
Abstract
Background:
Branchial cleft cysts are pediatric congenital anomalies that can present as sinus tracts to the neck. Intraoperative methylene blue dye with fibrin glue has been suggested as an effective tool for tracking the tract’s depth to help definitively excise. In this large retrospective study of 118 patients spanning a decade, we aim to elucidate outcomes of branchial cleft anomaly excision without methylene blue dye.
Methods:
A retrospective review was conducted with patients who received branchial cleft anomaly (BCA) with sinus tract excision at Monroe Carrell Jr. Children’s Hospital from June 2012 to June 2022. We collected demographic variables, BCA characteristics, perioperative care variables (ie, prior drainage, imaging, and concurrent procedure), and perioperative outcomes (ie, intra- and post-operative complications). Median and interquartile range (IQR) were calculated for continuous demographic variables, and average and standard deviation (SD) were calculated for sinus tract length. Two-tailed Chi-square or Fisher’s exact tests were performed to compare categorical samples where applicable with a statistical significance threshold set a priori at P < .05, and multivariable logistic regression assessed significant associations.
Results:
The sample included 118 patients with an average tract length of 3.3 cm (SD = 1.7 cm). Incision/drainage was performed before definitive excision in 16 (13.6%) patients and was associated with age above the median (aOR = 5.29, 95% CI = 1.39-20.09, P = .015) and female sex (aOR = 3.81, 95% CI = 1.12-13.01, P = .032). Most patients (N = 85, 72.0%) did not receive imaging. Among 118 cases, 2 (1.7%) required return to the operating room for surgical site complications. No patients experienced intra-operative complications or tract recurrence necessitating revision surgery.
Conclusion:
Patients with branchial cleft sinus tracts that were surgically excised without intraoperative dye achieved definitive resection with no recurrence and limited post-operative complications. While not a direct comparison, these results suggest that using intraoperative dye may be associated with unnecessary costs without benefit in outcomes.
Keywords
Introduction
Branchial cleft anomalies (BCAs) are exceedingly rare, making up about a quarter of congenital neck masses with no significant differences by sex or ethnicity.1,2 Fistulae or sinus tracts are more commonly diagnosed in infancy while cysts are more often diagnosed as an older child. 3 If not excised completely, branchial cleft cysts can also give rise to sinus tracts to the neck. 4
Techniques have been developed to aid in removing branchial sinus tracts in their entirety such as imaging, 5 endoscopy, 6 and novel incision types.5,7 Even with these techniques, the sinus tract is often hard to follow completely to its endpoint, 5 giving rise to the use of dyes intraoperatively, such as methylene blue dye. 8 Some evidence suggests that intraoperative dye can be an effective tool for tracking tract depth, guiding definitive excision, and thus preventing recurrence.8 -10 While 1 study showed no BCA recurrence among 17 patients receiving intraoperative dye, 9 other work suggests it is an unnecessary step: without intraoperative dye, BCA recurrence rates are below 5%. 11
Literature assessing the use of intraoperative dye during BCA excision has been limited to case reports and samples of under 40 patients. 11 In this large retrospective case series of 118 patients spanning a decade, we aim to elucidate outcomes of branchial cleft anomaly excision without methylene blue dye. Based on conducting the largest study of BCA recurrence after initial excision without the use of intraoperative dye, we hypothesize that the intra-operative complication and recurrence rates are low despite the use of dyes and multiple surgeons involved with these surgeries.
Methods
A retrospective chart review was conducted with patients who received BCA with sinus tract excision performed by over 10 different surgeons at Monroe Carrell Jr. Children’s Hospital from June 2012 to June 2022. We collected demographic variables, BCA characteristics, perioperative care variables (ie, prior drainage, imaging, and concurrent procedure), and perioperative outcomes (ie, intra- and post-operative complications). Median and interquartile range (IQR) were calculated for continuous demographic variables, and average and standard deviation (SD) were calculated for sinus tract length. Two-tailed Chi-square (with continuity correction as indicated) or Fisher’s exact tests were performed to assess the association of sinus tract length with age, race, sex, BMI, prior incision, and imaging; imaging with age, sex, race, insurance, BMI, prior incision/drainage, and concurrent procedure; and prior incision/drainage with age, sex, race, BMI, and insurance. A statistical significance threshold was set a priori at P < .05. Multivariable logistic regression was performed with prior incision/drainage and variables with statistically significant Chi-square or Fisher’s exact tests.
