
Abstract
Objective:
Survival of laryngeal cancer is decreasing; thus, optimal treatment selection is paramount. Specifically, T3 disease survival appears similar with surgical or non-surgical management; however, the implications of vocal cord fixation on treatment selection and survival are unknown. This study seeks to determine if surgical treatment of patients with T3M0 laryngeal cancer with vocal cord fixation is associated with superior survival compared to non-surgical treatment.
Methods:
The National Cancer Database (NCDB) was queried for all T3M0 laryngeal carcinoma cases from 2004 to 2015, whose treatment included surgery or radiation therapy. Cases were stratified by cord fixation status and overall survival was compared using multivariable methods based on surgical versus non-surgical management.
Results:
Non-surgical management was more common, regardless of cord fixation status (84% in fixed and 79% in mobile). Cord fixation itself did not influence survival; however, surgical management had a significant survival benefit in the fixed cohort (HR = 0.843; 95% CI: 0.738, 0.962).
Conclusion:
In this large observational cohort study of T3M0 laryngeal cancer, those with fixed cords had superior survival when managed surgically.
Introduction
Although the mortality rate for most cancers has decreased over the last few decades, multiple population-level studies have demonstrated a concerning increase in mortality among patients with laryngeal cancer.1-3 This increase in mortality has coincided with an increased use of non-surgical management following the landmark Veteran Affairs (VA) trial which demonstrated similar survival between surgical and non-surgical management in advanced laryngeal cancer.1,4 This begs the question whether a subgroup of these patients are better managed surgically. We now know that tumors with gross cartilage invasion or extra-laryngeal extension (T4a) are less responsive to chemoradiation and thus are preferentially treated with surgery. 5 However, T3 disease encompasses a more heterogeneous tumor profile, including those with fixed vocal cords. The etiology of this cord fixation includes cricoarytenoid joint invasion, which may result in reduced radiosensitivity, similar to cartilage invasion in T4a disease. 5 Further, studies indicate that cancers with impaired cord mobility portend a worse prognosis.6-9 Despite these findings, while guidelines dictate the necessity of evaluating laryngeal function and using this to inform treatment decision, the presence of vocal cord fixation has not explicitly impacted treatment guidelines for T3 laryngeal cancer and allows treatment to be surgical or non-surgical.
There have been no studies to our knowledge that establish a survival difference for surgical versus nonsurgical management in specific T3M0 laryngeal cancer, stratified by pretreatment vocal cord fixation status. We hypothesize that surgical management of T3M0 disease with pre-treatment cord fixation leads to improved overall survival compared to nonsurgical management of these patients. This finding could be used to better select patients requiring surgery to maximize survival and those able to avoid the morbidity of surgery.
Materials and Methods
Data Source and Patient Cohort
We performed a retrospective cohort study using the National Cancer Database (NCDB). A nationally recognized database sponsored by the American College of Surgeons and the American Cancer Society, the NCDB is a clinical oncology database that collects hospital registry data from more than 1500 Commission on Cancer (CoC)-accredited facilities. It has been an invaluable resource owing to its reported representation of more than 70% of newly diagnosed cancer cases nationwide and more than 34 million historical records. 10
The database was queried for all T3M0 laryngeal carcinoma cases from the years 2004 to 2015. This date range was chosen because staging information was not reliably present prior to 2004 and vital status was not available in 2016. Specifically, inclusion criteria consisted of age older than 18, confirmed histologic diagnosis of squamous cell carcinoma (ICD-O-3: 8052, 8070-8076, 8078, and 8083) of the larynx, clinically staged T3, including all laryngeal subsites (ICD-O-3: C32.1, C32.2, C32.8, C32.9, and C32.0) and all nodal staging, with no evidence of distant metastasis. Regarding staging, AJCC sixth edition was used for 2004 TO 2009 and AJCC seventh edition was used for 2010 to 2015. There were no significant changes in TNM or clinical group staging made between the sixth and seventh editions for laryngeal cancer. Only clinical staging was included because this is the staging information available to clinicians at the decision point important to our research question, namely the decision to pursue surgical versus nonsurgical primary management. Furthermore, including pathologic stage introduces information and misclassification bias differential on our exposure (ie, surgical and nonsurgical patients).
