
Abstract
Objectives:
To evaluate audiologic consequences of gunshot wounds (GSWs) to the temporal bone (TB), and to correlate hearing outcomes with neurologic and vascular injuries adjacent to the temporal bone.
Study design:
Retrospective case series.
Setting:
University-based level-one trauma center.
Methods:
Retrospective review of 35 patients surviving TB ballistic injury, 2012 to 2021. Main outcomes were audiologic results. Demographics, concomitant injuries, CT, and interventions were reviewed.
Results:
Mean age was 30.7 years; 80% male. Seventeen patients (48.6%) underwent audiologic testing. Mean pure tone average (PTA) was 75 ± 35 dB, bone line average 41 ± 26 dB, and speech discrimination score (SDS) 60 ± 43%. Nineteen (54.3%) demonstrated facial nerve injury (FNI), who were more likely to show SNHL especially anacusis, though their mean PTA and SDS were not statistically different from those without (P = .30 and .47, respectively). Radiographic review of those with sensorineural loss (SNHL, 6/17) revealed otic capsule-disrupting fracture (n = 2), pneumolabyrinth (n = 2), intracranial hemorrhage (n = 3). Those with mixed loss (6/17) showed otic capsule-sparing fracture (n = 6), EAC injury (n = 5), ossicular discontinuity (n = 2), and intracranial hemorrhage (n = 4). Two with mastoid tip fractures alone had normal audiograms. Audiometric outcomes were not predicted by concomitant CSF leak, spinal injuries, vascular injuries, cranial neuropathies, or traumatic brain injury.
Conclusions:
All patterns of hearing loss—conductive, sensorineural, mixed and normal—may be seen following TB ballistic injuries. Trauma severe enough to disrupt the facial nerve is more likely to cause anacusis. However, all should be formally evaluated, since ballistic injuries complicated by neurologic or vascular damage do not necessarily correlate with worse audiologic outcomes, while patients with minimal fractures may demonstrate losses.
Keywords
Introduction
Gunshot wounds (GSW) to the temporal bone are the etiology of only 3% of temporal bone fractures. 1 Though rare, GSW injuries require particular attention due to their potential for more severe and extensive damage compared with blunt trauma. 2 Structures at risk include those within and immediately adjacent to the temporal bone. This includes the facial nerve, cochlea, labyrinth, ossicles, tympanic membrane, pinna, external auditory canal (EAC), carotid artery, jugular vein, dura, and lower cranial nerves. Prior studies have provided limited audiologic data following GSW to the temporal bone.2–8 In this study, we aimed to understand the patterns and levels of hearing loss from temporal bone ballistic trauma and their relation to intratemporal involvement and adjacent neurologic and vascular injuries.
Methods
A retrospective chart review was performed for patients evaluated following temporal bone ballistic injury at a single institution, university-based level-one trauma center over a 10-year span (2012-2021). Institutional Review Board approval was obtained (Louisiana State University Health Sciences Center New Orleans IRB #1636, exempt). Inclusion criteria required a temporal bone fracture of any portion of the bone resulting from a GSW. Patients who died within 72 hours were excluded. The main outcomes were audiologic results including pure tone average (PTA), bone line average, and word recognition scores (WRS). PTA was calculated as the mean of the air conduction scores at 500, 1000, 2000, and 4000 hertz (Hz). When the frequency was inaudible, 120 dB was substituted for that frequency. Bone line average representing the sensorineural component was calculated as a mean of the same frequencies. The ear contralateral to the fracture served as a control. The control ear demonstrated normal hearing in all patients tested except two: one with conductive hearing loss in the setting of chronic otitis media with effusion, and the other with normal sloping to moderate high frequency sensorineural hearing loss at least 40 dB better than the injured ear at all frequencies. None reported known preexisting hearing loss or prior traumatic brain injury. Demographics, facial nerve status, CT images, interventions, and complications were additionally reviewed. Continuous variables were compared using non-paired Student’s t tests.
