
Abstract
Background
Inflammation is involved in the mechanism of obstructive sleep apnoea syndrome (OSAS). Omentin, a newly discovered adipokine, is implicated to play an anti-inflammatory role. This study aims to determine whether serum levels of omentin-1 are associated with the presence and severity of OSAS.
Methods
This study consisted of 192 patients with OSAS and 144 healthy subjects. Serum levels of omentin-1 were measured using enzyme-linked immunosorbent assay.
Results
Serum omentin-1 levels were significantly decreased in OSAS patients compared with healthy controls. Multivariable logistic regression analysis revealed that serum omentin-1 levels were inversely associated with the presence of OSAS (odds ratio 0.520, 95% confidence interval 0.433 to 0.623; P < 0.001). Severe OSAS patients had significantly lower serum omentin-1 levels compared with mild and moderate OSAS patients. Spearman correlation analysis showed that serum omentin-1 levels were correlated with the severity of OSAS. Simple linear regression analysis showed that the serum levels of omentin-1 were negatively correlated with waist circumference, body mass index, systolic blood pressure, homeostasis model assessment of insulin resistance (HOMA-IR), C-reactive protein (CRP), and apnoea-hypopnoea index in patients with OSAS. Furthermore, only HOMA-IR and CRP remained inversely associated with serum omentin-1 after multiple stepwise regression analysis.
Conclusion
Decreased serum omentin-1 levels could be considered as an independent predictive marker of the presence and severity of OSAS.
Introduction
Obstructive sleep apnoea syndrome (OSAS) is a common disorder, with an estimated prevalence of 4% for middle-aged men and 2% for middle-aged women in the general population. 1 It is characterized by repetitive collapse of upper airway during sleep, resulting in impedance to airflow, oxygen desaturation and arousals from sleep. 2 OSAS could lead to considerable morbidity and mortality. A growing body of evidence indicates that OSAS may be an independent risk factor for insulin resistance, metabolic syndrome, type 2 diabetes and cardiovascular diseases, independently of obesity. 3 The exact mechanism of OSAS is not clear. Inflammation is considered to play an important role in the development of OSAS. Recent studies have shown a wide variety of pro-inflammatory mediators are elevated in the circulation of patients with OSAS. 4
Omentin, a novel adipokine, is produced and secreted mainly by visceral adipose tissue. Omentin, a recently identified fat deposition-specific adipokine coded by two genes (1 and 2), is mainly expressed in visceral omental adipose tissue. Omentin-1 has been shown to be the major circulating isoform in human serum. 5 Serum omentin-1 level was shown to be significantly decreased in patients with obesity, 6 polycystic ovary syndrome, 7 diabetes 8 and coronary artery disease. 9 Recent evidence indicates that omentin may serve as an anti-inflammatory mediator. Omentin has been shown to play an anti-inflammatory role by preventing the tumour necrosis factor alpha (TNF-α)-induced COX-2 expression in vascular endothelial cells. 10 Inflammation is associated with the mechanism of OSAS. Therefore, omentin is hypothesized to be involved in the pathophysiology of OSAS.
Although there have been studies on the association of adipokines such as adiponectin, 11 leptin, 12 visfatin 13 and resistin 4 with OSAS, no investigation on the association between omentin-1 and OSAS has been performed yet. The present study aims to determine the serum levels of omentin-1 in patients with OSAS to assess its role in pathophysiology of OSAS.
Materials and methods
Patients
This study consisted of 192 newly diagnosed male patients with OSAS. All patients with OSAS were diagnosed with polysomnography (PSG). None had undergone any treatment for OSAS. Patients who had personal or family history of psychiatric disorders, history of alcohol and drug abuse, and any other significant medical illnesses such as diabetes mellitus, cancer, cardiovascular, cerebrovascular, pulmonary or neuromuscular disease were excluded from this study. Control participants were recruited from male healthy subjects with medical check-up in the medical checking centre of our hospital and matched to the cases by age, waist circumference (WC) and body mass index (BMI). Subjects with any symptoms of OSAS, history of alcohol and drug abuse, diabetes mellitus, any other respiratory disorder, any malignancy, chronic kidney or liver disease, endocrine disorders or psychiatric disorders were excluded from the control group.
