN) is able to bind fibrin and FN–fibrin complexes and is found in the plasma of some patients suffering from inflammatory disease. The present study was undertaken to determine whether soluble supra-molecular FN–fibrin complexes were present in the plasma of children with recurrent respiratory infections (RRI).
Design and methods
The frequency of occurrence and relative amounts of the supra-molecular FN–fibrin forms, concentrations of immunoglobulins and numbers of natural killer cells (NK) were determined in the plasma of children with recurrent respiratory infections. The frequencies of these parameters were compared with their frequencies in the plasma of children with acute respiratory infections and plasma from healthy children.
Results
SDS-agarose immunoblotting of patients’ plasma revealed the presence of several additional FN–fibrin bands, with decreasing electrophoretic mobilities and increasing molecular masses of 750 kDa, 1000 kDa, 1300 kDa, 1600 kDa and 1900 kDa. Such FN–fibrin complexes occurred with higher frequency and in larger amounts in the plasma of children with RRI and acute infection than they did in plasma from normal children. Moreover, bands above 1000 kDa were absent in most young healthy individuals. The occurrence of FN–fibrin complexes did not correlate with either immunoglobulin concentrations, or with the number of NK cells.
Conclusions
The occurrence of plasma supra-molecular FN–fibrin complexes is associated with acute and recurrent respiratory infections of children.
Introduction
Recurrent respiratory infection (RRI) is one of the most common and frequent diseases in children and adolescents. Its increased incidence in children is mainly related to constitutional (i.e. age of the child, immune system condition, congenital defects of respiratory system, concomitant diseases and allergies) and environmental factors, such as socio-economic conditions, increased exposure to infection, microbial virulence and overuse of antibiotics.1,2 In patients with RRI, it is more difficult to eliminate pathogens from the body and this can lead to an increased predisposition to recurrent infections. Consequently, RRI in childhood may increase susceptibility to diseases in adulthood, for example, asthma, diabetes, chronic bronchitis and emphysema. 3
Fibronectin (FN) is a large glycoprotein, and is present in significant amounts in plasma, cells and the extracellular matrix (ECM). It is involved in a wide variety of cellular functions, including cell adhesion, migration, proliferation and differentiation. 4 FN, secreted by hepatocytes, circulates in blood at varying concentrations in children, 5 and is involved in blood clotting, thrombosis, and wound healing processes.5,6 In the presence of endothelial injury, circulating FN enters the extravascular space and becomes incorporated into the ECM. 4 The binding of plasma FN to cellular integrin receptors leads to stretching of FN, leading to the formation of a fiber multimeric network. 7 An insoluble, cellular FN form, produced locally by fibroblasts, macrophages, lymphocytes, platelets and endothelial cells, accumulates locally in tissue, 4 where it is essential for the assembly and maintenance of the ECM, preserving its proper structural integrity, organization, and regulation of normal tissue metabolism. 8
The basic FN form is a 440–500 kDa dimer, made of two identical or similar disulphide-bonded polypeptide chains. Both FN polypeptides are composed of three types of repeating I, II and III modules which are arranged into independently folded functional domains with binding sites for ECM proteins (e.g. collagen), cell surface receptors (integrins, bacterial FN receptors), blood protein derivatives (e.g. fibrin) and glycosaminoglycans (e.g. heparin). 4 Additionally, an alternative splicing of mRNA leads to the inclusion of three extra domains (termed EDA, EDB and IIICS segments) to cellular FN, and only the IIICS segment to plasma FN.4,8
FN derived from different cell types displays high structural and functional heterogeneity, which may result primarily from alternative splicing of its pre-mRNA and different degrees of post-translational N- and O- glycosylations. 9 Moreover, FN has an ability to form cross-linked complexes with, for example, FN fragments, 10 various extracellular matrix components, 8 and some blood plasma components such as fibrin and fibrinogen, 5 creating high-molecular FN forms. The FN forms with increased molecular masses were shown to be produced by carcinoma cell lines in vitro.11,12 In a previous study, we have observed the high molecular FN forms, following SDS-PAGE under reducing conditions, in the plasma of patients with neurodegenerative diseases, 13 and plasma and pleural effusions of some patients with lung cancer and lung inflammation, 14 and also of elderly individuals. 5 These FN forms were identified as the subunits of soluble supra-molecular plasma FN–fibrin complexes, which were easily revealed by SDS-agarose immunoblotting. 15
The present study was undertaken to determine whether the soluble supra-molecular FN–fibrin complexes occurred in the plasma of children suffering from RRI. The frequency of occurrence and relative amounts of supra-molecular FN–fibrin forms in the plasma of children with RRI, during the period of recovery, stratified by immunoglobulin concentration and number of natural killer (NK) cells were compared to their frequency in those children with acute infection and to their frequency in healthy children.