Results
Demographics
Of the 42 patients with GSW to the temporal bone identified and reviewed, 7 mortalities from nonsurvivable intracranial injuries occurred, while 35 patients survived (patient details listed in Table 1). Mortalities were included in the demographic review, but were excluded from further analysis. Most patients were male (80%) with a mean age of 30.7 years (range 5-58). 68.6% were African American/Black, 17.1% white non-Hispanic, 8.6% white Hispanic, 2.9% Asian, 2.9% not identified. In Orleans Parish, 60.1% of residents are African American/Black, 30.9% white non-Hispanic, 5.5% white Hispanic, 2.9% Asian, 0.6% other. Thus, race/ethnicity of those injured approximated the demographics of the surrounding community. Each ear was affected at approximately equal rates (51% left).
Patient Injuries, Interventions and Outcomes.
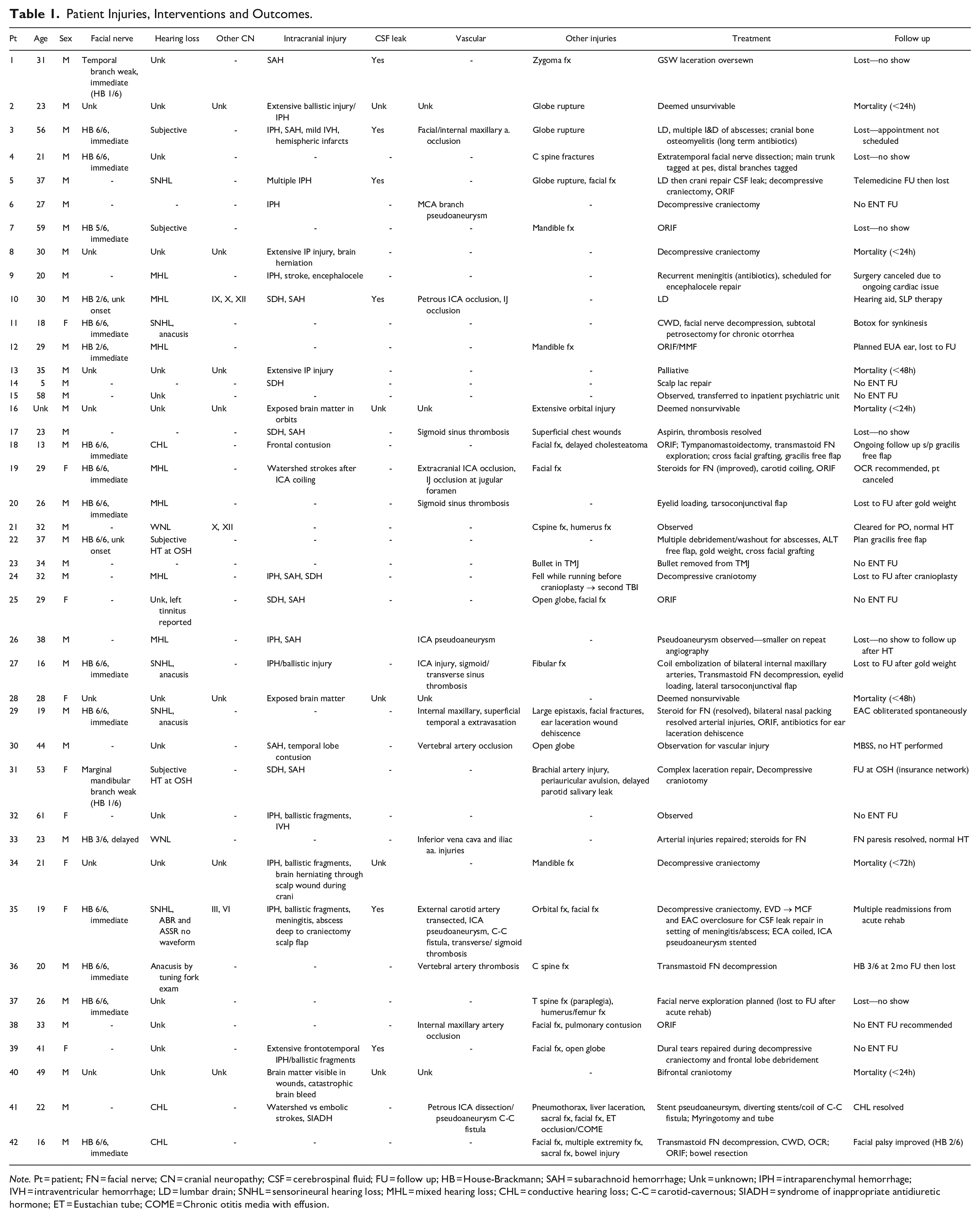
Note. Pt = patient; FN = facial nerve; CN = cranial neuropathy; CSF = cerebrospinal fluid; FU = follow up; HB = House-Brackmann; SAH = subarachnoid hemorrhage; Unk = unknown; IPH = intraparenchymal hemorrhage; IVH = intraventricular hemorrhage; LD = lumbar drain; SNHL = sensorineural hearing loss; MHL = mixed hearing loss; CHL = conductive hearing loss; C-C = carotid-cavernous; SIADH = syndrome of inappropriate antidiuretic hormone; ET = Eustachian tube; COME = Chronic otitis media with effusion.