This study was approved by The Ethics Committee of Shengjing Hospital of China Medical University (2010SJH0026), and informed consent was obtained from all participants.
Sleep study
Full PSG monitoring was performed in all participants using the Compumedics E-series Sleep System (Compumedics Sleep: Melbourne, Australia). Polysomnographic monitoring consisted of monitoring of sleep by electroencephalography, electrooculography, electromyography, airflow and respiratory muscle effort, and included measures of electrocardiographic rhythm and blood oxygen saturation. Apneas were defined as a complete lack of air flow for at least 10 s. Hypopnoea was defined as a reduction in airflow with a 50% from baseline for at least 10 s, a 3% drop in oxygen saturation from the preceding stable saturation, and/or arousal. Apnoea-hypopnoea index (AHI) was defined as the frequency of apnoea and hypopnoea per one hour. Subjects with AHI <5 were included in the control group. Subjects with AHI ≥5 were considered to have OSAS. The OSAS patients were then divided into three groups: a mild group with an AHI of ≥5 to <15 (n = 16), a moderate group with an AHI ≥15 to <30 (n = 123) and a severe group with an AHI ≥30 (n = 53).
Measurements
At first examinations, WC and blood pressure were measured. Venous blood was collected after a minimum of 10 h of fasting. Fasting plasma glucose (FPG), serum triglycerides (TG), serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) and C-reactive protein (CRP) were tested using an auto biochemistry instrument (Hitachi 7170, Tokyo, Japan). Serum fasting insulin level was tested by radioimmunoassay. Subjects with FPG ≥6.1 to <7.0 mmol/L were diagnosed with impaired fasting glucose (IFG). In addition, subjects with FPG <6.1 mmol/L were diagnosed with normal glucose tolerance (NGT). Serum omentin-1 levels were measured using an enzyme-linked immunosorbent assay (BlueGene Biotech Co., Shanghai, China). BMI was calculated as weight in kilograms divided by height squared in meters (kg/m2). Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as insulin reading (μIU/mL) multiplied by plasma glucose level (mmol/L) and divided by 22.5.
Statistical analysis
Data are presented as means ± SD or median (interquartile range). Data normality was analysed using the Kolmogorov–Smirnov test. Comparison of the characteristics between patients with OSAS and healthy controls were performed by unpaired t-test or Mann–Whitney U test. Univariate analysis was performed and the variables with a P < 0.10 were then entered into a backward stepwise multivariate logistic regression model to calculate the odds ratio values (ORs) and 95% confidence intervals (CIs) for the presence of OSAS. Kruskal–Wallis test was used to compare the differences of serum omentin-1 levels among mild, moderate and severe OSAS patients. And Nemenyi test was used to compare the differences between each two groups. The correlation of serum omentin-1 levels with the severity of OSAS was determined using Spearman correlation analysis. Mann–Whitney U test was utilized to analyse the differences of serum omentin-1 levels between NGT and IFG subjects. The correlation between serum omentin-1 and other parameters were analysed using simple linear regression analysis. Then a multiple stepwise linear regression analysis was used to determine the contribution of various factors to serum omentin-1. As serum omentin-1 and CRP levels were not normally distributed, logarithmic (log) transformed values were used for multiple linear regression analysis. Statistical analysis was carried out using SPSS version 13.0 software program (SPSS Inc, Chicago, IL, USA). Statistical significance was accepted at a level of P value less than 0.05.
