
Abstract

We read with interest recent postings on the ACB mailbase relating to seasonal pseudohypokalaemia. 1 At this time, we had noted an apparent increase in the incidence of hypokalaemia in samples from general practices (GP) analysed at University Hospital of Wales (UHW). Internal quality control monitoring revealed no shift in mean values on the analysers. The monitoring of daily patient means for all samples showed a decrease in mean potassium values for July 2013 and this prompted further investigation.
A retrospective data gather was performed for 10 working days 8–19 July 2013 inclusive, a period of prolonged higher than average daily temperatures. 2 Data were also requested for 10 working days 9–20 July 2012 inclusive, during which temperatures were similar or cooler than average. 2 Only samples from GP and UHW patients were included. Samples from outpatients were not differentiated from inpatients as there should be minimal delays in sample receipt in the laboratory. Statistical analyses were performed using IBM SPSS Statistics.
Mean potassium and incidence of hypokalaemia in comparative 10 working-day periods in July 2012 and July 2013.
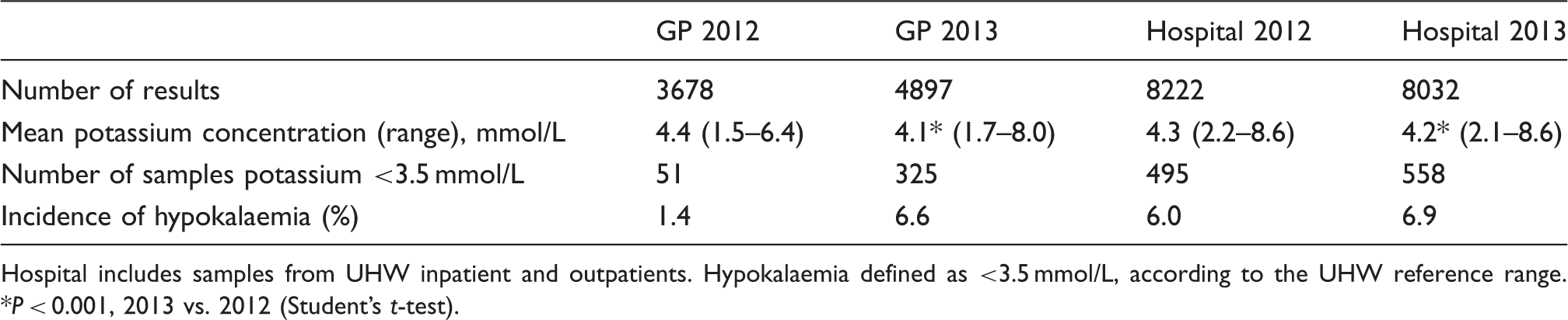
Hospital includes samples from UHW inpatient and outpatients. Hypokalaemia defined as <3.5 mmol/L, according to the UHW reference range. *P < 0.001, 2013 vs. 2012 (Student’s t-test).
These findings confirm an increased frequency of hypokalaemia in GP patients during July 2013, consistent with a contribution from prolonged higher than average ambient temperatures. The phenomenon of seasonal pseudohypokalaemia has been reported previously in GP samples during the summer months3–5 and appears to be related to increased Na+-K+-ATPase activity. 3 Interestingly, we also observed a shift in mean potassium of a smaller magnitude in hospital patients, similar to a previous report. 4 The effects of pseudohypokalaemia are likely to include time, cost, patient inconvenience and worry. 3 Seasonal pseudohypokalaemia should therefore be considered as a potential cause for unexplained hypokalaemia during hot weather. The possibility of pseudonormokalaemia masking hyperkalaemia is difficult to quantify but may have been significant during this period.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
SZ.
Contributorship
SZ conceived the study. KLJ analysed the data and prepared the first draft of the manuscript. Both authors reviewed, edited and approved the final draft.
Acknowledgements
The authors thank IT staff for performing the data gather.