Hospital Course
Patients were hospitalized on average 14.8 ± 13.5 days (range 0-47). On arrival, mean Glasgow Coma Scale (GCS) was 12.3 ± 4.2. The majority (63%) required intubation, typically for altered mental status (present in 54%). Most patients were discharged home (51.4%) or to an acute rehabilitation facility (29.0%). Two patients were transferred to an inpatient psychiatric ward, 2 to a pediatric intensive care unit at a children’s hospital, 2 had an unknown disposition, and one was released to law enforcement. At least one patient discharged home remained on house arrest, though this was not routinely documented in the chart, so the rate of this social limitation remains unknown.
Audiologic Results
Subjective hearing loss was reported by 57.1% of patients during their hospital stay. All patients with temporal bone trauma evaluated by the otolaryngology service at our institution are recommended to follow up in clinic with an audiogram in approximately 4 to 8 weeks after injury. In this cohort, audiograms were performed in 17 patients (48.6%). These were obtained, on average, 3.8 months after injury (range 0-18 months). Mean pure tone average (PTA) was 75 ± 35 dB, bone line average 41 ± 26 dB, and speech discrimination score (SDS) 60 ± 43% (with median and range also listed in Table 2). Graphical representation of audiometric outcomes following the AAO-HNS standard for reporting hearing results are seen in Figure 1. Overall, 18% (3/17) had serviceable hearing (PTA < 50 dB and SDS > 50%): two with normal hearing thresholds and one with a conductive loss due to serous effusion complicating Eustachian tube injury. An additional 6 patients had SDS > 50% but PTA > 50 dB, due to their air bone gap. Of those 6, two underwent surgery to address the conductive loss, 3 were offered surgery but canceled, and one was lost to follow up after audiogram.
Audiologic Results.
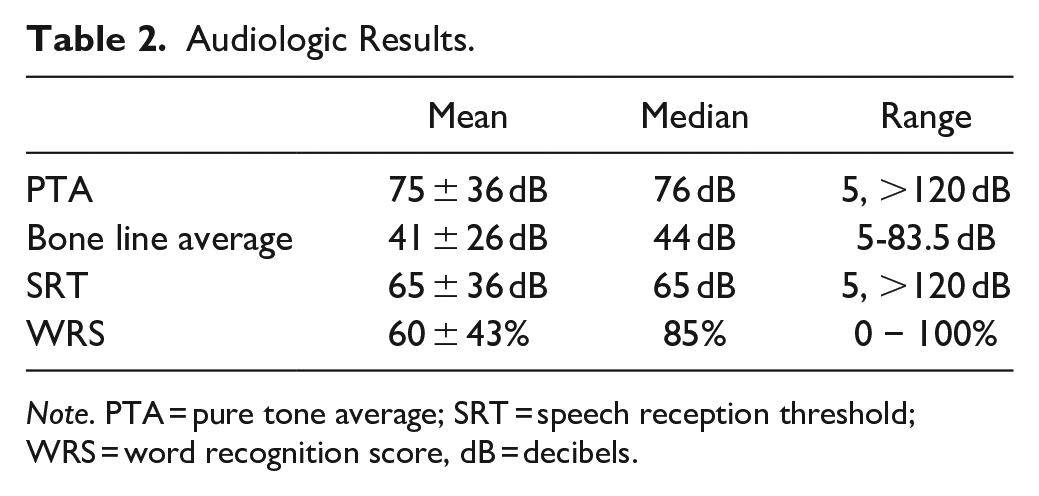
Note. PTA = pure tone average; SRT = speech reception threshold; WRS = word recognition score, dB = decibels.