Results
Baseline clinical characteristics
Clinical and biochemical characteristics of OSAS patients and healthy controls
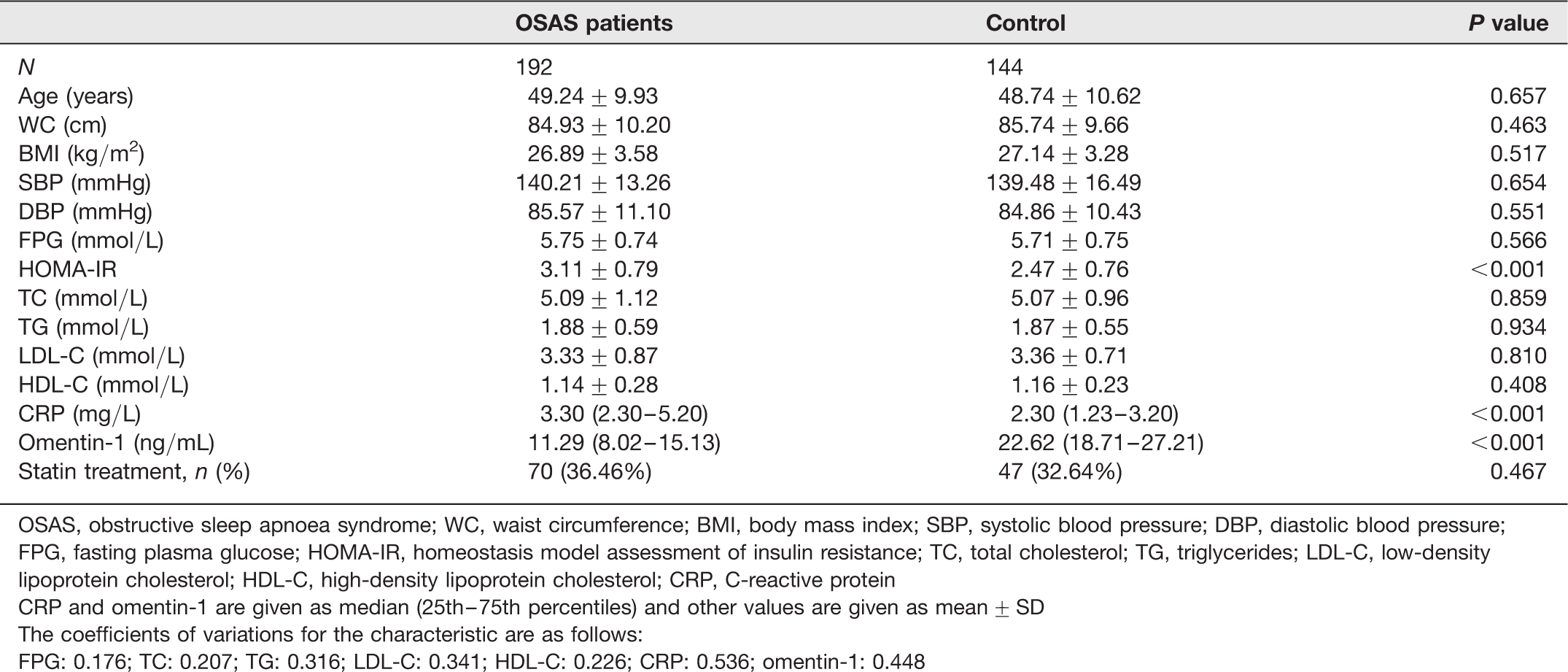
OSAS, obstructive sleep apnoea syndrome; WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HOMA-IR, homeostasis model assessment of insulin resistance; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; CRP, C-reactive protein
CRP and omentin-1 are given as median (25th–75th percentiles) and other values are given as mean ± SD
The coefficients of variations for the characteristic are as follows:
FPG: 0.176; TC: 0.207; TG: 0.316; LDL-C: 0.341; HDL-C: 0.226; CRP: 0.536; omentin-1: 0.448
Sleep characteristics of OSAS patients and healthy controls
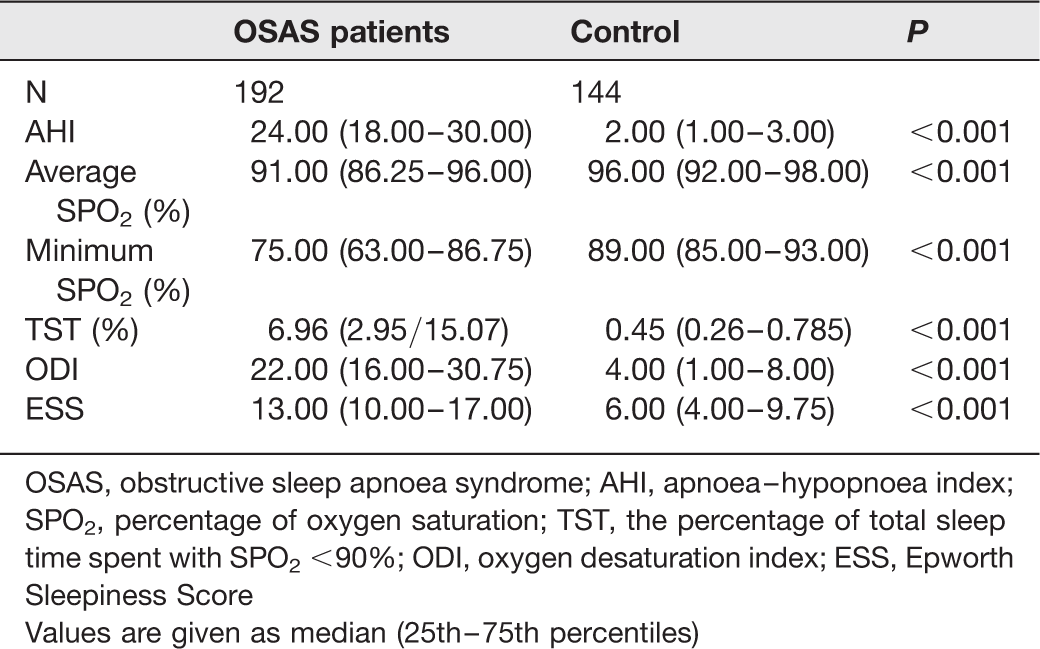
