
Abstract
Objective:
This systematic review was conducted to assess if there are changes in gastroesophageal reflux (GER) outcomes after frenotomy in infants with ankyloglossia.
Methods:
Systematic Review. CINAHL, Cochrane, EMBASE, Pubmed, and Scopus were searched from inception to May 20, 2023. Inclusion criteria consisted of all study designs, infants ≤12 months of age with ankyloglossia, and use of quantitative GER measures (esophageal pH manometry (pH) or multi-channel intraluminal impedance (MII), and/or patient-reported symptom scores) pre- and post-frenotomy. Quality assessment and data extraction were performed in duplicate.
Results:
Of 37 articles screened, 7 met inclusion criteria (6 prospective cohort studies and 1 RCT). No studies utilized objective measures to quantify reflux, that is MII or pH. The number of infants with ankyloglossia ranged from 47 to 237 (mean age of 4.4-8.3 weeks). Qualitative analysis included all 7 studies which used the GIGER, I-GERQ-R, and GSQ-I scales to assess GER. Parent-reported GER scores decreased post-frenotomy. However, the lack of control groups in the prospective cohort studies precludes conclusive findings that changes are related to frenotomy. Meta-analysis was not possible due to the high risk of bias from limited sample sizes, poor methodology, and lack of adequate control groups.
Conclusion:
Limited work has been conducted on the relationship between frenotomy and GER in infants with ankyloglossia. The lack of high-quality studies precludes definitive conclusions, as GER symptoms are known to improve spontaneously with time. Future RCT studies are warranted to further elucidate the effect of frenotomy on symptoms of GER in infants with ankyloglossia.
Level of Evidence:
III.
Introduction
Gastroesophageal reflux (GER) has been defined as the physiologic process of the passage of gastric contents into the esophagus by North American and European academic societies. 1 The term gastroesophageal reflux disease (GERD) is used to describe GER that produces bothersome symptoms or complications. As infants are unable to verbalize their symptoms, diagnosing reflux can be challenging given the nonspecific and variable nature of presentation. 1 The pathogenesis of GERD is multifactorial, involving transient lower esophageal sphincter relaxations and impaired esophageal acid clearance leading to reflux of acid, pepsin, and bile and esophageal mucosal injury. Severe and prolonged GERD in pediatric patients may have negative, long-term consequences. 2 However, there is a paucity of well-designed studies that identify at-risk infants and characterize the natural history of conditions such as esophageal strictures and Barrett’s esophagus. 3
The reported prevalence of congenital ankyloglossia, or tongue tie, is highly variable, ranging from 0.02% to 10.7% globally. 4 There has been a long-standing concern that restrictive lingual frenulum could interfere with an infant’s ability to breastfeed, speak, and perform mechanical or social skills. 5 However, the benefits and indications of intervention are still unclear according to professional medical associations. For instance, the American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNSF) reached consensus that frenotomy does not always relieve maternal breastfeeding pain and difficulty although frenotomy is more likely to relieve these concerns compared to no treatment. 5
Some professionals have proposed that GER and ankyloglossia may be linked, and some literature is emerging that examines whether symptoms of reflux are improved with frenotomy.6 -9 Some theories linking ankyloglossia and reflux include the concept of aerophagia, the swallowing of air that is believed to be caused by a poor latch in children with ankyloglossia and restrictive maxillary frenula (“upper lip tie”), although the latter entity may have minimal functional significance in breastfeeding or otherwise as research emerges.6 -9 As an area of study currently lacking extensive review and analysis, rigorous evaluation of evidence is imperative prior to encouraging families to subject their children to lingual frenotomy for this indication. The purpose of this systematic review is to evaluate the existing evidence that investigates the use of frenotomy to treat infantile GER.
Methods
Search Strategy
This systematic review was conducted using the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) statements. 10 The databases CINAHL, Cochrane, EMBASE, Pubmed, and Scopus were systematically searched to identify articles that assessed the effect of frenotomy on reflux symptoms in infants born with ankyloglossia up until May 20, 2023. The PICOS (Participants, Intervention, Comparison, Outcome, Study design) criteria were used to form a searchable query from the research question (Table 1). A database specific search strategy was designed (see Supplemental S1) including keywords and Medical Subject Headings (MeSH) terms specific to each database. Only full-text studies published in English were included. There were no limits placed on the publication date or geographic location. Both forward and backward citation tracking of eligible full-text articles was conducted to maximize comprehensiveness. This review was registered on PROSPERO, ID = CRD42023413268, April 11, 2023.