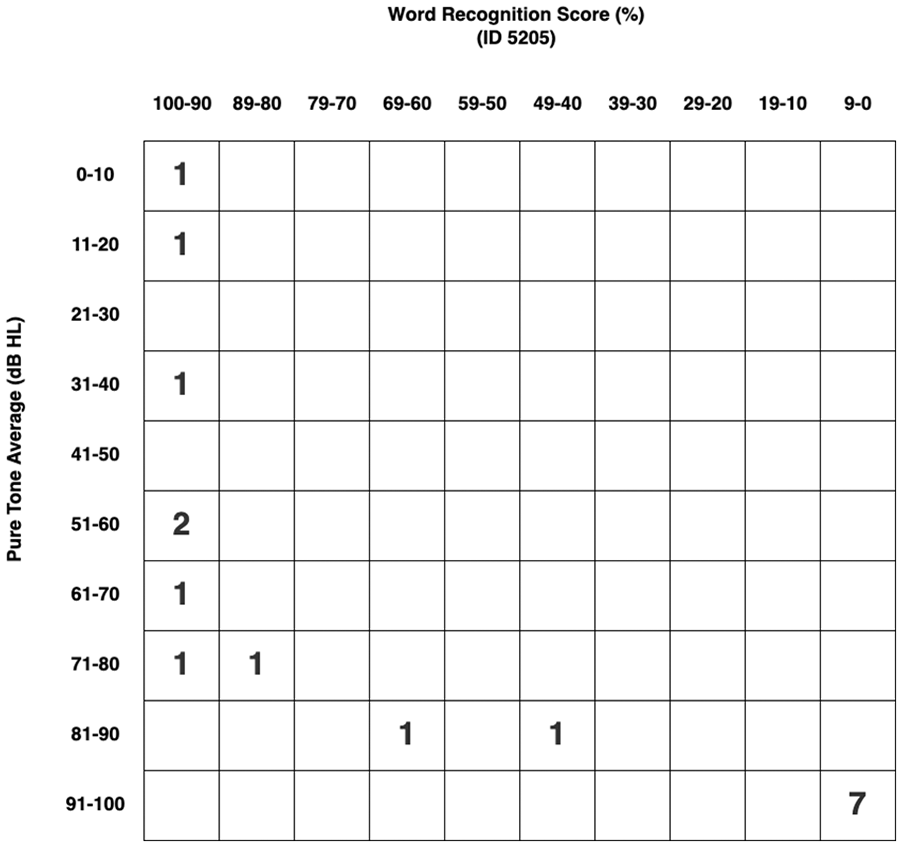
Graphical representation of audiologic results following the 2012 American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) minimum standard for reporting hearing results.
Sensorineural loss (SNHL) was very common, with 70.5% of patients demonstrating some component of sensorineural loss, either sensorineural alone or a mixed loss. Six patients (35.3%) demonstrated a pure SNHL without conductive component. Radiographic review of those patients revealed otic capsule-disrupting fractures and pneumolabyrinth in one-third (n = 2), only EAC and mastoid tip fracture in one-third (n = 2), and an association with intracranial hemorrhage in half (n = 3). Five of those patients demonstrated anacusis, and all of those had concomitant ipsilateral complete facial paralysis.
Mixed hearing loss (MHL) was seen in 6 patients (35.3%), all with CT evidence of otic capsule sparing fracture (n = 6), most with external auditory canal (EAC) injury (n = 5) and intracranial hemorrhage (n = 4). Ossicular discontinuity was evident in 2 patients with mixed hearing loss. All were observed due to the severity of the sensorineural component of their mixed losses, precluding meaningful benefit from ossiculoplasty.
Purely conductive loss (CHL) was present in 3 patients (17.6%), all of whom were treated surgically (further described in “Surgical intervention” below). Normal audiograms were obtained in 2 patients (11.8%), who both had isolated mastoid tip fractures. Two additional patients were seen in otolaryngology clinic but did not undergo audiometric evaluation: One (Patient 30) reported no subjective hearing loss and his appointment addressed a chief complaint of dysphagia, and the second (Patient 36) was seen following transmastoid facial nerve decompression and planned for audiogram but subsequently was lost to follow up. No preoperative inpatient audiogram was described or available in the chart for this patient.