OSAS, obstructive sleep apnoea syndrome; AHI, apnoea–hypopnoea index; SPO2, percentage of oxygen saturation; TST, the percentage of total sleep time spent with SPO2 <90%; ODI, oxygen desaturation index; ESS, Epworth Sleepiness Score
Values are given as median (25th–75th percentiles)
Serum omentin-1 level in OSAS patients
Logistic regression analysis for the presence of OSAS
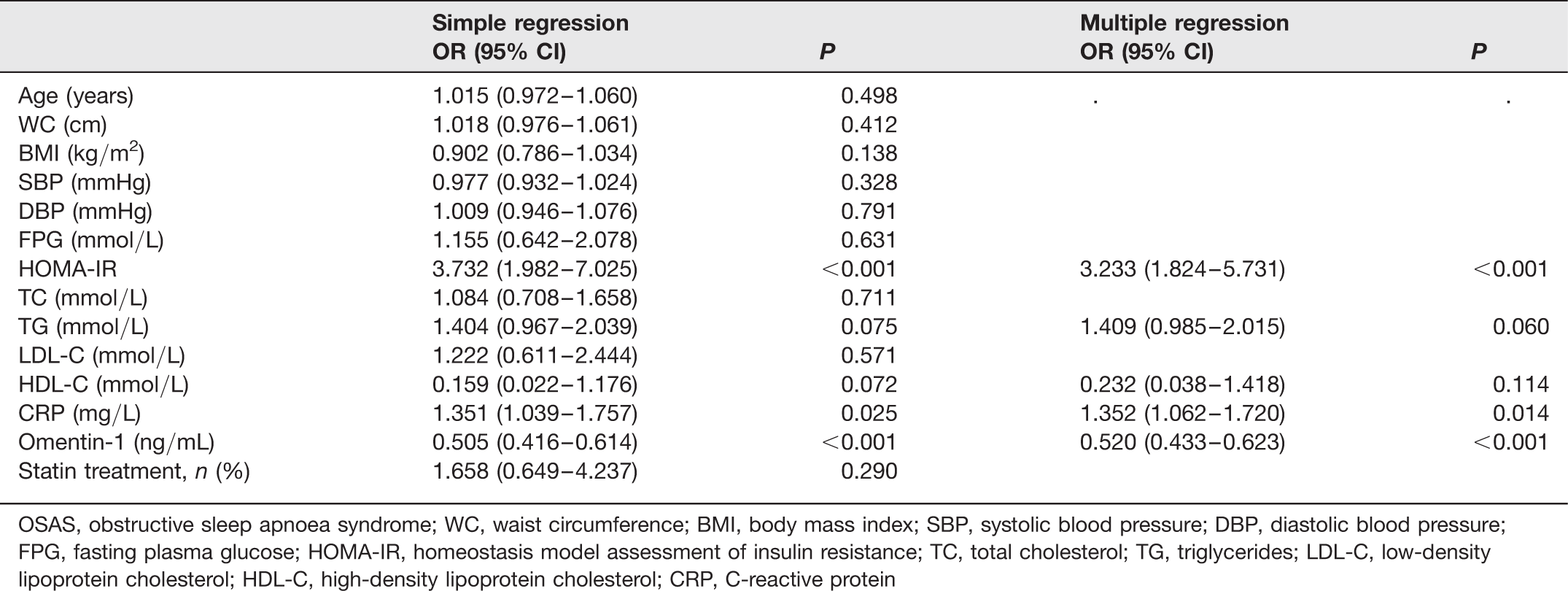
OSAS, obstructive sleep apnoea syndrome; WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HOMA-IR, homeostasis model assessment of insulin resistance; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; CRP, C-reactive protein
Association of omentin-1 levels with OSAS severity
Association of omentin-1 levels with OSAS severity

OSAS, obstructive sleep apnoea syndrome
Values are given as median (25th–75th percentiles)
P1: P value between mild OSAS patients and moderate OSAS patients
