
Abstract
Context
Heterophilic antibodies are a well-described interferent but poorly appreciated and are often not a recognized problem affecting most immunoassays. We describe for the first time heterophilic antibodies interference affecting an adrenocorticotropic hormone (ACTH) assay in a patient with Cushing’s syndrome due to bilateral nodular adrenal hyperplasia.
Case
A 60-year-old retired female nurse underwent extensive invasive investigations, which were ultimately unnecessary, as a result of initial analytical interference in the ACTH assay, which could not be resolved using a proprietary heterophilic binding reagent.
Results
This case highlights the inherent difficulty of diagnosing Cushing’s syndrome and the large emphasis placed on laboratory tests. The consequence of not initially identifying interference in this patient’s laboratory test results led to unnecessary and costly investigations with potentially adverse outcomes.
Conclusions
Clinicians and the laboratory community need to be continuously vigilant and view laboratory results with caution when they are inconsistent with the clinical picture. This approach is paramount, especially at a time of increasing automation and ever-diminishing scientist involvement in sample processing.
Introduction
Since the description of the first immunoassay in 1959 by Nobel Laureates Berson and Yalow, 1 this technology has matured and taken on a central role in clinical laboratories. However, the use of non-human antibodies can produce erroneous results with serious clinical diagnostic and management consequences. One of the relatively well-recognized causes of analytical error is heterophilic antibody interference. 2 Heterophilic antibodies are proteins that bind animal antigens.3–6 They may be endogenous antibodies or autoantibodies, usually polyspecific, and show low affinity with weak binding to a heterogeneous group of antigens. 5 Immunometric assays that utilize non-human cells to manufacture analytically useful antibodies introduce an inherent risk that a patient’s sample with endogenous heterophilic antibodies could react in a similar fashion to the analyte of interest resulting in positive assay interference. Positive assay interference could occur when heterophilic antibodies bridge the capture and detection assay antibodies, resulting in elevated analyte results. Rarely, heterophilic antibodies can also lead to false negative or low analyte results due to interfering with analyte binding to either capture or detection antibodies.3–6 We describe a patient with Cushing’s syndrome who underwent extensive but ultimately unnecessary investigations as a consequence of initial erroneous laboratory results due to heterophilic antibody interference in the Siemens Immulite 2000Xpi adrenocorticotropic hormone (ACTH) assay.
Subject, methods and results
A 60-year-old retired female nurse with a history of hypertension and depressive illness presented following the diagnosis and treatment of breast cancer which was deemed to be in clinical remission. The patient was noted to have bilateral adrenal gland enlargement on a recent abdominal CT scan. On initial presentation, there were a few clinical features suggestive of glucocorticoid excess; however, over the subsequent 12 months, classic features of Cushing’s syndrome developed including hypertension, weight gain, bruising and moon facies. Bone mineral density evaluated using dual-energy X-ray absorptiometry (DEXA) scan confirmed osteoporosis with lumbar spine and left total hip T-scores of 3.4 and 2.9, respectively.
Initial investigation for Cushing’s syndrome.

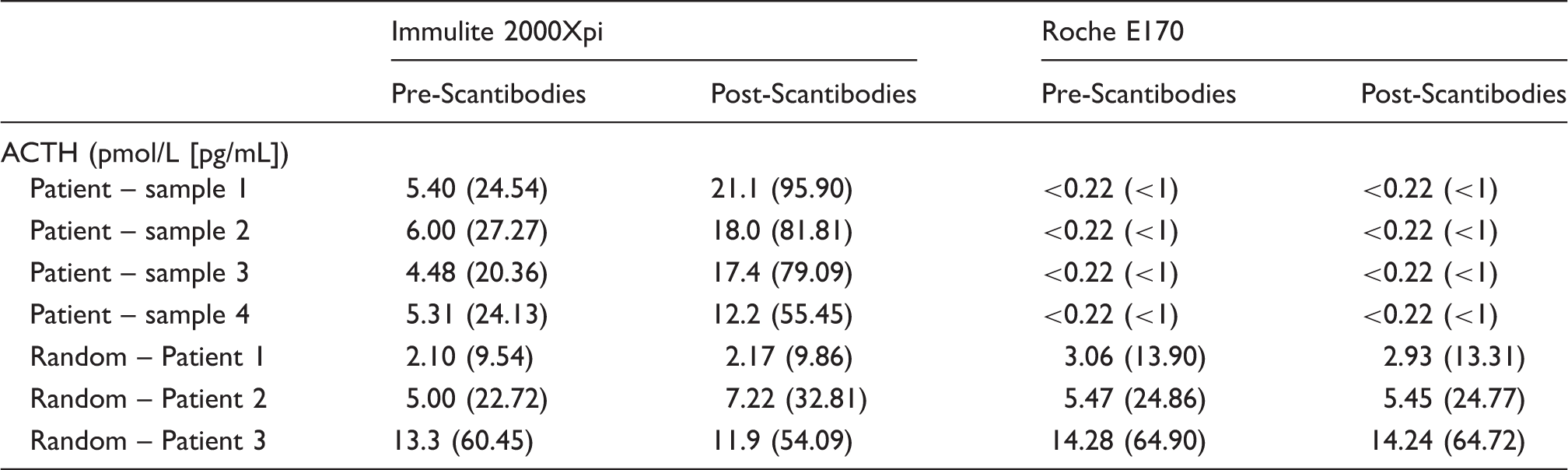
Patient’s samples tested for heterophile antibodies with Scantibody tubes and three unrelated patients’ samples.