Surgical Intervention
Surgical intervention was performed in all 3 patients with conductive hearing loss. Patient 18 underwent tympanomastoidectomy with ossiculoplasty for cholestesteatoma with maximal CHL. This was performed 1 year after injury by a pediatric otolaryngologist at the children’s hospital. Simultaneous attempted transmastoid facial nerve exploration for persistent flaccid facial paralysis was unsuccessful due to scar formation at the stylomastoid foramen. Postoperatively, the patient developed acquired EAC stenosis refractory to 5-fluorouracil requiring several revision canalplasty surgeries. His hearing improved to a mild CHL (PTA 21.5 dB). He subsequently underwent cross facial grafting and gracilis free flap for facial reanimation.
Patient 41’s bullet trajectory involved the Eustachian tube and carotid canal requiring stenting of a petrous carotid dissection and pseudoaneurysm. He developed chronic serous otitis media and CHL (PTA 40 dB), due to scarring of the Eustachian tube in its bony segment. Myringotomy and tube placement was performed with resolution of his CHL.
Patient 42 underwent ossiculoplasty during canal wall down tympanomastoidectomy and facial nerve decompression in the acute setting for complete facial paralysis and visible bony spicules and ballistic fragments compressing the tympanic and mastoid segments of the facial nerve. He was noted to have incus dislocation and fracture of the stapes crura; therefore, total ossicular replacement prosthesis (TORP) was placed. In the postoperative period, his wide meatoplasty scarred and became atretic. Due to meatal atresia, he retained a maximal conductive hearing loss (PTA 70 dB) and is currently scheduled for revision canal wall down mastoidectomy and meatoplasty.
Facial Nerve Injury
Facial nerve injury was noted in 19/35 patients (54%), which was immediate in 13, delayed onset in 1 and unknown timing in 5 due to altered mental status. The average House-Brackmann score 9 for those with facial nerve injury was 5/6 including 13 with complete flaccid paralysis and 2 with isolated peripheral branch weakness due to concomitant injury in the facial soft tissues (one temporal branch, one marginal mandibular branch weakness). Of the 19 with facial nerve involvement, 10/19 (52%) improved their HB score, including all 4 patients who underwent transmastoid facial nerve decompression in the acute period (<4 weeks after injury). 10 Ten patients (53%) underwent audiogram. Though those with facial nerve injury seemed to have slightly worse mean audiologic outcomes (higher mean PTA 83vs 63 dB, and lower SDS 48%vs 66%), this was not statistically significant (P = .30 and .47, respectively). All patients with audiometrically-documented anacusis had a complete facial nerve paralysis
Traumatic Brain Injuries
Intracranial injuries were common, occurring in 57.1% of patients (n = 20). Half of those underwent audiometric testing, all (100%) documenting hearing loss of a sensorineural (n = 3), mixed (n = 5) or conductive nature (n = 2). Of the 15 patients without intracranial injury, 8 underwent audiologic testing: 6 (75%) showed hearing loss and 2 (25%) had normal hearing. There was no difference in mean PTA (83vs 76 dB) or SDS (50%vs 54%) with or without traumatic brain injury (P = .74, .85). Additionally, there was no difference in rate of follow up. No specific pattern of hearing loss correlated with intracranial injuries.
Other Neurologic Injuries
Spinal injuries were present in 4 patients (11%; 3 cervical, 1 thoracic). One had normal hearing, one anacusis, and 2 were lost to follow up. Cranial neuropathies other than VII/VIII were present in 3 patients. Patient 10 had CN IX, X, and XI palsies and a MHL, Patient 32 had CN X and XII palsies and normal hearing, and Patient 35 had CN III and VI palsies and anacusis. No discernable pattern of hearing loss was associated with these injuries.
