
Abstract
Background
There is general agreement that the lower limit for postprandial venous plasma glucose is the same or higher than for a fasted sample. The finding of a postprandial fall in glucose would therefore have implications for assignment of the lower limit of the normal glucose range.
Methods
An antecubital venous sample was collected before and one hour after breakfast. Plasma was separated immediately after collection and glucose measured using the hexokinase method. Participants with dysglycaemia were excluded from subsequent analysis.
Results
Glucose range (mmol/L) for the 96 participants was 4.4–6.0 fasting and 2.7–7.2 postprandially. There was no relationship between postprandial glucose and either gender or carbohydrate intake. About 24% of postprandial concentrations were <3.9 mmol/L.
Conclusions
If laboratories choose to define a random venous plasma glucose reference range, the lower limit should be below 3.9 mmol/L.
Introduction
In contrast to many other analytes, defining a value for the lower cut-off for random venous plasma glucose in healthy individuals is difficult. 1 Broadly agreed parameters would however suggest that >3.9 mmol/L is unequivocally normal and <3.0 mmol/L is abnormal, 1 and that results between these values should be interpreted within their clinical context. This presents a dilemma for the clinical biochemist when asked to interpret a random venous plasma glucose value <3.9 mmol/L, in the absence of symptoms and signs of hypoglycaemia. This study aims to add to our knowledge of the random glucose range by describing the one hour post breakfast venous plasma glucose results from healthy individuals, obtained as part of a previous study. 2
Methods
Healthy non-diabetic volunteers aged 18–45 years were recruited as part of a previous study of venous plasma-capillary glucose differences. 2 Participants attended a morning research clinic after a minimum fast of 8 hours. Antecubital venous blood samples were collected fasting and approximately one hour after breakfast, which consisted of a choice of foods with known carbohydrate content. Participants ate ‘to appetite’. A medication history was obtained, as some medications are known to influence plasma glucose. 3 Venous samples were centrifuged immediately after collection, plasma was separated then assessed during a routine laboratory ‘run’ using the glucose hexokinase method on the Abbott ci8200 automated analyser (Abbott laboratories, Chicago, IL, USA), coefficient of variation <2%. Additional methodology is described in detail elsewhere. 2
Statistical comparisons were undertaken using unpaired two tailed t-tests, simple linear regression and χ2 tests. P < 0.05 was considered to be significant. Local Ethics Committee approval was obtained.
Results
The current study excluded seven of the initial 103 participants because of evidence of dysglycaemia, defined as a fasting glucose >6.0 mmol/L and/or postprandial glucose >7.8 mmo/L; however, no formal diabetic screening tests such as an oral glucose tolerance test or haemoglobin A1c were performed. One participant experienced dizziness and nausea 90 min after breakfast, was pale but had normal vital signs. Postprandial glucose was subsequently found to be 2.7 mmol/L. Six months later, symptoms had not recurred, thus her result was considered to be physiological and was included on this basis. No other participants developed symptoms. Participants excluded because of dysglycaemia were older (mean age 36.3 years) than the remaining 96 participants. There was otherwise no difference in measured characteristics between these two subgroups of participants.
Of the 96 participants, 41 were male and 55 female. The mean (SD) age was 27.0 (6.9) years; mean (SD) carbohydrate intake was 89.1 (41.8) g; mean fasting and postprandial glucose (range) concentrations were 5.2 (4.4–6.0) and 4.5 (2.7–7.2) mmol/L respectively, with a mean prandial change of −0.70 mmol/L. The postprandial glucose median (interquartile range) was 4.3 (3.9–4.9) mmol/L. The 5th and 95th percentiles for postprandial glucose (mmol/L) were 3.3 and 6.6, respectively. Results were subanalysed by gender, because of known gender differences in carbohydrate intake, 2 and glucose.1,4,5 Mean fasting glucose was lower in women (5.1 mmol/L) than men (5.3 mmol/L), P = 0.03. There were no significant gender differences for age (t = −1.20, P = 0.23), postprandial glucose (t = −1.98, P = 0.051) or prandial change in glucose (t = −1.23, P = 0.22). A postprandial plasma glucose <3.9 mmol/L was present in 15 (27%) women and 8 (20%) men (χ2 = 0.41, P = 0.52).
