
Abstract
Objective:
to investigate the ability of mandibular distraction osteogenesis (MDO) to avoid gastrostomy tube (G-tube).
Data Sources:
PubMed, EBSCOhost, Cochrane, and Embase.
Review Methods:
We retrospectively reviewed the number of MDO cases performed at our institution for patients with Robin Sequence (RS) over the past 10 years. In our institutional review, patients were excluded if they had a G-tube already placed at the time of surgery. We also performed a systematic review of the literature. Articles were excluded if they did not detail feeding outcomes after MDO, or if MDO was performed on patients that did not have RS.
Results:
In our systematic review, 12 articles were included that comprised a total of 209 neonates with RS that underwent MDO. A total of 174 (83.3%) patients avoided a G-tube once MDO was performed. A total of 14 patients met the inclusion criteria at our institution. Of the 14 RS patients, 9 (64%) avoided having a G-tube placed and all (14/14) avoided tracheostomy. The average birth weight of patients avoiding a G-tube was 3.11 kg compared to 2.25 kg (P = .045) in the group requiring a G-tube. In the group avoiding a G-tube, the average weight at time of operation was 3.46 kg compared to 2.83 kg (P = .037) in the group requiring a G-tube.
Conclusion:
MDO may be considered as a surgical option to prevent G-tube placement for neonates with non-syndromic RS who have difficulty with PO feeding but whose airway obstruction is not severe enough to require respiratory support. Based on our institutional experience, a minimum weight of 3.00 kg correlated with higher success rates of PO intake and avoiding a G-tube.
Introduction
Robin Sequence (RS) is a rare condition defined by a combination of micrognathia, glossoptosis, airway obstruction, and sometimes accompanied by cleft palate. RS occurs in 1/8500 live births and presents as a wide spectrum of symptom severity. Some patients do not require any airway management and are able to maintain oral intake without issue, while others can experience life-threatening upper airway obstruction.1,2 If a child with RS has airway obstruction not relieved with conservative measures (eg prone or side positioning and nasal trumpet), there are surgical options including tracheostomy, tongue-lip adhesion (TLA), and mandibular distraction osteogenesis (MDO). Tracheostomy is a definitive treatment for upper airway obstruction but is associated with significant morbidity and long-term costs. 3 Over the last couple of decades, numerous studies have shown MDO to be a more effective alternative to tracheostomy and TLA, while also addressing the primary problem of a deficient mandible. Studies have shown MDO to effectively improve upper airway obstruction and avoid the need for tracheostomy.3 -6
The impact of RS extends beyond the airway for these infants with well-documented impairment to nutrition and weight gain in the first year of life. 7 Previous research by Lidsky et al 8 has shown promising results for early airway intervention in patients with isolated RS associated with lower rates of G-tube placement compared to late or no surgical intervention. One interesting cohort of patients with RS is those who do not require respiratory support measures beyond prone/side positioning but are unable to sustain adequate oral feeding. Due to their inability to maintain coordinated feeding, these patients require enteric feeds to provide adequate nutrition. MDO may be particularly beneficial to this cohort, as it has been shown to improve the ability of neonates with RS to take oral feeding, with 80% to 100% of patients resuming oral feeds after the procedure.3,9 -12 Correction of the upper airway obstruction and glossoptosis allows for coordination of the suck-swallow-breath reflex, less effort and energy expenditure, and relief of gastroesophageal reflux (GER).9,10 Ultimately, the improved upper airway patency and facial skeletal profile allow for better oxygenation during feeding, thus allowing patients to be weaned from pre-operative enteric feeding. 13
Though prior studies on post-MDO feeding outcomes commonly focus on transition to oral feeding, many of these patients also achieve a valuable secondary outcome by avoiding pre-operative placement of a gastrostomy tube (G-tube). Eliminating G-tube placement results in better patient quality of life, fewer surgeries, and a lower burden on caregivers. While the primary indication for MDO in patients with RS is to relieve upper airway obstruction, few studies have specifically investigated the ability of MDO to outright avoid G-tube. Through a retrospective review of patients with RS that underwent MDO at our institution and a systematic review of the literature, we aim to investigate how often this patient population is able to avoid G-tube placement.