Materials and methods
Sampling
Blood samples, anti-coagulated with sodium citrate, were collected from 94 children under the medical care of the 3rd Clinic of Pediatrics, Immunology and Rheumatology, of Developmental Age of Wroclaw Medical University (Poland). The samples were collected with the informed consent of parents of children and the study was approved by the local ethics committee (Commission of Bioethics at Wroclaw Medical University, no. KB-445/2012). Plasma was prepared by centrifugation for 15 min at 2000 g and +4 ℃. The samples were stored at −76 ℃ until use. All samples included in the studies consisted of excess plasma remaining after all routine laboratory investigations had been completed.
Characteristics of the groups of children with recurrent respiratory infection and blood parameter findings.
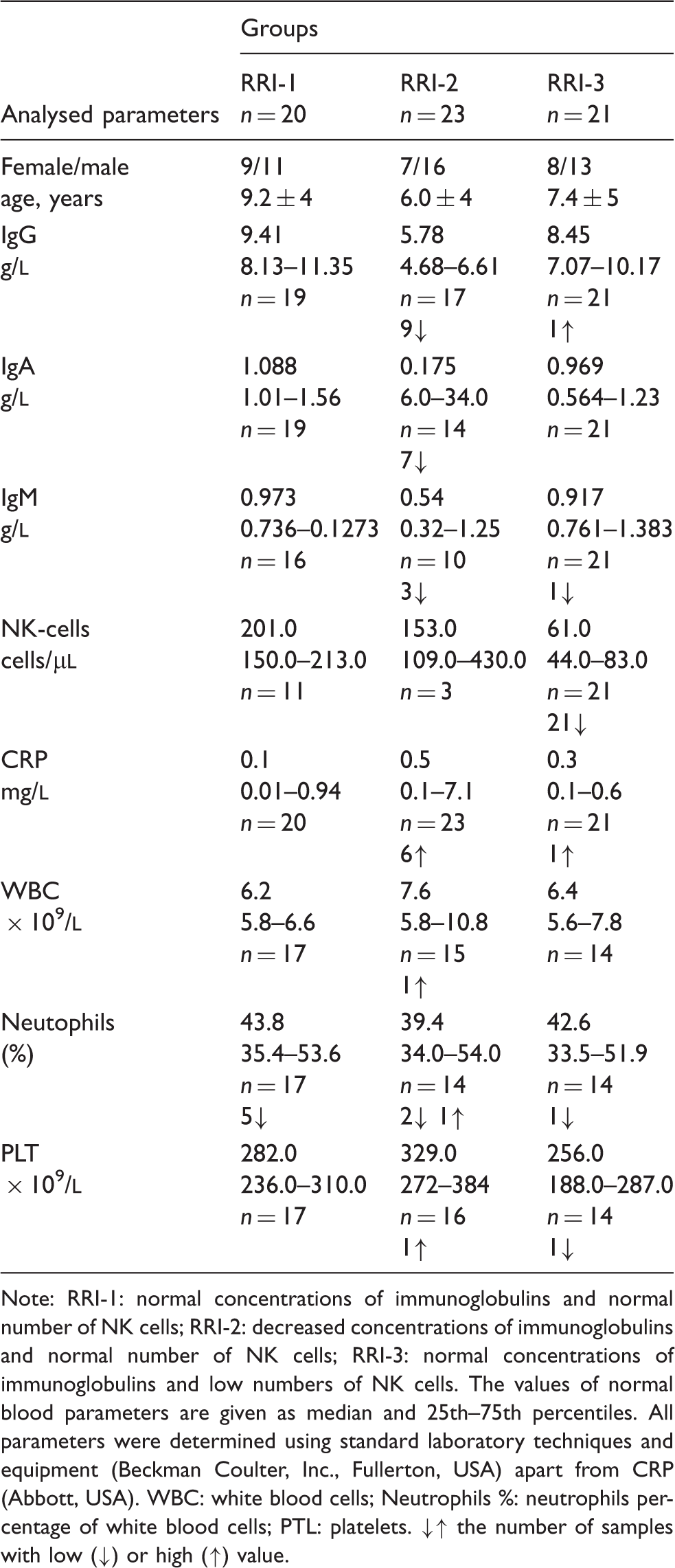
Note: RRI-1: normal concentrations of immunoglobulins and normal number of NK cells; RRI-2: decreased concentrations of immunoglobulins and normal number of NK cells; RRI-3: normal concentrations of immunoglobulins and low numbers of NK cells. The values of normal blood parameters are given as median and 25th–75th percentiles. All parameters were determined using standard laboratory techniques and equipment (Beckman Coulter, Inc., Fullerton, USA) apart from CRP (Abbott, USA). WBC: white blood cells; Neutrophils %: neutrophils percentage of white blood cells; PTL: platelets. ↓↑ the number of samples with low (↓) or high (↑) value.
