
Abstract
Parathyroid gland (PG) auto-transplantation is performed to preserve the function of de-vascularized or unintentionally removed PGs, however, little has been published about the technique and outcomes in children. In our study, we aimed to present the results of PG auto-transplantation in children undergoing thyroidectomy or parathyroidectomy at a tertiary single institution. A retrospective review identified 14 patients (<18 years of age) who underwent PG auto-transplantation from January 2000 to December 2022. 57.1% (8/14) had transient postoperative hypocalcemia and 14.3% (2/14) had permanent postoperative hypocalcemia. Eight patients had transient hypoparathyroidism, correlating with the rate of transient hypocalcemia. The most common reimplantation site was the sternocleidomastoid (11/14) and it was significantly associated with normalized calcium levels 6 months after auto-transplantation (p=0.033). Bilateral central neck dissection and surgical indication of cancer had a statistically significant association with transient hypocalcemia (p=0.03 and p=0.005, respectively). Our study provides valuable insights into the outcomes of PG auto-transplantation in pediatric patients, highlighting the potential for successful engraftment and factors associated with hypocalcemia.
Keywords
Introduction:
Postoperative hypocalcemia is the most common complication of thyroidectomy in children and adults. 1 This complication can occur due to accidental injury, excision, or devascularization of the parathyroid glands (PGs). The management of transient postoperative hypocalcemia requires treatment and monitoring, which can prolong hospitalization and escalate care costs. 1 Furthermore, permanent hypocalcemia requires lifelong treatment with calcium and/or vitamin D supplementation.
Thyroidectomy in children is considered a safe procedure with a mortality rate below 0.1% and a 30-year survival rate of over 95% for differentiated thyroid cancer.2,3 However, the incidence of hypocalcemia post-thyroidectomy is higher among children when compared to adults.4,5 Recognizing the substantial disease burden associated with permanent hypoparathyroidism, the use of PG auto-transplantation is an option restore parathyroid function and reduce incidence of postoperative hypocalcemia in children. However, there is a paucity of literature addressing the outcomes of PG auto-transplantation in children.6 -9 In our study, we present the outcomes of PG auto-transplantation in children undergoing thyroidectomy or parathyroidectomy at a large, single institution.
Methods
Pediatric patients (≤18 years of age) who underwent parathyroid gland (PG) auto-transplantation following total thyroidectomy or parathyroidectomy at Monroe Carell Junior Children’s Hospital at Vanderbilt University Medical Center (VUMC) between January 2000 and December 2022 were included in this retrospective study. Patients were identified through a comprehensive search of operative records and electronic medical records. The study was approved by the VUMC Institutional Review Board.
Demographic, surgical, and clinical data were extracted from electronic medical records, including operative and pathology reports. Race and ethnicity were collected from clinic intake forms. Statistical analysis was performed using R version 4.1.2 (R Core Team, Vienna, Austria). Categorical data were compared using Fisher’s exact test, with statistical significance defined as P < 0.05.
Criteria for Auto- transplantation
PG auto-transplantation was performed in cases where parathyroid viability was concerning during thyroidectomy or parathyroidectomy.
The standard technique used involved the PG being minced into 1mm slices to increase surface area, improving the likelihood of uptake by surrounding vasculature. Small pieces of glandular tissue were then inserted into individual muscle pockets such as the sternocleidomastoid muscle (SCM) to optimize vascular integration and transplant viability.
Definitions Used
Hypocalcemia
At least one total serum calcium level < 8.4 mg/dL (<2.1 mmol/L) or ionized calcium <4.5 mg/dL (<1.05 mmol/L), with or without clinical signs of hypocalcemia.
Transient hypocalcemia
Hypocalcemia within 48 hours postoperatively or prior to discharge that resolves and normalizes by 6 months.
Permanent hypocalcemia
Hypocalcemia persisting at 6 months postoperatively.
Transient hypoparathyroidism
Serum PTH <16 pg/ml within 48 hours postoperatively or prior to discharge that resolves and normalizes by 6 months.
Results
A total of 14 pediatric patients underwent PG auto-transplantation at VUMC (Table 1). Thirteen patients underwent thyroidectomy, and one underwent parathyroidectomy. The most common transplantation site was the sternocleidomastoid (SCM) muscle (n=11, 78.6%). Thyroid cancer was the surgical indication for 50% of cases (n=7), predominantly papillary thyroid cancer (n=6) and medullary thyroid cancer (n=1). All thyroid cancer patients underwent concurrent central neck dissections (CND), with 71.4% undergoing bilateral CND and 28.6% unilateral CND.
Patient Demographic and Surgical Characteristics.

Abbreviations: no., number; SD, standard deviation.