PICOS Criteria for Inclusion of Studies.

Inclusion/Exclusion Criteria
Inclusion criteria for this systematic review included: (1) study design that was a comparative, randomized controlled comparison, or non-randomized comparisons such as cohort studies, case-control studies, cross-sectional studies, prospective follow-up studies, retrospective studies, and multi-center studies; (2) studies that were conducted in vivo in infants under 1 year of age born with ankyloglossia that underwent a frenotomy; (3) the effect of ankyloglossia correction/frenotomy on gastroesophageal reflux must have been investigated quantitatively both before and after surgery; and, (4) the quantitative impact of gastroesophageal reflux before and after frenotomy must have been reported as an outcome.
Exclusion criteria included: (1) single cases studies or reports, systematic reviews, meta-analyses, editorials, not original research, conference abstracts, opinion studies, commentaries, and studies that utilized non-human participants; (2) those with other oral structural abnormalities. No limits were placed on the location of the study or length of follow-up.
Study Selection and Screening
The studies identified through database searches were imported into Covidence Systematic Review Software (Covidence, Veritas Health Innovation, Melbourne, Australia). 11 An automated duplication check conducted by Covidence and a manual duplicate check were performed to detect and remove duplicates. The systematic screening process was performed independently by 2 reviewers (AP and KDC) consisting of a title and abstract screen followed by full-text screening. The title and abstract screen included articles that examined reflux in infants before and after surgical correction of ankyloglossia.
Upon the completion of each level of screening, Cohen’s kappa coefficient was computed, and conflicts were resolved with a consensus meeting. The PRISMA flowchart (Figure 1) outlines the number of studies included and excluded at each stage throughout the selection process.
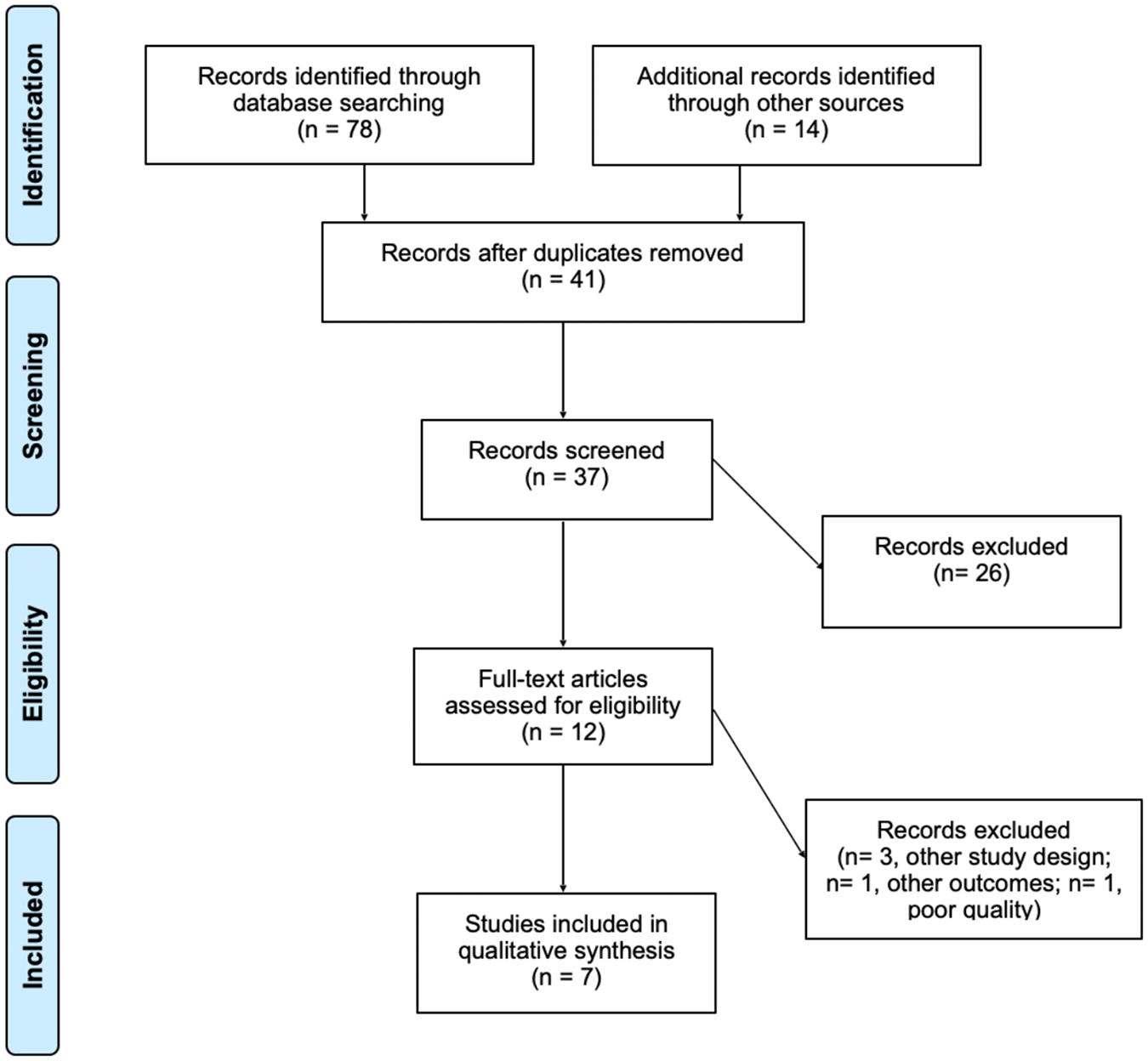
PRISMA flow chart summarizing the results of the literature search.
Quality Assessment
The Newcastle-Ottawa Scale was used by 2 authors (AP and KDC) to perform a methodological quality assessment of included cohort studies, and Cochrane risk of bias tool version 2.0 was used for the randomized controlled trial. The results are reported in Supplemental S2. 12 The scores for each study were compared and any points of contention were reviewed until a unanimous result was obtained. For study evaluation, their methods of selection, comparability, and outcomes/exposure were assessed. A maximum score of 9 can be achieved for cohort studies and the randomized controlled trial was rated as either low, some, or high risk of bias.