FN concentration
FN concentration was determined by an enzyme-linked immunosorbent assay (ELISA) using a well-defined domain-specific monoclonal antibody directed to a centrally located cell-binding domain of FN (FN30-8; M010 TaKaRa Shuzo Co. Ltd., Shiga, Japan) as described earlier. 16
Western immunoblotting
Plasma samples containing 300 ng of FN were subjected to SDS-polyacrylamide gel electrophoresis under reducing conditions and immunoblots prepared as described earlier. 16 The immunoblots were scanned and protein band patterns were analysed by densitometry using GelScan V6.0 (BioSciTec GmbH, Frankfurt/Main, Germany).
SDS-agarose FN immunoblotting
Supramolecular forms of plasma FN were revealed by SDS-agarose immunoblotting as described previously. 15
Statistics
Data are presented as means ± standard deviations (SD). Comparisons between groups were performed by means of the Kruskal–Wallis and post hoc tests. P < 0.05 was regarded as significant.
Results
FN reduced bands
Electrophoresis followed by immunoblotting revealed the presence of a high molecular ∼280 kDa FN reduced band, in addition to the normal FN subunit of ∼240 kDa (Figure 1).
Representative immunoblotting pattern of plasma FN of children suffering from RRI. SDS-PAGE was done under reducing conditions in 5% gel. The immunoblots were developed with monoclonal antibody directed to cellular binding domain FN (TaKaRa Shuzo Co. Ltd., Japan) as described by Pupek et al.
16
In all cases, 300 ng of FN was applied per lane. The immunoblotting was done for all 94 plasma samples, but only the representative patterns of plasma FN are shown: RRI-1 (lane 1), RRI-2 (lane 2), RRI-3 (lane 3), normal plasma of child (lane 4).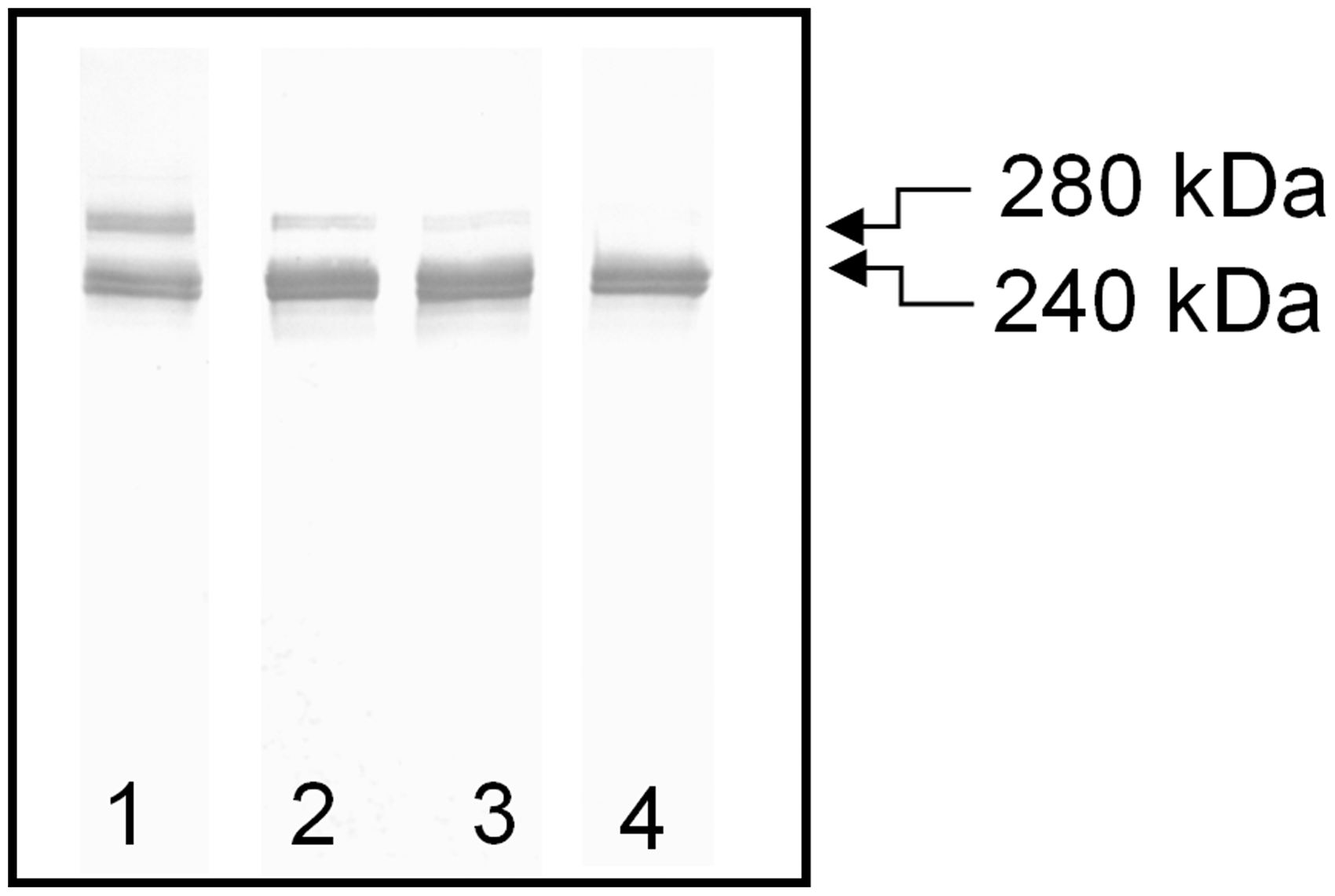
FN concentration and occurrence of reduced FN form in plasma of children.
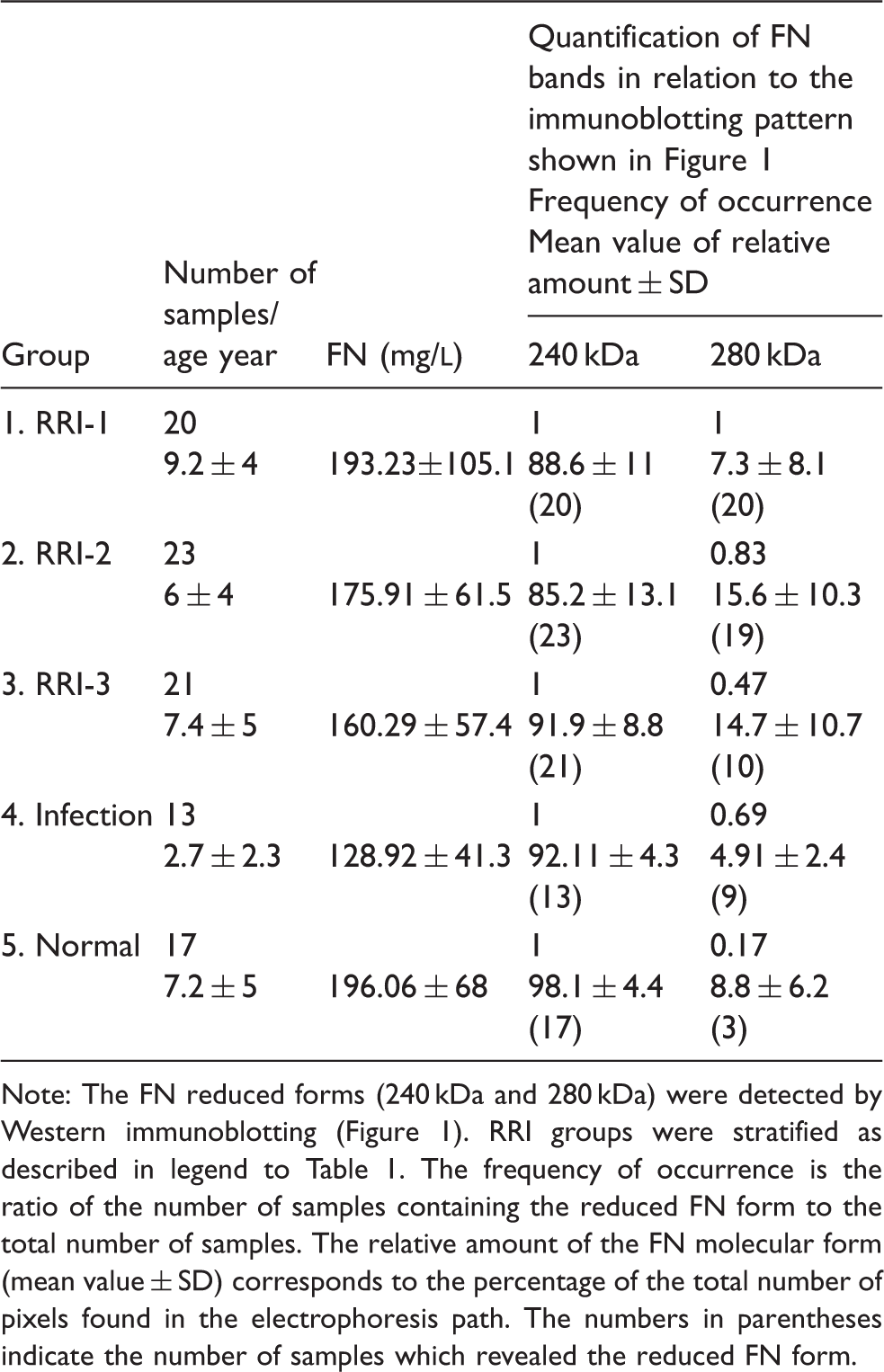
Note: The FN reduced forms (240 kDa and 280 kDa) were detected by Western immunoblotting (Figure 1). RRI groups were stratified as described in legend to Table 1. The frequency of occurrence is the ratio of the number of samples containing the reduced FN form to the total number of samples. The relative amount of the FN molecular form (mean value ± SD) corresponds to the percentage of the total number of pixels found in the electrophoresis path. The numbers in parentheses indicate the number of samples which revealed the reduced FN form.
FN multimers
SDS-agarose immunoblotting revealed the presence of several bands with decreasing electrophoretic mobilities (Figure 2a). The band of 500 kDa was a dimer of FN, whereas the bands of 750 kDa, 1000 kDa, 1300 kDa, 1600 kDa and 1900 kDa recognized by anti-FN monoclonal antibody and anti-fibrinogen polyclonal antibodies (Figure 2b) corresponded to the supramolecular FN–fibrin complexes I–V.
SDS-agarose immunoblotting of FN and FN–fibrin complexes in plasma of children with RRI. Electrophoresis (300 ng of FN per lane) was undertaken in 1.5% agarose gel under non-reducing conditions and the blots were developed with anti-FN monoclonal antibody (FN30-8; TaKaRa Shuzo Co. Ltd., Japan).