P2: P value between mild OSAS patients and severe OSAS patients
P3: P value between moderate OSAS patients and severe OSAS patients
Omentin-1 levels in NGT and IFG patients with OSAS
Omentin-1 levels in NGT and IFG subjects with OSAS
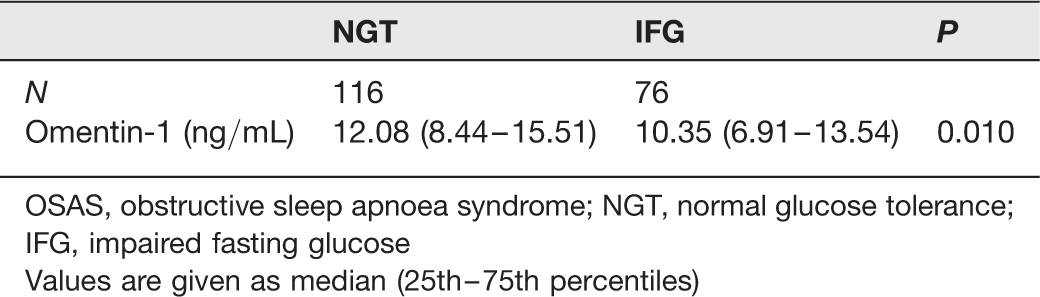
OSAS, obstructive sleep apnoea syndrome; NGT, normal glucose tolerance; IFG, impaired fasting glucose
Values are given as median (25th–75th percentiles)
The association of serum omentin-1 level with other clinical characteristics
Linear regression analyses between omentin-1 and other clinical parameters
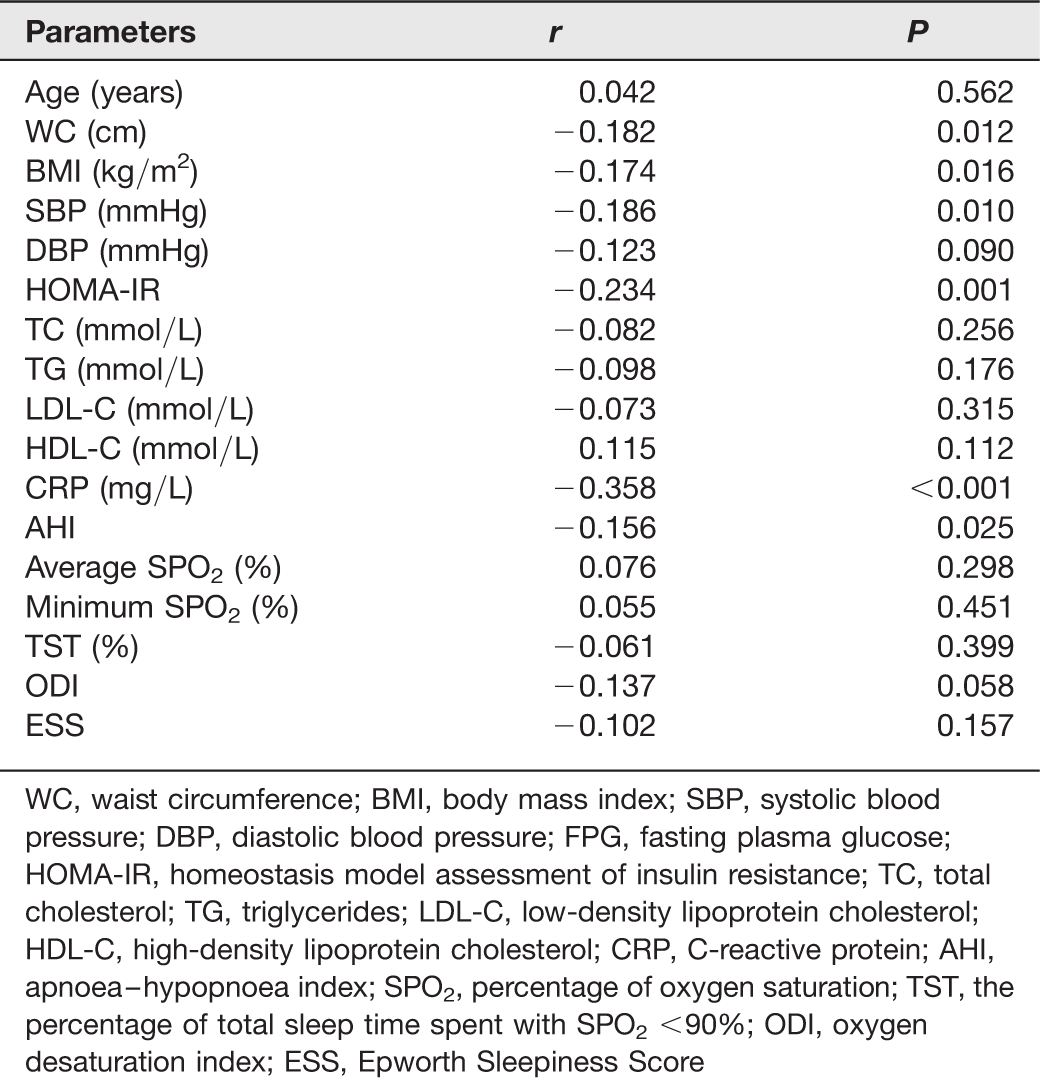
WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HOMA-IR, homeostasis model assessment of insulin resistance; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; CRP, C-reactive protein; AHI, apnoea–hypopnoea index; SPO2, percentage of oxygen saturation; TST, the percentage of total sleep time spent with SPO2 <90%; ODI, oxygen desaturation index; ESS, Epworth Sleepiness Score
Discussion
The current study indicated that serum omentin-1 levels were significantly decreased in OSAS patients compared with healthy subjects. Multivariable logistic regression analysis revealed that serum omentin-1 levels were an independent determinant of the presence of OSAS. Severe OSAS patients had significantly decreased levels of serum omentin-1 compared with mild and moderate OSAS patients. In addition, serum levels of omentin-1 were negatively correlated with WC, BMI, SBP, HOMA-IR, CRP and AHI in patients with OSAS. To the best of our knowledge, there is no previous study evaluating omentin-1 levels in OSAS patients.