Methods
This study was approved by the institutional review board (IRB) at Vanderbilt University Medical Center IRB #190840. This study is a review of patients from our institution with a systematic review of the literature. Full-text review was conducted by following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. We retrospectively reviewed the number of MDO cases performed at our institution for patients with RS over 10 years (2011-2020). To evaluate the number of patients that avoided having a G-tube placed via this procedure, patients were excluded if they had undergone G-tube placement prior to or concurrent with the time of MDO. Other exclusion criteria included performing MDO for diagnoses other than RS, such as hemifacial microsomia. Patients with additional developmental or neurologic limitations (e.g hypotonia or genetic diagnoses) were not excluded from the study. Patient data were collected through a retrospective review of their electronic health records (EHR). This included patient gestational age, age at operation, birth weight, weight at operation, feeding status, time from operation to discharge, and genetic syndromes. The characteristics of patients avoiding gastrostomy were compared to the characteristics of those requiring gastrostomy, and significance was determined with a t-test assuming unequal variances.
For the systematic review of the literature, Pubmed, EBSCOhost, Cochrane, and Embase were queried for terms singularly and in combination including “mandibular distraction osteogenesis,” “dysphagia,” “swallow,” “gastrostomy,” “G-tube,” “feeding tube,” and “enteral nutrition.” The search strategy filtered for publications in English and surgeries performed only on human subjects. Search strategies were defined in collaboration with academic librarians, which allowed for the creation of comprehensive search queries optimized for each database to reduce bias at the level of the search terms. These query terms can be viewed in Supplemental Appendix. This study was primarily interested in the feeding outcomes from MDO surgeries, with all surveyed outcomes displayed in Table 2. A total of 52 unique articles resulted across the 4 databases, with the triage process shown in Figure 1. After reviewing the results, studies discussing outcomes of MDO that involved feeding