Data Extraction
Studies that met inclusion criteria underwent standardized data extraction performed by 2 investigators (AP and KDC) which consisted of: author(s), year of publication, study design, study location, number of enrolled participants, baseline and demographic characteristics of participants including age and sex, pH and MII measurements, and quantitative scores for the revised infant gastroesophageal reflux questionnaire (I-GERQ-R), gastroesophageal symptom questionnaire for infants (GSQ-I), or gastrointestinal and gastroesophageal reflux (GIGER) completed by caregivers of study participants before and after frenotomy. Further data on the percent change in reflux following frenotomy was also reported for studies that utilized the I-GERQ-R.
Main Outcomes
The primary outcome of this study was to assess the effect of frenotomy on reflux in infants with congenital ankyloglossia using (1) objective measures to quantify reflux, namely pH and MII, and (2) currently available parent report measures of GER for infants such as the I-GERQ-R (total score range = 0-42), GIGER (total score range = 0-180), or GSQ-I [(6 symptoms of GER rating number of times per day each symptom occurred and severity ranging from 1 (not at all severe) to 7 (most severe)]; higher scores on self-report tools indicate more severe symptoms/dysfunction.
Results
Search Results
The database search identified 78 articles from Pubmed, CINAHL, Cochrane, SCOPUS, and EMBASE and MEDLINE. An additional 14 were found using manual search on Google Scholar, backward and forward reference searching. After removing duplicates, a total of 37 studies were screened. After the title and abstract screen, 12 articles were identified for full text screening and a total of 7 articles were included in this systematic review.
Study Characteristics
Six articles were prospective cohort studies13 -18 and 1 was a randomized control trial. 19 Table 2 presents all study characteristics. In terms of study location, 4 were in USA, 1 in the Netherlands, and 2 in Italy. Of note, 3 of the studies conducted in the USA were published by the same lead author. All studies were published from 2017 to 2023. Total participant numbers ranged from 47 to 237 infants with mean age of 4.4 to 8.3 weeks, although 1 study did not report mean age. Total number of patients who received a lingual frenotomy ranged from 8 to 237 patients. The percentage of female infants ranged from 37.5% to 55.2%. The included RCT used a crossover design to compare infants undergoing frenotomy (n = 23) to an observational group (n = 24). 19 Crossover data in the observational group was not reported for 17 participants and 7 were lost to follow-up.
Study Characteristics.