Although the main symptom of OSAS is daytime hypersomnolence, OSAS is often complicated with type 2 diabetes mellitus, hypertension and other diseases involving metabolic syndrome. 14 Therefore, it is important to assess the risk of OSAS at an early stage and then to target strategies to prevent or treat OSAS. Our results revealed that serum levels of omentin-1 were significantly decreased in patients with OSAS compared with healthy controls. This indicates that omentin-1 may be involved in the pathophysiology of OSAS. Our results also suggested that omentin-1 levels were negatively correlated with AHI. Severe OSAS patients showed significantly reduced levels of serum omentin-1 compared with mild and moderate OSAS patients. This indicates that decreased omentin-1 levels are associated with the severity of OSAS. Therefore, decreased levels of serum omentin-1 could serve as a new biomarker to predict the presence and severity of OSAS.
Inflammation has been indicated as a potential mechanism for OSAS. Elevated levels of various circulating inflammatory markers, such as tumour necrosis factor alpha (TNF-α), interleukin-6 (IL-6), and CRP have been suggested to be associated with OSAS. 15 Omentin-1, one newly discovered adipokine, is shown to act as an anti-inflammatory mediator. Omentin could inhibit TNF-induced vascular inflammation in human endothelial cells. 10 Omentin was also reported to inhibit TNF-α-induced vascular cell adhesion molecule-1 expression via preventing the activation of p38 and c-Jun N-terminal kinase at least in part through inhibition of superoxide production. 16 These results indicate that omentin may play an important anti-inflammatory role. Furthermore, serum omentin-1 was negatively correlated with TNF-α and IL-6 in patients with type 2 diabetes and polycystic ovary syndrome.7,17 In both NGT and impaired glucose tolerance subjects, circulating omentin concentration was correlated with CRP and IL-6. 18 Similar results were found in our study, which revealed that serum omentin-1 levels were negatively correlated with CRP. Hence, decreased levels of serum omentin-1 may reflect decreased anti-inflammatory activity and then elevated levels of inflammatory molecules, at last the presence and progression of OSAS.
The current results indicate that serum levels of omentin-1 were negatively correlated with WC, BMI, SBP, and HOMA-IR. This is consistent with other studies. Serum levels of omentin were found to be associated with WC, BMI, SBP and HOMA-IR in patients with obesity, 19 metabolic syndrome (MetS), 20 type 2 diabetes 17 and coronary artery disease. 21 Obesity, insulin resistance and hypertension are multiple compounding factors of MetS. This indicates that omentin-1 may be involved in the mechanism of obesity and MetS. Recent studies have reported decreased concentrations of serum omentin-1 in patients with obesity 18 and MetS. 20 Obesity and MetS are closely associated with OSAS. Obesity and particularly central adiposity are potent risk factors for OSAS. In addition, current data suggest that there is an increased prevalence of MetS in subjects with OSAS. This indicates that omentin may be involved in the crosstalk of obesity, MetS and OSAS.
Potential limitations of this study merit consideration. First, the numbers of subjects in the case and control groups were somehow small. Second, this study was cross-sectional, so our findings should be validated in long-term prospective studies.
In conclusion, this study showed that serum omentin-1 levels were decreased in OSAS patients compared with healthy controls. Severe OSAS patients showed significantly decreased levels of serum omentin-1 compared with mild and moderate OSAS patients. Decreased serum omentin-1 levels are suggested to be an independent predictive marker of the presence and severity of OSAS.