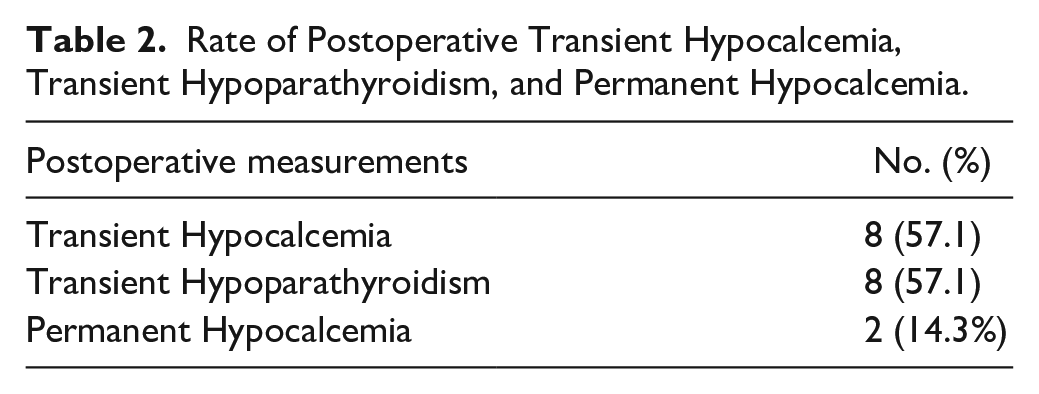
Transient postoperative hypocalcemia occurred in 57.1% of patients (8/14), while permanent hypocalcemia was observed in 14.3% (2/14). Serum PTH levels were measured within 48 hours for all patients (n=14), and transient hypoparathyroidism was identified in 8 patients, aligning with the rate of transient hypocalcemia (57.1%, Table 2). Surgical characteristics associated with transient and permanent hypocalcemia are detailed in Table 3. Patients who underwent bilateral CND were significantly more likely to experience transient hypocalcemia compared to those who did not (62.5% vs. 37.5%, 95% CI [26-90], p=0.03). Additionally, thyroid cancer as a surgical indication was significantly associated with transient hypocalcemia (87.5% vs. 12.5%, 95% CI [47-99], p=0.005).
Rate of Postoperative Transient Hypocalcemia, Transient Hypoparathyroidism, and Permanent Hypocalcemia.
Surgical Characteristics for Patients With Transient Hypocalcemia and Permanent Hypocalcemia after PG Auto-Transplantation.
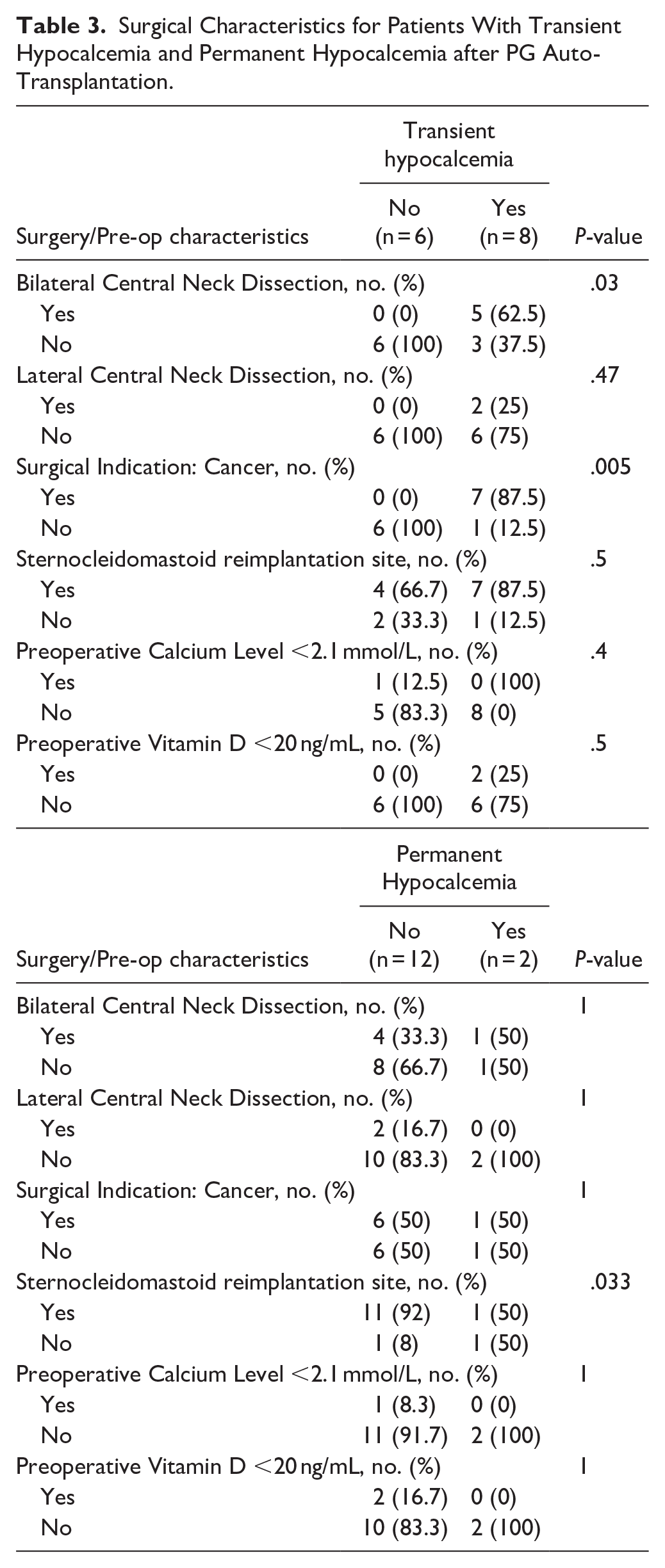
Auto-transplantation of PG into the SCM muscle (87.5%) was significantly associated with normal calcium levels at 6 months postoperatively compared to other reimplantation sites (95% CI [60-100], p=0.033).