15
(a) Groups: RRI-1 (lane 1), RRI-2 (lane 2), RRI-3 (lane 3); infection (lane 4); normal plasma of child (lane 5) and a commercial plasma FN preparation (lane 6). Molecular masses of standards: Polymers of von Willebrand factor (vWF: 900 kDa, 1350 kDa, 1800 kDa and 2250 kDa) and commercial plasma FN preparation (240 kDa). (b) Reactivity of normal plasma with anti-FN monoclonal antibody (FN) and antiserum directed to human fibrinogen (Fb).15,17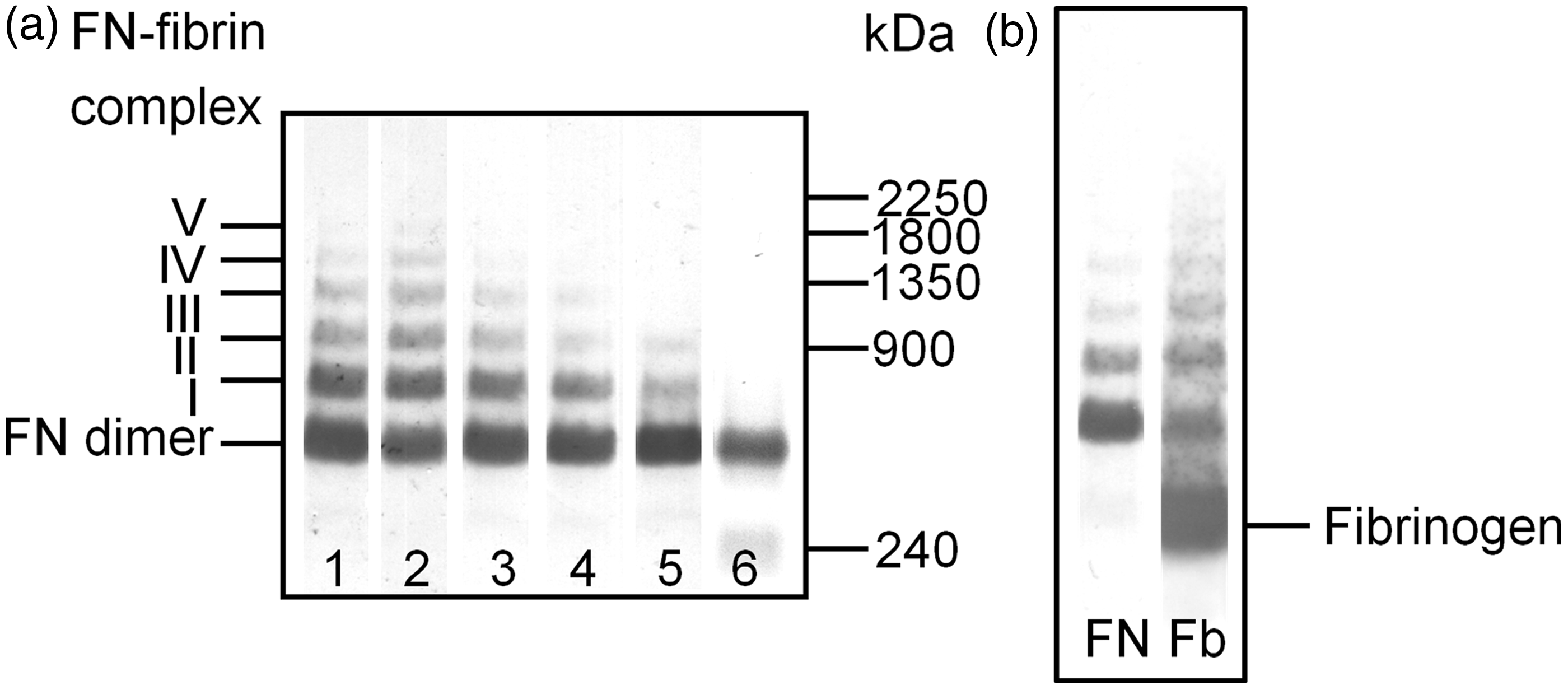
Frequency of occurrence of bands in FN multimers in blood plasma of children suffering from recurrent respiratory infection.