The patient proceeded to a right unilateral adrenalectomy. A well-circumscribed nodule measuring 23 × 17 × 23 mm with a variegated brown and golden yellow cut surface was seen on macroscopic examination. Microscopic assessment showed a well-defined, but unencapsulated nodule composed of nests of large polygonal eosinophilic cells with fairly uniform round nuclei and an intervening delicate fibrovascular network. The lesion exhibited no malignant features. The histological changes were consistent with a dominant adrenal nodule arising in the background of nodular adrenal hyperplasia. Post-surgical urine-free corticoids were 360 nmol/d (<900), and at 8:00, the serum cortisol was 240 nmol/L (150–700) confirming biochemical normalization.
Discussion
Difficulties with interfering antibodies have been recognized since the advent of immunoassays and manufacturers have striven to improve assay performance by routinely integrating a multitude of blocking agents. 4 Due to the heterogeneity of different interfering antibodies, no single routine test is available to identify heterophilic antibodies. 8 We describe the first case of heterophilic antibody interference with ACTH analysis identified at our laboratory network or reported in the medical literature. The importance of identifying heterophilic antibody interference in this case was twofold: extensive, unnecessary investigations were undertaken as a result of the persistently detectable ACTH and initially pituitary surgery as a therapeutic option was considered. This case highlights the need for the laboratory and clinician to closely interact and consider the possibility of interfering heterophilic antibodies when immunoassay results are discrepant from other available laboratory and clinical information.
The prevalence of heterophilic antibodies is unknown but has been postulated to vary widely depending on assay antibody formation and patient-specific factors (<1–80%). 3 Although 40% of samples contain non-analyte substances that bind to assay antibodies, 5 analytically important heterophilic antibodies are most likely occur in about 0.5–3% of the specimens tested.4,9 A patient can form heterophilic antibodies at any time when exposed to ‘foreign’ antigens. Most notable exposures are iatrogenic, for example during vaccination, antibody-targeted therapies and antibody-targeted imaging reagents.3–6 Further confusion results from the knowledge that heterophilic antibodies can be transient, making interpretation and detection more difficult. 5
ACTH concentrations in our case patient were persistently within the reference interval, (2.0–10 pmol/L), with values ranging between 3 and 6 pmol/L and in concert with markedly raised total urine corticoids, and these results were consistent with ACTH-dependent Cushing’s syndrome.10,11 The expected incidence of Cushing’s syndrome depends on the population studied, with data ranging from 0·7 to 2·4 per million population per year. 12 In our West Australian population, approximately 5–10 new cases are diagnosed per year following screening tests of approximately 800 patients annually. The lack of complementary and confirmatory laboratory tests makes identification of Cushings’ syndrome difficult. Subsequent IPSS excluded a central to peripheral gradient, the expected outcome with pituitary ACTH production and was the principal reason to investigate for heterophilic antibodies prior to recommending unilateral or bilateral adrenalectomy.
Investigation of plasma samples for heterophilic antibodies were undertaken using heterophile blocking tubes (Scantibodies®) to remove any interfering antibodies. Such proprietary Scantibodies® tubes have a specific binder called heterophilic blocking reagent (HBR) which inactivates heterophilic antibodies. The raised ACTH values obtained after preincubation with Scantibody tubes were initially unexpected. A possible explanation for this finding may be that the pretreatment removed weakly reactive, polyspecific IgG class antibodies, leaving the remaining higher affinity monospecific IgM class antibodies to bind more avidly to the analyte antibodies, resulting in even higher assay results. The definitive test was analysis by a different method that utilizes different capture and recognition antibodies. When this was performed on our patient, no interference was noted in both the neat and post Scantibody-treated samples, resulting in consistently undetectable ACTH concentrations. Whilst we cannot exclude the possibility that the inference was due to something other than heterophilic antibodies, the fact that the use of Scantibody tubes altered the results indicates to us that an antibody-based interference is most likely.
Conclusions
We describe a patient with Cushing’s syndrome due to bilateral nodular adrenal hyperplasia and heterophilic antibodies resulting in falsely measurable ACTH results leading to unnecessary and potentially harmful investigations. Targeted investigations using heterophilic blocking (Scantibody) tubes failed to detect heterophilic antibody interference on the Siemens Immulite 2000Xpi ACTH assay, but IPSS and AVS findings plus repeat ACTH immunoassay using an alternative method led to the correct diagnosis of ACTH independent Cushing’s syndrome. Clinicians and the laboratory community need to be vigilant and view laboratory results with caution when they are discordant with the clinical picture. This approach is paramount, especially at a time of increasing automation and ever-diminishing scientist involvement in sample processing.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Patient consent obtained. No ethic approval required as all tests performed were part of routine investigation and management.
Guarantor
SV.
Contributorship
JB was the attending physician. JG, SV and PG conceived the study. RW analysed the samples and data. SF analysed the surgical samples. JG wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.