Thirty-six participants took prescribed medications, the commonest of which were: oral contraceptive pill (OCP) n = 17, asthma inhalers n = 8 and antidepressants n = 7, with five participants taking selective serotonin reuptake inhibitors. No participant took medication known to be associated with hypoglycaemia. 3 If OCPs were excluded, there were no gender differences in medication use. Exploratory analyses were undertaken on the relationship between postprandial glucose by gender and the following variables; exact timing of postprandial sample collection in relation to the completion of breakfast, carbohydrate intake and also pre- and postprandial glucose difference. A weak negative relationship between postprandial glucose and carbohydrate intake was observed in men (R2 = 0.15, P = 0.01), but no other relationship was found.
Conclusion
Our results suggest that a one-hour postprandial venous plasma glucose value as low as 3.3 mmol/L in healthy young adults may be normal, given that 95% of study participants had postprandial glucose values at or above this concentration. This value is lower than the commonly accepted value for the lower limit of non-fasting venous plasma glucose of 3.9 mmol/L.
1
The postprandial drop in mean venous plasma glucose (see Figure 1) was unexpected, however at least three other studies showed a similar phenomenon.4–6 Study participants chose their breakfast size and composition, thus the measured glucose reflected a ‘real-world’ setting
Comparison of fasting and postprandial venous plasma glucose for male (a, n = 41) and female (b, n = 55) participants. The commonly reported lower limit for venous plasma glucose (solid horizontal line, y = 3.9 mmol/L) and the 5th percentile for postprandial venous plasma glucose in the current study (dotted line, y = 3.3 mmol/L) are shown to highlight the region of uncertainty when reporting on laboratory measured non-fasting venous plasma glucose. Four female participants and zero male participants had postprandial glucose values <3.3 mmol/L.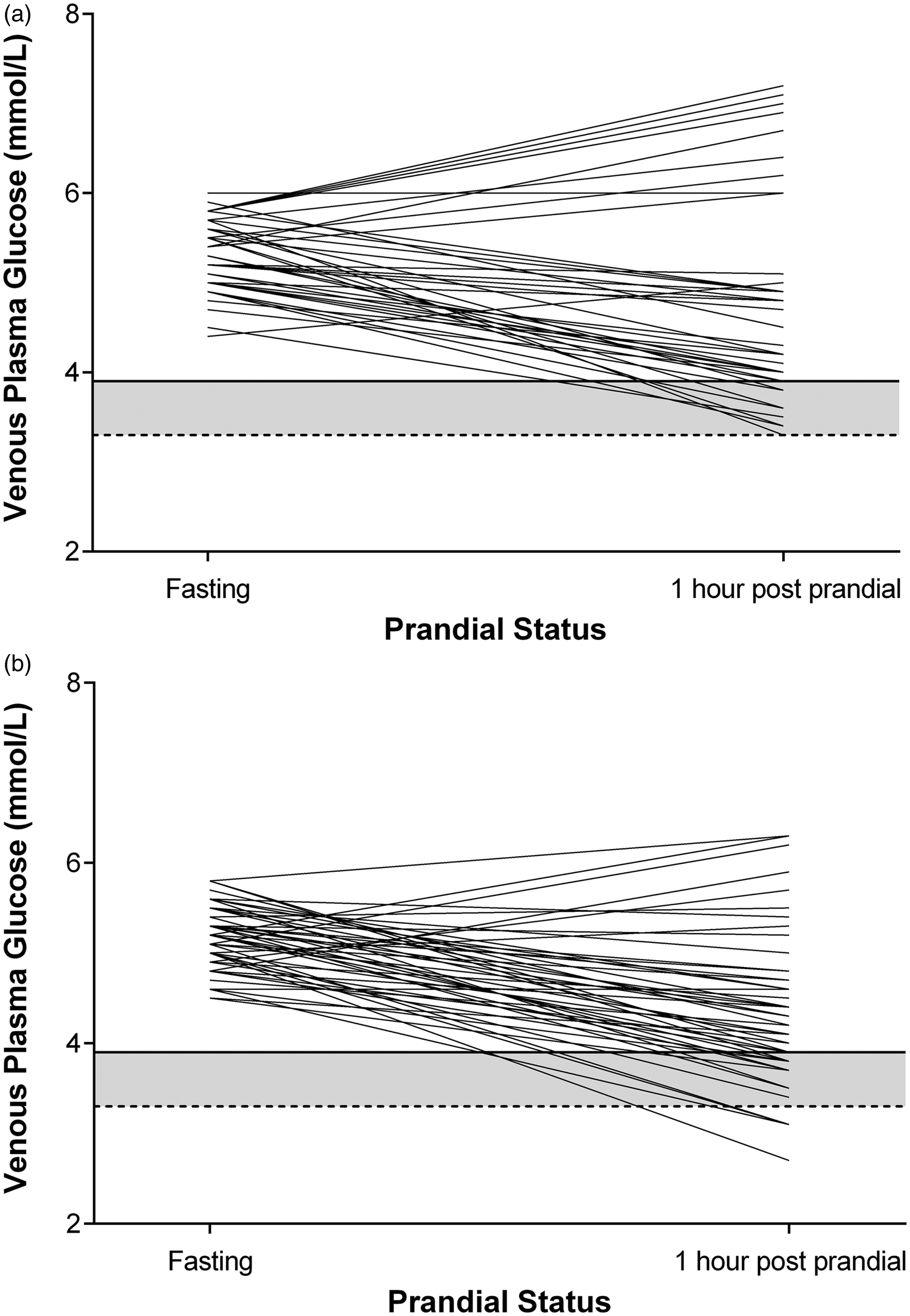
The results presented in this article were collected as part of an earlier study, 1 which was not designed to address the possible mechanisms for the observed postprandial drop in venous plasma glucose. It is however worth noting that the earlier study showed the expected postprandial rise in finger stick capillary glucose, of 0.63 mmol/L at one hour. These combined findings (postprandial rise in capillary glucose, fall in venous glucose) suggest that the venous plasma glucose fall was due to tissue uptake of glucose as blood circulates from the capillary to venous system. Future studies aimed at defining the physiological mechanism(s) for the fall in venous glucose should therefore include the measurement of insulin, 7 and other hormones known to modulate tissue glucose uptake. Breakfast carbohydrate intake was measured but no additional nutritional data were collected, thus no information is available about other macronutrients or glycaemic index. Additional nutritional information might have offered an explanation for the observed weak negative relationship between postprandial glucose and carbohydrate intake in men. This relationship was however detected on post hoc analysis and may thus represent a chance statistical finding.