Results
The sample included 118 patients with slight male predominance (51.7%) and median age of 2 years and 8 months (Table 1). BCA location was predominantly left-sided (N = 57, 48.3%) with 9 (7.6%) bilateral cases and 11 (9.3%) midline cases. Of the cases with quantitative values for sinus tract length (N = 40), the average tract length was 3.3 cm (SD = 1.7 cm). Sinus tract length was not associated with age, sex, race, BMI, prior incision/drainage, or imaging (Supplemental Table 1).
Patient Demographics and Branchial Cleft Anomaly Characteristics.
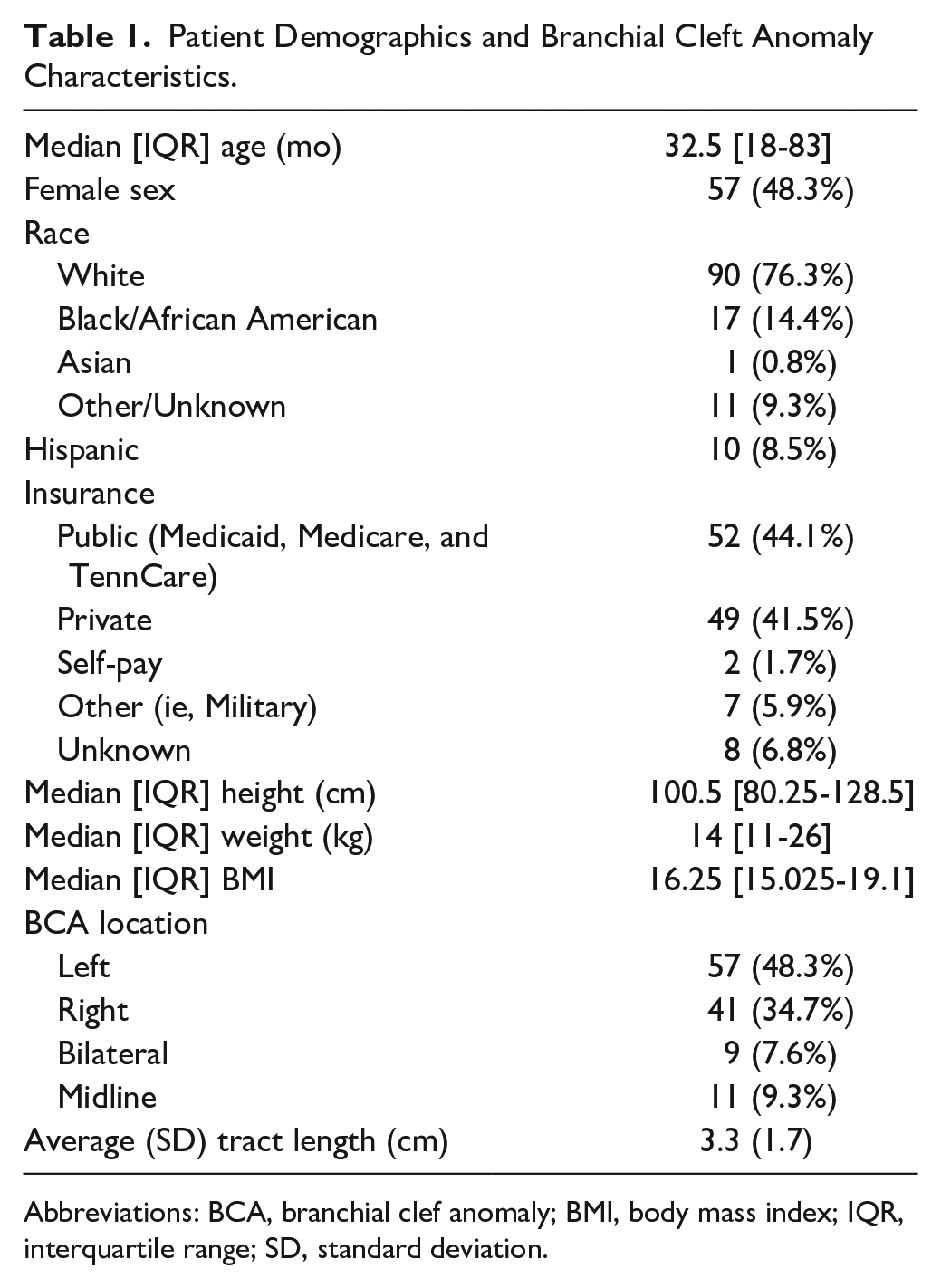
Abbreviations: BCA, branchial clef anomaly; BMI, body mass index; IQR, interquartile range; SD, standard deviation.