outcomes were reviewed. Articles were excluded if they did not explicitly detail feeding outcomes after MDO, or if MDO was performed on patients that did not have RS. If the article discussed feeding outcomes but did not detail whether the patients had G-tubes prior to MDO, then it was excluded. Any studies with missing data were considered to not meet inclusion criteria. These strict exclusion criteria to identify studies reporting on binary outcomes helped minimize ambiguity in interpretation of studies and bias among reviewers. A total of 12 articles were included in the review (date last accessed: March 2023). The primary and secondary authors (EM and SK) and principal investigator (RB) worked together in the selection and screening process.
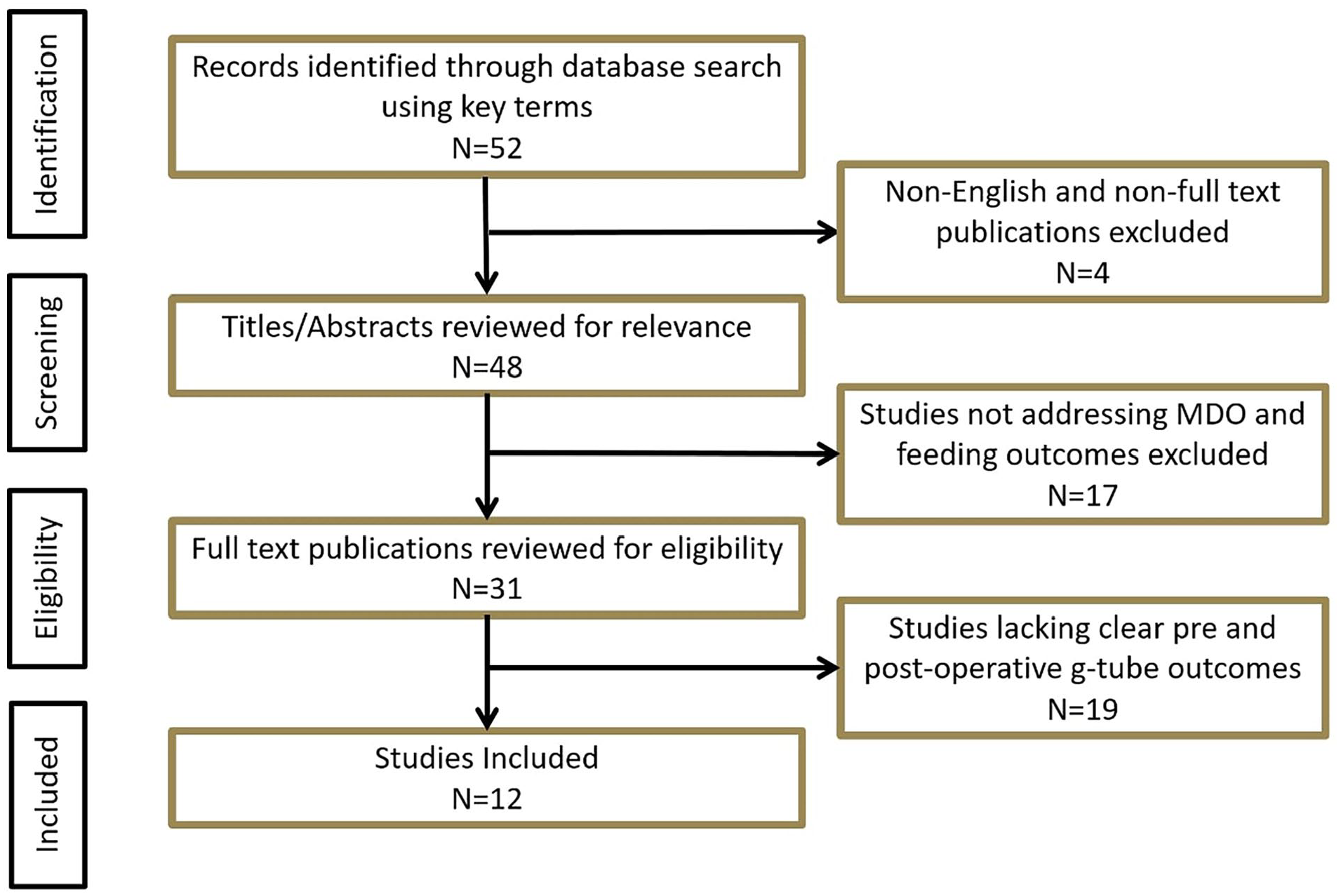
Systematic review of literature assessing gastrostomy outcomes after MDO.
Results
Between the years 2011 and 2020, 26 patients were identified to have undergone MDO at Vanderbilt Children’s Hospital. We have detailed our surgical technique for MDO in a previous article. 14 Eleven of these patients had gastrostomy tube placement prior to MDO, so these patients were excluded. One patient was excluded because mandibular distraction was performed for cosmetic correction in an older child without feeding difficulties. Of the 14 patients included in this study, 9 were able to tolerate full PO feeds and did not have G-tube placed, while 5 required G-tube placement after MDO due to not being able to fully take PO after surgery. Characteristics of these patients are further demonstrated in Table 1.
Comparison of Patients Avoiding Gastrostomy to Patients Requiring Gastrostomy at Our Own Institution.
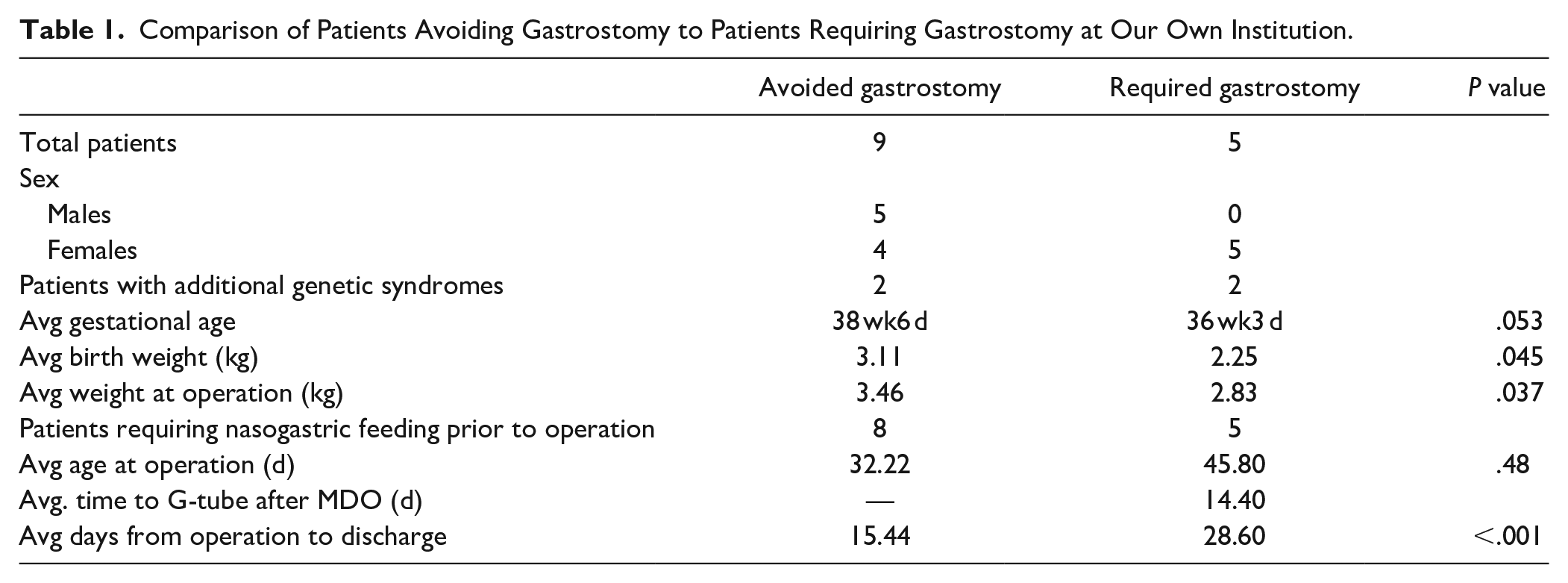
Of the 9 patients who avoided gastrostomy, 2 had additional genetic syndromes, which were Stickler Syndrome and spondyloepiphyseal dysplasia congenita. Two out of the 5 requiring G-tube also had additional genetic syndromes, which were Marshall Smith Syndrome and Nager Syndrome. All 14 patients avoided tracheostomy. Patients that ended up requiring G-tube were more likely to be more premature (36 weeks3 days vs 38 weeks6 days; P = .053). Patients that had G-tube placed after MDO also had a statistically significant difference in weight (2.83 kg vs 3.46 kg) at time of surgery (P = .037), birth weight (P = .045), and longer inpatient stay after surgery (P < .001). There was no statistical significance in age (in days) at time of operation of MDO.