Cerebrospinal Fluid (CSF) Fistulae
CSF leak occurred in 6 patients (17.1%). Lumbar drain was placed for 3, with one failure requiring frontoparietal craniotomy. One (Patient 1) had a GSW exit wound leaking CSF from the wound treated by oversewing the laceration. External ventriculostomy drain was placed in one patient (Patient 35) who continued to leak, developed fulminant meningitis, and underwent subtotal petrosectomy and middle cranial fossa repair. One (Patient 39) had dural tears with CSF leak repaired at the time of emergent decompressive craniotomy. Of all those with CSF fistulae, one demonstrated anacusis, one MHL and 4 were lost to follow up.
Vascular Injuries
Vascular injuries were common and present in 14 patients (40%). Intracranial carotid injuries occurred in 5 patients (14.3%), extracranial carotid injuries in 4 (11.4%), with carotid-cavernous fistulae in 2 patients (5.7%) and venous injuries in 5 patients (14.3%). Venous injuries occurred most commonly at the sigmoid sinus (n = 4), all involving the sigmoid-transverse junction, the most lateral location along the temporal bone. The internal jugular vein was disrupted in 2 patients (5.7%). Other major vessels injured included the internal maxillary artery (n = 3), vertebral artery (n = 2), facial artery, temporal artery, iliac artery, and inferior vena cava. Of those with vascular injuries, 4 demonstrated SNHL (all anacusis), 3 MHL, 1 CHL, and 1 normal hearing. Five patients were lost to follow up and/or no audiogram was performed. Of those with vascular injuries, mean PTA was 83 ± 39 dB (median 84 dB), mean bone line average was 55 ± 28 dB (median 75 dB), and mean word recognition score was 45 ± 50% (median 31%). There was no significant difference in these parameters between those with or without vascular injuries (P = .84, .21, .55, respectively).
Loss to Follow Up
Sixteen patients (45.7%) were not evaluated after hospital discharge due to: no show to scheduled appointment (n = 5), failure to schedule appointment (n = 1), insurance out of network (n = 2), or follow up not recommended (n = 8).
Discussion
Injury severity depends on wound site, range (distance of the firearm from the wound), as well as the kinetic energy, material, and caliber of the bullet. The petrous temporal bone is the densest bone of the body requiring an estimated 1875 pounds of lateral force to fracture. 11 The bullet’s velocity is the main driver of its kinetic energy (KE = ½ mv 2 ) to achieve this force. 12 The vast majority of temporal bone ballistic injuries do not fracture the otic capsule bone, which houses the delicate labyrinthine structures. However, due to acoustic trauma and labyrinthine concussion from a higher primary blast wave associated with GSW, our series demonstrates that sensorineural hearing loss is common even with a spared otic capsule. Labyrinthine concussion describes sensorineural hearing loss with or without vestibulopathy after head trauma without fracture of the bony labyrinthine capsule. Labyrinthine concussion affecting only hearing may be termed cochlear concussion. Based on animal experiments, the proposed mechanism is high-intensity pressure waves disrupting the organ of Corti structures, including damage to the hair cells and microvascular circulation with resulting spiral ganglion nerve fiber degeneration.13-15 High frequencies, centered on 4000 Hz, are the most affected, as in acoustic trauma. Progressive partial auditory threshold recovery following labyrinthine concussion may occur over the first few weeks after head trauma. 13 It is not known if patients in our cohort experienced any spontaneous recovery as none underwent serial audiometry.
In the present series, the majority (70%) of temporal bone ballistic injuries cause some degree of sensorineural hearing loss, with half of those demonstrating a mixed loss. Five patients demonstrated anacusis, all with immediate, complete facial nerve paralysis. No patients with normal facial function demonstrated audiometrically-documented anacusis. However, conclusions regarding this correlation should be approached cautiously. Many patients were lost to follow up with an audiogram obtained in 48.6% of patients. As those with an immediate, complete facial paralysis were more likely to proceed to surgery for facial nerve decompression, a greater attempt was made to obtain an inpatient urgent audiogram for preoperative baseline testing. This differential effort for formalized testing likely introduces bias into the audiometric outcomes. Concomitant injuries including other cranial nerves, intracranial, spinal, and vascular injuries, were not associated with any particular hearing loss pattern, or anacusis.