29 patients lost to follow up at 6 months.
Diagnosis of Ankyloglossia
The diagnosis and inclusion of patients with ankyloglossia varied across studies (Table 3). The majority of studies used the Coryllos tongue tie classification and the Kotlow lip tie classification except for Hill 2023 and Slagter 2020. Hand 2020 and Hand 2023 included patients with buccal tie although no classification system was reported. Two studies reported performing revision frenotomies after the initial procedure did not relieve symptoms.14,18 Only 1 study exclusively included patients with tongue tie. 19 All studies except Hill 2023 and Slagter 2020 presented reflux data stratified by the types of ties that were corrected.
The Diagnosis and Inclusion of Patients with Ankyloglossia.

Abbreviation: NR, not reported.
Posterior tongue tie was found in 67.5% of participants and described as Class III and IV tongue frenum +/− class IV lip frenum.
Authors reported that 60.5% of the infants had a combination of tethered lip-tie and posterior tongue tie (class III or IV).
Gastroesophageal Reflux Outcomes
Reflux outcomes were assessed using the GIGER, I-GERQ-R, and GSQ-I scales (Table 4). No study clearly defined whether infants had GER or GERD. The I-GERQ-R scale was the most commonly used (n=5). Studies conducted by Ghaheri 2018, Ghaheri 2017, Hand 2023, Hand 2020, and Slagter 2020 reported in the respective percentage reductions in I-GERQ-R scores at 1 week post-operatively compared to pre-operatively as 23%, 19%, 9%, 15%, and 20% (Supplemental S3).
I-GERQ-R Outcomes.
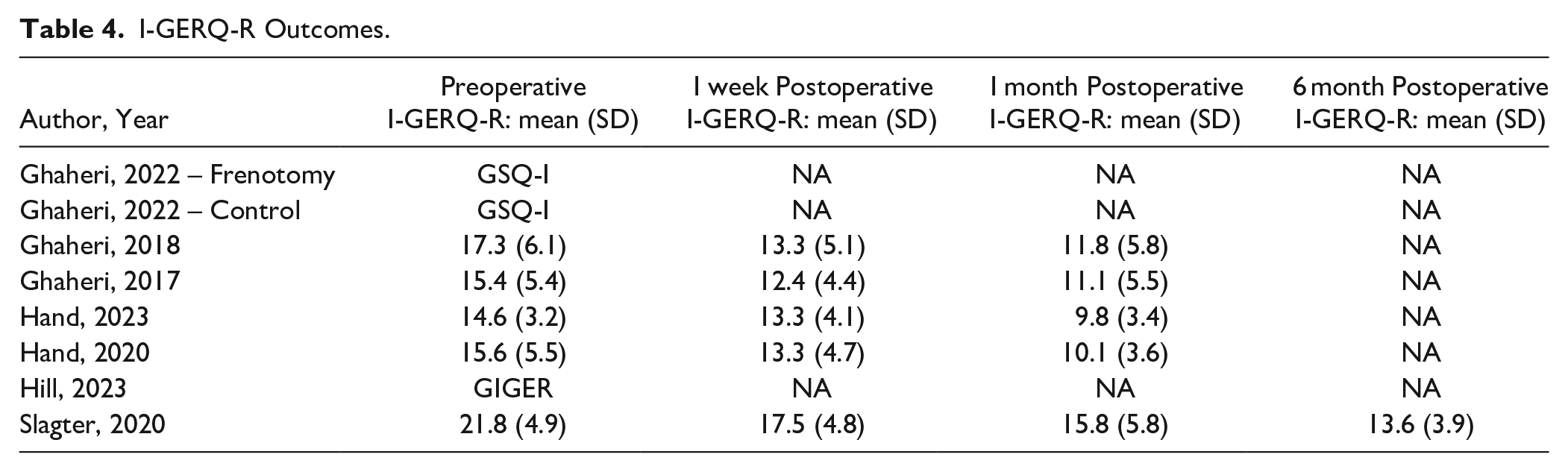
The GSQ-I scale was used by the 1 RCT included in this review, 19 which examined the frequency and severity of vomiting/regurgitation, irritability/fussiness, refusal to feed, choking/gagging, arching back, and episodes of hiccups. This study only assessed post-operative between-group improvement between day 0 and day 10 and reported statistically significant between-group differences on all items of the GSQ-I, favoring the surgical group, with the exception of frequency of irritability/fussiness and severity of choking/gagging, where no statistically significant between-group differences were found (P > .05). Blinding of the intervention was not performed in this study or addressed in the limitations of the study. The GIGER scale was used by Hill 2023 with a total pre-operative score of 51.88 and total 2-week post-operative score of 37.94, indicating improvement in GER symptoms post-frenotomy. No studies utilized pH and MII to quantify reflux, nor endoscopy.