Discussion
Assessing the role and success of PG re-implantation is difficult when PGs are identified intra-operatively and preserved, but there is very little literature discussing experience and outcomes in the pediatric population in our study, 85.7% of pediatric patients achieved normalized calcium levels within 6 months after PG auto-transplantation, indicating a high rate of successful engraftment. The rates of transient and permanent postoperative hypocalcemia in our study were 57.1% and 14.3%, respectively. Measurement of serum PTH levels within 24 hours for all patients revealed that eight experienced transient hypoparathyroidism, aligning with the observed rate of transient hypocalcemia.
Notably, PG re-implantation into the sternocleidomastoid (SCM) was a strong predictor of preventing permanent hypocalcemia. Furthermore, bilateral central neck dissection (CND) and thyroid cancer as surgical indications were significantly associated with transient hypocalcemia, consistent with prior studies.10,11
In our study, two patients experienced permanent hypocalcemia following PG auto-transplantation. One of these patients had the only instance of re-implantation into the strap muscle. The other patient had medullary thyroid carcinoma with extensive metastasis and direct tracheal involvement, requiring a complex surgical procedure involving the sacrifice of major structures such as one jugular vein, both recurrent laryngeal nerves, and part of the trachea, necessitating a tracheostomy. These operative characteristics are potential confounders that could explain the rates of postoperative permanent hypocalcemia found in our cohort.
However, it's important to acknowledge the limitations of our study. The primary limitation is its retrospective design with a limited sample size. Future studies would benefit from a multi-institutional cohort with standardized surgical techniques to improve generalizability Additionally, there is significant variability in the criteria used to define postoperative hypocalcemia across studies.12 -14 Although we reported rates of both hypocalcemia and hypoparathyroidism in the transient setting, we lacked data to track parathyroid hormone (PTH) levels 6 months postoperatively, which limits our ability to fully assess long-term parathyroid function. Standardized definitions would improve the quality of research in this field, which remains a limitation when studying PG auto-transplantation in both adults and children.
Lastly, we recognize the difficulty in distinguishing between the success of parathyroid re-implantation and the preservation of native parathyroid gland function. The degree of potential confounding is high, as it is possible that some cases of transient hypocalcemia may result from devascularization or compromised blood supply to the parathyroid glands during dissection, with subsequent return of function, rather than from successful engraftment of the transplanted tissue. This nuance should be considered when interpreting our findings, and further research is needed to clarify these distinctions. Furthermore, additional studies are warranted to compare the incidence of permanent hypocalcemia in patients who did not undergo auto-transplantation versus those who did. Such analyses could provide valuable insights into whether patients who developed hypoparathyroidism might have benefited from auto-transplantation, and if surgeons should have a higher threshold for considering PG reimplantation.
Our study provides valuable insights into the outcomes of PG auto-transplantation in pediatric patients, highlighting the potential for successful engraftment and factors associated with hypocalcemia. These findings can guide surgeons in selecting optimal re-implantation sites and identifying patients at higher risk for postoperative hypocalcemia, ultimately improving patient care and surgical decision-making in this population.
Footnotes
Acknowledgements
None.
Consent for Publication
Not applicable.
Data Avaliability Statement
The raw data is not available to access because the IRB does not allow it
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval Statement
The study was approved by the VUMC Institutional Review Board.