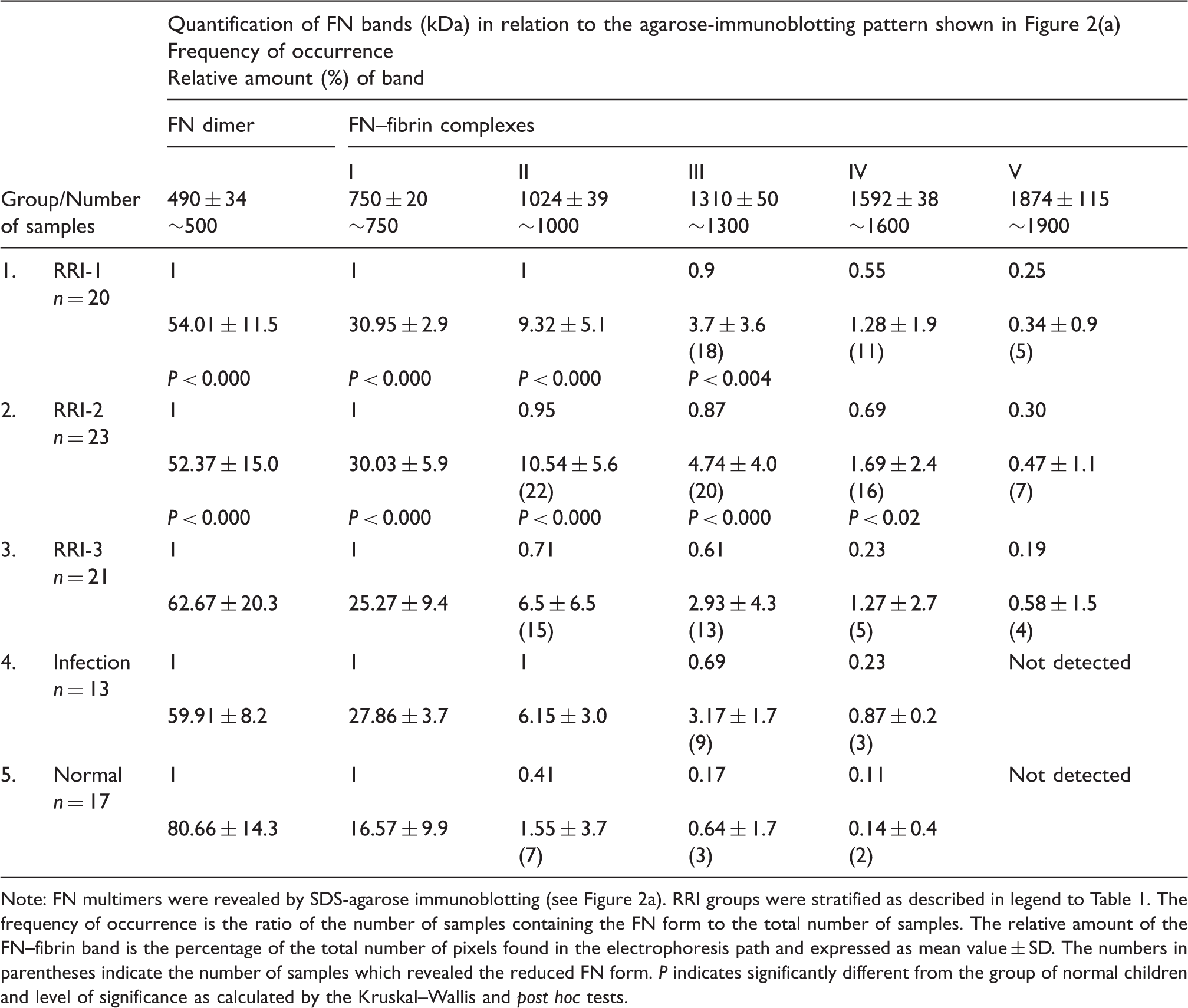
Note: FN multimers were revealed by SDS-agarose immunoblotting (see Figure 2a). RRI groups were stratified as described in legend to Table 1. The frequency of occurrence is the ratio of the number of samples containing the FN form to the total number of samples. The relative amount of the FN–fibrin band is the percentage of the total number of pixels found in the electrophoresis path and expressed as mean value ± SD. The numbers in parentheses indicate the number of samples which revealed the reduced FN form. P indicates significantly different from the group of normal children and level of significance as calculated by the Kruskal–Wallis and post hoc tests.
Discussion
In the present study, we found that the soluble-supra-molecular plasma FN–fibrin complexes, normally absent in most young healthy individuals, occurred with high frequency in the plasma of children with acute infection and recurrent respiratory infections (RRI). However, their occurrence in the plasma of children with RRI did not correlate with either immunoglobulin concentrations or the number of NK cells.