Study Quality
The Newcastle Ottawa Scale was used to assess risk of bias in the cohort studies. The 5 cohort studies ranged from a total score of 4 to 5, indicating a high risk of bias. The randomized control trial also had an overall high risk of bias on Cochrane Risk of Bias analysis (Supplemental S2 and S3).
Discussion
This systematic review aimed to examine the relationship between gastroesophageal reflux outcomes and frenotomy in infants with ankyloglossia. No studies used objective diagnostic tools for diagnosis. However, all studies reported improvements in reflux scores post-frenotomy, suggesting frenotomy could improve symptoms of infantile reflux in patients with ankyloglossia. Given the high risk of bias present in all included studies, definitive conclusions cannot be made. A meta-analysis was not conducted to prevent the formation of definitive conclusions based on poor quality studies. It is also possible, based on previous literature, that there is an alternative explanation for the improvements in scores noted.
Longitudinal studies have demonstrated the incidence of GER gradually declines with age.20 -22 Campanozzi et al prospectively followed 210 infants with GER between 1 and 12 months of age and found that GER scores using the I-GERQ-R scale were significantly higher in infants aged 1 to 5 months compared to >5 months. Overall findings were that regurgitation was absent in 88% of infants at 12 months of age, and no infants demonstrated regurgitation by 24 months. Martin et al 21 prospectively investigated the natural history of infant regurgitation in 693 children and found that regurgitation reached a peak of 41% between 3 and 4 months of age and declined to <5% between 13 and 14 months of age. Nelson et al 22 followed 948 children 13 months old and younger and found that peak regurgitation was 67% at 4 months and by 10 to 12 months of age, only 5% of participants continued to display regurgitation. Similarly, a 2020 study among 157 French babies found that physiological GER peaked at 3 months and most cases resolved on their own. 23 By virtue of the natural history of GER, findings from included prospective cohort studies in the systematic review may be confounded. It cannot be clear whether the improvements reported in reflux scores are attributable to frenotomy or simply a natural resolution of the reflux. As all included studies did not use objective measures to diagnose reflux, misattribution of normal infant behaviors to reflux may also explain resolution of symptoms that were never related to reflux at all. Rigorous study design in the form of RCTs using validated instrumental and self-report measures is warranted to provide more conclusive findings on the efficacy of frenotomy on resolving GER symptoms in infants with ankyloglossia.
Studies included in the systematic review were also varied in the diagnostic criteria used for ankyloglossia. Several of the included studies include division of tethered oral tissues other than ankyloglossia, including restrictive upper labial/maxillary frenula (lip ties) and buccal/cheek ties. Previous systematic review suggests that the evidence supporting division of maxillary frenula is inadequate to support this practice for breastfeeding. 8 The 2020 Consensus Statement published by the American Academy of Otolaryngology defines the upper labial frenulum as a normal structure with unclear significance. 5 Buccal ties have no proven functional significance and should not be divided. 23 In their respective studies, data presented by Hill 2020 and Slagter 2020, are confounded given that isolated tongue tie correction data was not presented.
Included studies also assessed different patient populations which also obscures a conclusive finding. For instance, Ghaheri 2018 only included patients for revision frenotomy, Ghaheri 2022 only included patients with posterior tongue tie. Posterior tongue tie was assessed by most included studies, however the AAO-HNSF was unable to reach a consensus on the definition of posterior tongue tie or utility of frenotomy for posterior tongue tie. 5 As a controversial clinical entity without universally clear diagnostic criteria, it is challenging to interpret studies solely related to division of posterior tongue tie.