For the systematic review of the literature, 12 publications were found to report on tube feeding outcomes of patients undergoing mandibular distraction. All 12 of those publications had details on feeding prior to MDO and the postoperative course. The dates of these articles ranged from 2003 to 2022. The 12 articles totaled 209 patients with 174 (83.3%) of the patients avoiding G-tube after MDO. Thirty-five patients (16.7%) required a G-tube post-operatively. The results of this review are displayed in Table 2.
Literature Review Results Evaluating Feeding Outcomes of Patients Undergoing MDO for RS.

Discussion
Complications from G-tube placement can range from minor postoperative complications such as wound infection to major complications (gastric separation or gastrocolonic fistula) with about 10% of patients having a major complication within 6 to 12 months of placement.24 -27 Furthermore, the burden on caretakers cannot be understated. Children with G-tubes often require double the home care costs of medically-complex children without G-tubes. 28 The ability to feed an infant without G-tube assistance can be life-changing for families. This is especially true in rural settings, areas without home nursing coverage, or families without strong social support. The primary indication for MDO in infants with RS is to relieve upper airway obstruction, and often to avoid a tracheostomy, but it is also important to know that G-tubes can be avoided in many patients with RS. This emphasizes the need to have craniofacial surgery teams consulted early in the patient’s course to help counsel and potentially avoid pre-emptive G-tube placement prior to possible MDO surgery.
Our systematic review reveals 83.3% of infants with RS did not require G-tube after MDO. Our institutional case series and systematic review results indicate MDO helps a large portion of infants avoid future gastrostomy. Because gastrostomy placement was not the primary outcome measured in the majority of these publications, it is difficult to compare characteristics of the patients in the systematic review who avoided G-tube versus those that required it after their operation.