Prior published series of temporal bone ballistic trauma offer limited audiologic details. In a large series of 98 patients treated in Brazil for facial paralysis after GSW to temporal bone, no audiologic results were mentioned. 2 Likewise, Yetsier and Kahramanyol did not discuss the audiologic outcomes of their 5 patients, only mentioning that one had anacusis. 3 In those who reported audiologic results, approximately half of patients underwent testing, consistent with our series. Habercamp et al described results in 7/12 patients, 6 of which had anacusis and 1 with CHL, unreported degree. 4 Hooper et al mentioned audiologic results in 6/8 patients: 3 with profound SNHL (2/3 anacusis), 1 moderate MHL, 1 mild CHL, 1 mild SNHL bilaterally. 5 Sabin et al reported audiologic results in 14/28 patients, 12 of which had sensorineural or mixed hearing loss. 6 Shindo et al discussed audiologic results in 22 of 43 patients, 13 with profound SNHL, 5 with severe MHL, 2 with high-frequency SNHL and 2 with moderate MHL. 7 Duncan et al presented audiologic results in 14/22 patients, mentioning + or ++ severity of CHL, MHL, or SNHL. 8 No conclusions regarding the average severity of hearing loss in these patients were reached. Consistent with our series, most patients who were tested had some degree of SNHL, with or without a concomitant conductive component.
Auditory rehabilitation was recommended for those with SNHL or MHL after audiometry. Due to the severity of loss and low speech discrimination scores, most were recommended for a CROS (Contralateral Routing of Signals) aid rather than a conventional hearing aid. Most patients who undergo cochlear implantation after temporal bone fracture demonstrate audiologic and functional improvement. 16 None in our cohort proceeded to osseointegrated hearing implant or cochlear implantation, mostly due to insurance coverage limitations for those with state-sponsored public insurance. However, should cochlear implantation be undertaken in this population, special consideration must be taken to ensure a patent cochlea is present.
Limitations
This study is limited by its retrospective nature and small sample size due to the relative rarity of ballistic trauma to the temporal bone. Additionally, many patients (45.7%) were lost to follow up after hospital discharge and did not undergo audiologic testing, limiting the ability to draw conclusions regarding those patients. It was suspected that admission to an acute rehabilitation facility after hospital discharge may be a barrier to follow up; however, it was equally likely for patients discharged to an acute rehabilitation facility to follow up as those who were not (approximately 50%). Therefore, acute rehabilitation admission did not appear to be a barrier to outpatient follow up care. For those patients who underwent urgent surgery, including facial nerve decompression, an attempt was made to obtain an inpatient audiogram for a preoperative baseline hearing assessment. Considering the high rate of loss to follow up, this likely introduced bias in documenting audiologic outcomes.
Insurance coverage limited care in some patients. Two patients were not able to follow up at our institution due to insurance-network constraints, so there were no audiologic results obtained for these patients. In addition, public health insurance plans for indigent populations are managed on the state level and are subject to coverage limitations that vary by state. In Louisiana, surgical auditory rehabilitation, including osseointegrated hearing implants and cochlear implants, is not covered by state-sponsored public insurance (Medicaid plans) for financially disadvantaged adults. The vast majority of these patients were covered by one of these plans, limiting both the care of these patients and the ability to draw conclusions regarding the audiologic outcomes of these devices in this patient population. These limitations, based on payer source as a proxy for income, likely generate health care disparities, an important area for future research.
Conclusions
Sensorineural hearing loss occurs at a high rate following ballistic trauma to the temporal bone, even though most fractures spare the otic capsule. Conductive hearing losses due to ossicular discontinuity or serous otitis media following Eustachian tube injury can be addressed surgically. While mixed losses can be considered for surgical intervention to correct the conductive component, in the present series, the underlying sensorineural loss was too pronounced to allow meaningful benefit. Therefore, no surgical intervention was performed in those with mixed hearing loss. Altered mental status due to concomitant traumatic brain injury and social issues including interactions with the criminal justice system complicate management and likely contribute to the high rates of loss to follow up in this patient population.
Footnotes
Authors’ Note
This manuscript was presented at the AAO-HNSF 2022 Annual Meeting, Philadelphia, PA, September 11-14, 2022.
Author Contributions
Anne K. Maxwell: Conceptualization, data acquisition/analysis/interpretation, drafted article, approved final version; Jacob B. Kahane: data interpretation, revised article, approved final version; Terrence P. Murphy: data interpretation, revised article, approved final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.