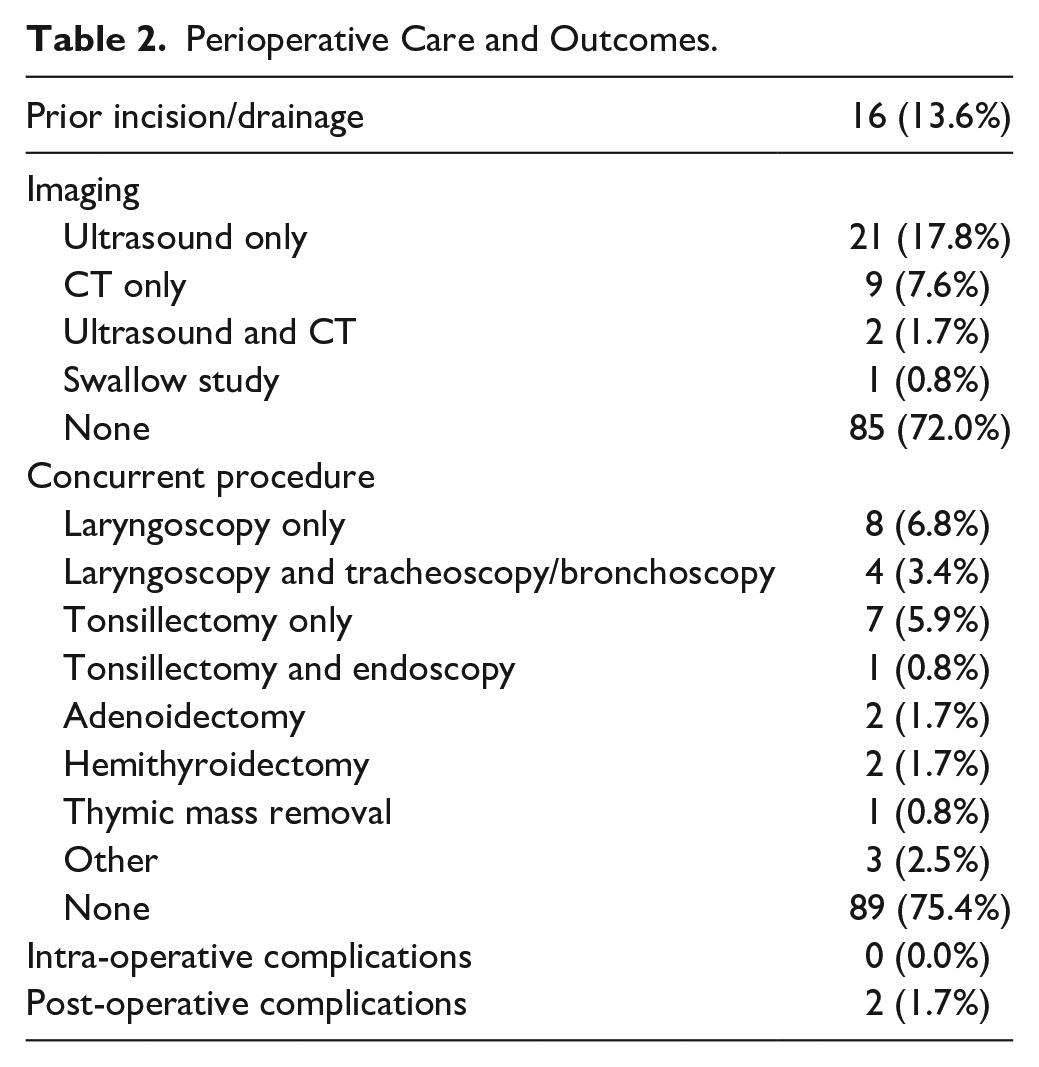
Before the date of definitive excision, incision/drainage was performed in 16 (13.6%) patients (Table 2). Prior incision/drainage was not associated with race, BMI, or insurance (Supplemental Table 2), but it was associated with older age (P = .016) and female sex (P = .042). On multivariable logistic regression (Table 3), prior incision/drainage remained positively associated with age above the median (aOR = 5.29, 95% CI = 1.39-20.09, P = .015) and female sex (aOR = 3.81, 95% CI = 1.12-13.01, P = .032).
Perioperative Care and Outcomes.
Multivariable Regression of Prior Incision/Drainage With Sex and Age.