The results from our institution help demonstrate what factors may influence post-surgical outcomes and the eventual need for gastrostomy in these patients. At our institution, 9 out of 14 (64.3%) infants with RS avoided G-tube placement after MDO and were maintaining oral nutrition at the time of discharge. There were several differences between the group that avoided G-tube compared to the group that required G-tube. The patients who required gastrostomy had significantly lower birth weight than those who avoided gastrostomy, which is likely related to this group also having an earlier gestational age. In addition to predisposing infants to low birth weight, gestational age is associated with swallowing difficulties and limitations in infant feeding capabilities. This is because of immature sucking skills and poor suck-swallow-breath coordination.29 -32 The ability to feed orally can be even more challenging for preterm infants due to cardiopulmonary instability, resulting in desaturations and bradycardia during feeds.33,34 Previous studies have shown that preterm infants continue to struggle at equivalent postmenstrual ages compared to term infants when assessing various feeding measures, including arousal, tongue positioning, aspiration, and ability to complete the feed. 35 It is therefore unsurprising that the patients requiring G-tube placement after MDO had a younger average gestational age since this is an independent risk for poor feeding in addition to their micrognathic mandible. Gestational age may be an important factor for physicians to consider when anticipating feeding outcomes in infants undergoing MDO. It is also possible that these results reflect low birth weight as a risk factor for G-tube placement independent of prematurity status. Handley et al 36 have found that infants with intrauterine growth restriction (IUGR) have 4 times increased risk for requiring surgical airway intervention, hence IUGR may pose a similar risk for requiring G-tube placement. With a limited sample size, it was not possible to perform multivariate analysis to delineate these 2 patient characteristics.
Weight at the time of operation was also significantly greater in patients avoiding gastrostomy compared to those requiring gastrostomy in our retrospective review. Previous studies assessing weight at time of operation have indicated that it is overall safe and effective to perform MDO in infants weighing less than 4 kg. Tahiri et al 37 demonstrate no difference in complication rates after MDO for infants in the very low weight group (mean 3.1 kg) compared to those in the higher weight group (mean 11 kg). The complications included device failure, premature ossification, fibrous nonunion, and abscess, but this did not assess feeding outcomes. When specifically evaluating feeding outcomes, Taufique et al 23 found no significant difference in postoperative G-tube rates when comparing infants above and below 3 kg. Alternatively, the results from our institution suggest there may be better G-tube outcomes if infants can reach 3 kg before the time of operation, but definitive interpretation of these results are limited by inability to perform multivariate analysis of our data to assess for the impact of confounding comorbidities. Furthermore, delaying the time of operation for the sake of weight gain may not always be beneficial, especially if this would require operation at greater than 3 months. Infants have been shown to have better early post-operative weight gain when MDO is performed at less than 3 months of age. 38 Therefore, the timing of surgery must balance the goals of pre-operative weight gain and early intervention.
Another factor to consider when evaluating patients with RS for MDO is the presence of comorbid syndromic diagnosis. Among patients at our institution, there was no clear impact of syndromic RS on the post-surgical G-tube outcomes. However, previous literature has described greater challenges in the treatment of syndromic RS patients. Spring et al 11 describe a significant association between the presence of multisystem genetic syndrome and postoperative feeding disorder, which was defined as requiring nasogastric or G-tube feeding for greater than a month after operation. The challenge of treating syndromic RS is not exclusive to mandibular distraction. In their review of patients undergoing MDO, tracheostomy, TLA, or no operation, El Ghoul et al 20 demonstrate higher rates of G-tube placement in syndromic patients across all groups. Susarla et al report similar findings in their cohort of patients undergoing MDO or TLA, with syndromic diagnosis conferring an increased risk for gastrostomy. 3 Ultimately, for these more complex patients with syndromic RS, physicians and families may not expect to see as significant of a feeding benefit postoperatively, and it will be important to address other comorbidities to optimize feeding outcomes.