The most commonly used questionnaire in our included studies was the I-GERQ-R to evaluate reflux severity. The diagnostic validation of the I-GERQ-R score was designed to define definitely GERD-positive and -negative subjects, which precludes a group of symptomatic non-GERD infants that were not included in the validation of this tool. 25 Large clinical trial data estimates that most referred infants do not undergo endoscopy to confirm diagnosis and therefore, approximately 40% of referred symptomatic infants that do not respond to nonpharmacologic treatment may report symptoms not caused by GERD.25,26 As such, this group of infants pose as confounders as they are not expected to respond to GERD pharmacotherapy better than placebo. Given the limitation of questionaries, additional objective evidence is helpful, such as esophageal pH monitoring or esophageal biopsy. 25 In fact, current gastroenterology professional association guidelines recommend using the MII-pH (multichannel intraluminal impedance-pH) study to correlate troublesome symptoms with reflux episodes, though this is rarely performed in well infants. 24 Given that included studies only used questionnaires as a measure of reflux, findings may be skewed given the lack of testing for children with nonacid reflux and those with physiologic reflux.
The current literature is inconclusive on the utility of frenotomy in treating reflux. While frenotomy is a fast, in-office procedure, subjecting infants to procedural intervention without adequate cause does not constitute good clinical care. Though complications are uncommonly reported, they are possible, and their frequency may not be adequately represented in the literature given the variety of settings in which the procedure is performed. Possible procedural complications include bleeding, tongue tip anesthesia from nerve injury, and oral aversion. 27 Little is known about the effect of frenotomy on infant feeding outside of breastfeeding, and studies have not methodically examined the feeding metrics of infants with ankyloglossia. 28 Though this intervention may be offered in correctly selected patients for maternal pain with latch associated with ankyloglossia after appropriate conservative measurements, current data does not conclusively support frenotomy for GER/GERD alone.
Results of 6 prospective cohort studies and 1 RCT suggest that frenotomy may result in improvements in GER symptoms in infants with ankyloglossia. However, low study quality and high risk of bias, preclude definitive and reliable conclusions from being made. Therefore, this study focused on the critical appraisal of existing literature as a means to call for more rigorous investigation and encourage critical judgement when considering frenotomy for this indication without good clinical cause.
Conclusion
This systematic review presents data on 7 studies examining the relationship between gastroesophageal reflux and frenotomy in infants with ankyloglossia. No studies used objective tools like pH and MII to quantify infant reflux. Although improvements in reflux scores were reported post-frenotomy, small sample sizes, a lack of adequate controls, inappropriate measurement tools, and a high risk of bias precludes a definitive conclusion. Future RCTs using validated instrumental and self-report measures are warranted to further elucidate the efficacy of frenotomy on resolving GER symptoms in infants with ankyloglossia.
Supplemental Material
sj-docx-1-aor-10.1177_00034894241297584 – Supplemental material for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review
Supplemental material, sj-docx-1-aor-10.1177_00034894241297584 for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review by Ashaka Patel, Katrina Cirone, Sami Khoury, Edward Madou, Agnieszka Dzioba, Dhandapani Ashok, Julie E. Strychowsky and M. Elise Graham in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-docx-2-aor-10.1177_00034894241297584 – Supplemental material for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review
Supplemental material, sj-docx-2-aor-10.1177_00034894241297584 for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review by Ashaka Patel, Katrina Cirone, Sami Khoury, Edward Madou, Agnieszka Dzioba, Dhandapani Ashok, Julie E. Strychowsky and M. Elise Graham in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-docx-3-aor-10.1177_00034894241297584 – Supplemental material for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review
Supplemental material, sj-docx-3-aor-10.1177_00034894241297584 for The Impact of Frenotomy on Gastroesophageal Reflux in Pediatric Ankyloglossia: A Systematic Review by Ashaka Patel, Katrina Cirone, Sami Khoury, Edward Madou, Agnieszka Dzioba, Dhandapani Ashok, Julie E. Strychowsky and M. Elise Graham in Annals of Otology, Rhinology & Laryngology
Footnotes
Acknowledgements
The authors would like to thank Mr. Darren Hamilton for his assistance in designing the search strategy.
Author Contributions
AP: study design, data collection/curation, drafting of the manuscript; KC: data collection/curation, critical review of manuscript; SK: data analysis, critical review of manuscript; EM: study design, statistical analysis, critical review of manuscript; AD: study design, statistical analysis, critical review of manuscript; DA: study design, critical review of manuscript; JS: study design, data validation, critical review of manuscript; MG: study design, data curation, data validation, critical review of manuscript. All authors approved the final version of the manuscript.
Consent to Participate
N/A: There were no patient participants.
Consent for Publication
N/A.
Data availability
On reasonable request
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
N/A: Institutional IRB not required (systematic review).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.