The SDS-agarose FN immunoblotting pattern (Figure 2(a), Table 3) showed that FN present in the plasma of children with respiratory infection consists of a mixture of native dimeric FN (band of ∼500 kDa, a normal constituent of blood plasma) and a series of supramolecular FN–fibrin complexes visible as the ladder of bands with increasing molecular masses of ∼750-, ∼1000-, ∼1300-, ∼1600 and ∼1900-kDa, which were recognized by anti-FN and anti-fibrinogen antibodies (Figure 2b). As discussed earlier, 15 these FN–fibrin complexes differed from the adjacent one by ∼280 kDa, which corresponded to the mass of one FN reduced subunit crosslinked with a fibrin fragment (Figure 1; Table 2).
The absence of any significant differences in FN–fibrin patterns among children in Groups 1 and 2, and those in Group 4 (Figure 2; Table 3) suggests that the qualitative and quantitative changes in the FN–fibrin complex profile is not related to the ability of the immunological system of children to respond to infection agent stimulation. Moreover, the finding that the plasma FN concentration in the childrens’ groups were in the reference interval (Table 2) suggests that the presence of abnormal FN forms was not related to either the rate of synthesis of FN or the release of the abnormal forms from immunological cells. We believe that the observed pattern may reflect a molecular connection between inflammation and activation of the coagulation cascade. Infection is known to provoke inflammation, and therefore might lead to injury and to malfunctions of inflamed tissue, particularly in children.18,19 Bacterial products and/or pro-inflammatory cytokines are able to elicit pro-coagulant reactions activated primarily by the tissue factor pathway. Tissue factor binds and activates clotting factor VII, which via factor X results in the generation of thrombin. 20 Thus, after activation of a coagulation cascade, during enhanced thrombotic processes, fibrinogen undergoes conversion to fibrin and its fragments, which might form complexes with plasma FN.6,21 The FN can be covalently crosslinked by factor XIIIa through an isopeptide bond to the carboxyl terminal compact and flexible αC-domain of fibrin,21,22 creating soluble FN–fibrin hetero-complexes easily revealed by agarose immunoblotting. 15 In contrast, in healthy individuals, FN and fibrinogen circulate in the blood independently (binding sites on fibrinogen for FN are concealed); thus they are unable to interact and therefore the FN–fibrin complexes should not be observed. 21 Indeed, such FN–fibrin complexes were absent in most of the normal adult samples, 15 although in this study, they were present in a few samples taken from children in the normal group, Group5. However, it should be realized that samples within our normal group were collected from children visiting a doctor for non-infection events. We have previously shown that the FN–fibrin complexes, particularly those with lower molecular masses of ∼750 kDa and ∼1000 kDa, can occur in some normal samples taken from physically healthy individuals and having normal biochemical and haematological parameters. 15
Whilst RRI can cause either acute, chronic or transitional destruction states of the structure of the respiratory epithelium, our results show the molecular consequences of respiratory infections at the level of activation of inflammatory and coagulation systems. The occurrence of a 280-kDa FN–fibrin reduced form and multiple FN–fibrin complexes seems to be a dynamic and transient process related to pathophysiological events probably connected with normal haemostasis. 15 The occurrence of FN–fibrin complexes being evidently associated with inflammatory disease probably reflects FN involvement in the tissue repair process. However, on the other hand, the occurrence of supra-molecular multimers of FN–fibrin complexes carries a risk of disseminated intravascular coagulation in conditions of pro-coagulant states, inhibition of fibrinolysis and consumption of coagulation inhibitors. 23 Such a state might lead to FN–fibrin deposition in the microvasculature and emerging thrombotic micro-angiopathic events. We believe therefore that the findings of this study may have beneficial clinical consequences and prove helpful in the management of therapy, particularly in children with RRI.
Footnotes
Acknowledgements
We thank Dr Leszek Noga for statistical consultations.
Declaration of conflicting interests
None.
Funding
This study was funded by grants from the Wrocław Medical University (PBm6).
Ethical approval
The study was approved by the Commission of Bioethics at Wrocław Medical University (no. KB-445/2012) and conformed to the Helsinki Declaration.
Guarantor
K-PI.
Contributorship
PB was involved in patient recruitment, diagnosis, and written consent. L-PA and K-GD were involved in laboratory work, measuring the parameters, analysis and interpretation of its results. K-PI and L-PA wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.