The study measured venous plasma glucose at a single time point, one hour after breakfast, as this timing was considered to be the most relevant for the earlier study of capillary–venous glucose difference. 2 Although the exact timing of the postprandial venous plasma glucose nadir is unknown, other studies would suggest that it is around 90 min with the maximal capillary–venous glucose difference occurring at one hour.4,5,8 Alternative methods of glucose measurement such as continuous glucose monitoring of interstitial glucose (CGM) are unfortunately unlikely to define the exact timing of the nadir, due to the complex relationship between glucose concentrations within the capillary, venous and interstitial compartments. 9 In addition, although CGM results are thought to reflect venous glucose concentration, especially under stable conditions, 9 CGM calibration is usually undertaken using a capillary sample measured with a glucose meter, thus introducing an element of incorporation bias into the CGM results.
The current study has several additional limitations. Older individuals and children were excluded, thus limiting wider applicability of the findings. The overnight fast was unsupervised, thus fasting status is self-reported. Undertaking a study that specifically addresses these and related limitations would however be logistically challenging.
In summary, this study adds to the available evidence base for interpretation of low glucose values. If a laboratory chooses to define a reference interval for a random glucose in asymptomatic healthy individuals, then a lower limit for postprandial venous plasma glucose of around 3.3 mmol/L may be appropriate.
Footnotes
Acknowledgements
We would like to thank Florence Logan and Dr Winston Chang for their expert technical assistance and Canterbury Health Laboratories for measuring venous plasma glucose.
Declaration of conflicting interests
None relevant to the current study.
Funding
This study was funded by a grant from the New Zealand Society for the Study of Diabetes. AS was supported by a University of Otago summer student grant sponsored by The Diabetes Training and Research Trust.
Ethical approval
The Upper South B Regional Ethics Committee of New Zealand approved this study (URB/10/10/039).
Guarantor
HL.
Contributorship
AS collected data, contributed to the discussion and wrote the manuscript. CMAF reviewed the statistical protocol, contributed to the discussion and reviewed/edited the manuscript. HL and CMF designed the study protocol, contributed to the discussion and reviewed/edited the manuscript.