Beyond the specific measure of gastrostomy prevention, Hong et al 16 provide insight into the functional improvements in feeding seen after MDO for patients with RS. All 6 patients included in their study required nasogastric or nasoduodenal tube feeding due to swallowing difficulties and failure to thrive prior to treatment. Pre-operative video fluoroscopy showed penetration, abnormal tongue movements, abnormal transit time, and laryngeal elevation in all patients. After distraction was completed, modified barium swallow tests showed significant improvement in all parameters for each patient, supporting the role of MDO in improving oral feeding for infants with RS. This improvement in feeding abilities after MDO is further demonstrated by the trajectory of post-operative weight gain with greater than expected average daily weight gain and growth velocity, especially in patients with isolated RS.39,40 It is hypothesized that the post-operative weight improvements can be attributed to improvements in oral feeding mechanisms as well as reduction in work of breathing once MDO has relieved upper airway obstruction and glossoptosis. 39
When comparing outcomes across surgical interventions, it has been well documented that MDO is the superior option for airway outcomes in comparison to TLA. MDO has shown to have lower tracheostomy rates, higher rates of decannulation, and higher oxygen saturations, as well as having the benefit of addressing the root cause of obstruction.10,41 Retrospective review by El Ghoul et al 20 supports that MDO is also superior to TLA in regard to G-tube outcomes in infants with RS. In their study assessing feeding outcomes, they demonstrate that patients with RS undergoing MDO had the lowest percentage of post-operative G-tube placement at 33%, compared to 61% in patients undergoing TLA, and 89% in patients undergoing tracheostomy. However, some studies report contradicting feeding outcomes when comparing the 2 surgical interventions. Khansa et al 18 found no difference in gastrostomy outcomes in patients undergoing MDO, TLA, or conservative management.
This systematic review consolidates the available literature reporting on gastrostomy outcomes in this unique population, and our retrospective review expands upon the limited sample size that has previously been published. There are several limitations to this study, including the exclusion of any non-English publications. Additionally, further meta-analysis to evaluate the different characteristics among G-tube outcomes was not possible because, in many of these studies, this was a secondary outcome measure. Few studies elaborated on these specific groups’ characteristics, like syndromic status, age, and weight. A limitation of the retrospective review of patients at our institution is a lack of multivariate analysis due to the small sample size. There is also no true control group comparing gastrostomy outcomes in patients with RS who did not undergo MDO. This is because patients treated conservatively without surgery likely have adequate oral feeding without intervention and are at less risk of requiring a G-tube. Future, prospective studies could better delineate the ability of MDO to prevent G-tube placement and identify the role of baseline nutrition in feeding outcomes. There have been previous studies on the cost-benefit analysis of MDO versus tracheostomy showing MDO having lower long-term costs, but it may be useful for future studies to look at the cost-benefit analysis of MDO versus G-tube placement as well.
Conclusion
MDO has gained wide acceptance as a procedure to improve airway obstruction and avoid tracheostomy in neonates with RS. A secondary benefit is the avoidance of G-tube placement. In neonates with non-syndromic RS whose airway obstruction is not severe enough to require respiratory support, MDO may be considered as a surgical option with the primary goal of improving their ability for PO intake and ultimately preventing the need for G-tube placement. Based on our institutional experience, neonates that weighed at least 3 kg at time of surgery had higher rates of G-tube avoidance, but further investigation is necessary to determine ideal weight for surgical timing. Other patient characteristics that may impact feeding outcomes are gestational age, comorbid genetic syndromes, and neurological impairment.
Supplemental Material
sj-docx-1-aor-10.1177_00034894241249547 – Supplemental material for Pre-Operative Characteristics Helping to Avoid Gastrostomy Tube After Mandibular Distraction in Neonates With Pierre-Robin Sequence: A Institutional Case-Series and Review of the Literature
Supplemental material, sj-docx-1-aor-10.1177_00034894241249547 for Pre-Operative Characteristics Helping to Avoid Gastrostomy Tube After Mandibular Distraction in Neonates With Pierre-Robin Sequence: A Institutional Case-Series and Review of the Literature by Emily L. Mace, Shreyas G. Krishnapura, Michael Golinko, James D. Phillips and Ryan H. Belcher in Annals of Otology, Rhinology & Laryngology
Footnotes
Author Contributions
Emily L. Mace: Methodology, analysis, and manuscript draft preparation. Shreyas G. Krishnapura: manuscript draft preparation and review and editing. Michael Golinko: Manuscript review and editing. James D. Phillips: Conceptualization, methodology, and manuscript review and editing, Ryan H. Belcher: Conceptualization, methodology, analysis, manuscript draft preparation, and review and editing.
Authors’ Note
Presentation: poster presentation at ASPO Annual Meeting, virtual meeting at COSM, April 9-11, 2021
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.