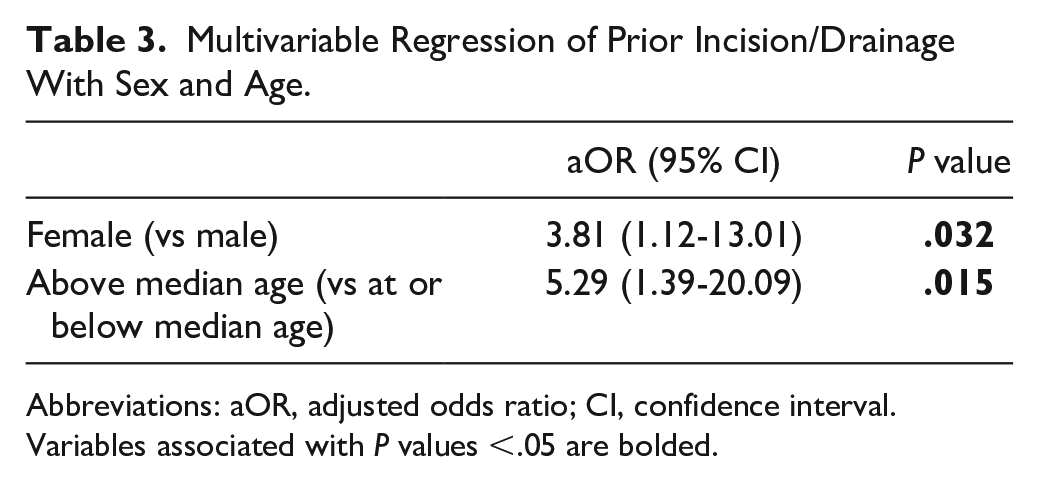
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval.
Variables associated with P values <.05 are bolded.
During BCA excision, concurrent procedures included laryngoscopy only in 8 (6.8%) cases, laryngoscopy and tracheoscopy/bronchoscopy in 4 (3.4%) cases, tonsillectomy only in 7 (5.9%) cases, and tonsillectomy and endoscopy in 1 (0.8%) case. Imaging consisted of ultrasound only in 21 (17.8%) cases, CT scan only in 9 (7.6%) cases, ultrasound and CT scan in 2 cases (1.7%), and swallow study in 1 (0.8%) case. However, most patients (N = 85, 72.0%) did not receive imaging. Imaging was not associated with race, insurance, BMI, prior incision/drainage, or concurrent procedure (Supplemental Table 3), but there was a trend of imaging being associated with older age (P = .065) and female sex (P = .096).
Among 118 cases, 2 (1.7%) required return to the operating room for surgical site complications. One was a neck abscess, and the other was a cervical hematoma. Both cases involved left-sided BCA with no concurrent surgery. No patients experienced intra-operative complications or sinus tract recurrence necessitating revision surgery.
Discussion
Our results show that branchial cleft sinus tracts have a low rate of revision surgery after excision without intraoperative dye, with our study showing 0 out of 118 patients needing revision. Since the surgeries span over a decade with over 10 different surgeons, this finding is not related to a particular surgeon’s technique to limit recurrence. Various imaging techniques such as ultrasound can help guide surgical planning but were not utilized for most cases with no impact on BCA recurrence. These findings suggest that intraoperative dye may not be necessary.
Previous work sheds light on why intraoperative dye may not be necessary. One reason is that certain tracts, especially type II branchial cleft tracts, may not need to be fully excised from end to end. Previous work shows that it is not necessary to excise the tract all the way to the pharyngeal fossa; instead, it is sufficient to stop at the greater cornu of the hyoid. 12 This was the approach for the majority of surgeries performed in our group. Another consideration is that type III branchial cleft anomalies ending in the pyriform sinus of the larynx may necessitate cauterization of the tract endoscopically. However, we did not encounter any of these cases in this series.
Each BCA case is unique. Based on our low recurrence rate without dye, we hypothesize that intraoperative dye may not be broadly necessary to prevent branchial cleft sinus tract recurrence. Future research using a larger, multi-institutional dataset that includes revision cases could test this hypothesis and help delineate when intraoperative dye may offer advantages for specific patient characteristics, anatomical complexities, or procedural contexts.
Conclusion
Patients with branchial cleft sinus tracts that were surgically excised without intraoperative dye achieved definitive resection with no recurrence and limited post-operative complications. While not a direct comparison, these results suggest that using intraoperative dye may entail unnecessary costs without significant benefit in outcomes.
Supplemental Material
sj-docx-1-aor-10.1177_00034894241303021 – Supplemental material for Perioperative Outcomes of Branchial Cleft Sinus Tract Excision in Pediatric Patients Without the Use of Intraoperative Dye
Supplemental material, sj-docx-1-aor-10.1177_00034894241303021 for Perioperative Outcomes of Branchial Cleft Sinus Tract Excision in Pediatric Patients Without the Use of Intraoperative Dye by Daniel R. S. Habib, Naadir H. Jamal, Kalpnaben Patel, Christopher T. Wootten and Ryan H. Belcher in Annals of Otology, Rhinology & Laryngology
Footnotes
Data Availability Statement
The data include patient health information and are thus not available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Vanderbilt Institutional Review Board under IRB211065.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.