The NCDB captures a patient’s first course of treatment defined as all methods of treatment recorded in the treatment plan and administered to the patient before disease progression or recurrence. The typical primary treatment modalities for laryngeal cancer are either primary radiation therapy (with or without chemotherapy) or primary surgery (with or without adjuvant chemoradiotherapy). Therefore, patients were excluded from analysis if they had prior malignancy, no documented treatment, treatment with chemotherapy alone, or treatment with radiation before surgery (as this is not a standard primary treatment modality) so as to not muddle survival results.
These cases were then stratified into 2 cohorts based on pre-treatment vocal cord fixation status: fixed and mobile, as documented in the NCDB. These cohorts were then compared by treatment type: surgical (+/− adjuvant therapy) and non-surgical (radiation +/− chemotherapy). The NCDB does not allow the analysis of subsequent disease progression/recurrence or salvage treatments. The database also does not allow analysis of functional status including gastrostomy tube or tracheostomy dependence.
Variables
Variables incorporated into the analysis included patient age, sex, race/ethnicity, insurance status, median income quartile (derived at the population level), Charlson comorbidity score (0, 1, and 2+, with a higher score indicating more comorbidities), and treatment facility type. Additionally, cancer-specific characteristics analyzed included laryngeal subsite, nodal stage, vocal cord fixation status (Collaborative Staging, CS, extension code 400), primary treatment modality (radiation alone, chemoradiation, surgery alone, surgery + radiation, and surgery + chemoradiation), and surgery type (total laryngectomy: Surveillance, Epidemiology & End Results (SEER) Site-Specific Surgery of Primary Site Codes 40-42 and 50, partial laryngectomy: SEER Site-Specific Surgery of Primary Site Codes 30-33, or other: SEER Site-Specific Surgery of Primary Site Codes 20, 22-25, 28). These local excision codes were included and grouped as “other” because they were all ultimately considered oncologic surgeries by the NCDB, and exclusion of these codes would bias comparisons to the non-surgical cohort (which includes tumors that may have been otherwise treated with similar surgeries).
Outcome
The primary outcome measure analyzed was 5-year overall survival. Of note, the NCDB does not allow the analysis of disease-specific survival or recurrence because the cause of death and recurrence were not recorded.
Statistical Analysis
The descriptive analysis compared covariates across races and was tested by 2-sided Pearson chi-square tests for categorical variables. For continuous variables, means and standard deviations (SD) were calculated, and t-tests were conducted for normally distributed variables.
We calculated overall survival as the time from diagnosis to either the date of death due to any cause or censoring due to lost to follow-up or 5 years of follow-up. Kaplan-Meier all-cause survival plots were constructed, and log-rank P-values were calculated. Hazard ratios (HR) were estimated by Cox proportional hazards regressions. An alpha of .05 was used for all statistical testing and confidence interval calculations. The proportional hazards assumption was satisfied. The data on radiation dose is missing in most patients, and there is concern for reliability in those with available data. Therefore, we did not include it as a criterion for our primary analysis. However, we performed a sensitivity analysis excluding patients who received less than 45 Gy dosing to address the concern that patients treated with palliative doses could have been included and limit the generalizability of the survival results.
Statistics including the survival analyses were conducted with R 3.2.0 using rms, survival, and survminer packages (R Foundation for Statistical Computing, Vienna, Austria).
This research study was presented to the Saint Louis University Institutional Review Board and it was determined that the study did not necessitate approval.
Results
Patient Demographics
The search resulted in 10 216 patients after applying the inclusion and exclusion criteria (Table 1). Non-surgical management was the most common treatment modality, regardless of pre-treatment cord fixation status (84% of fixed cord cohort managed non-surgically vs 79% of mobile cohort).
Demographics Overall and Stratified by Pre-Treatment Vocal Cord Fixation Status.
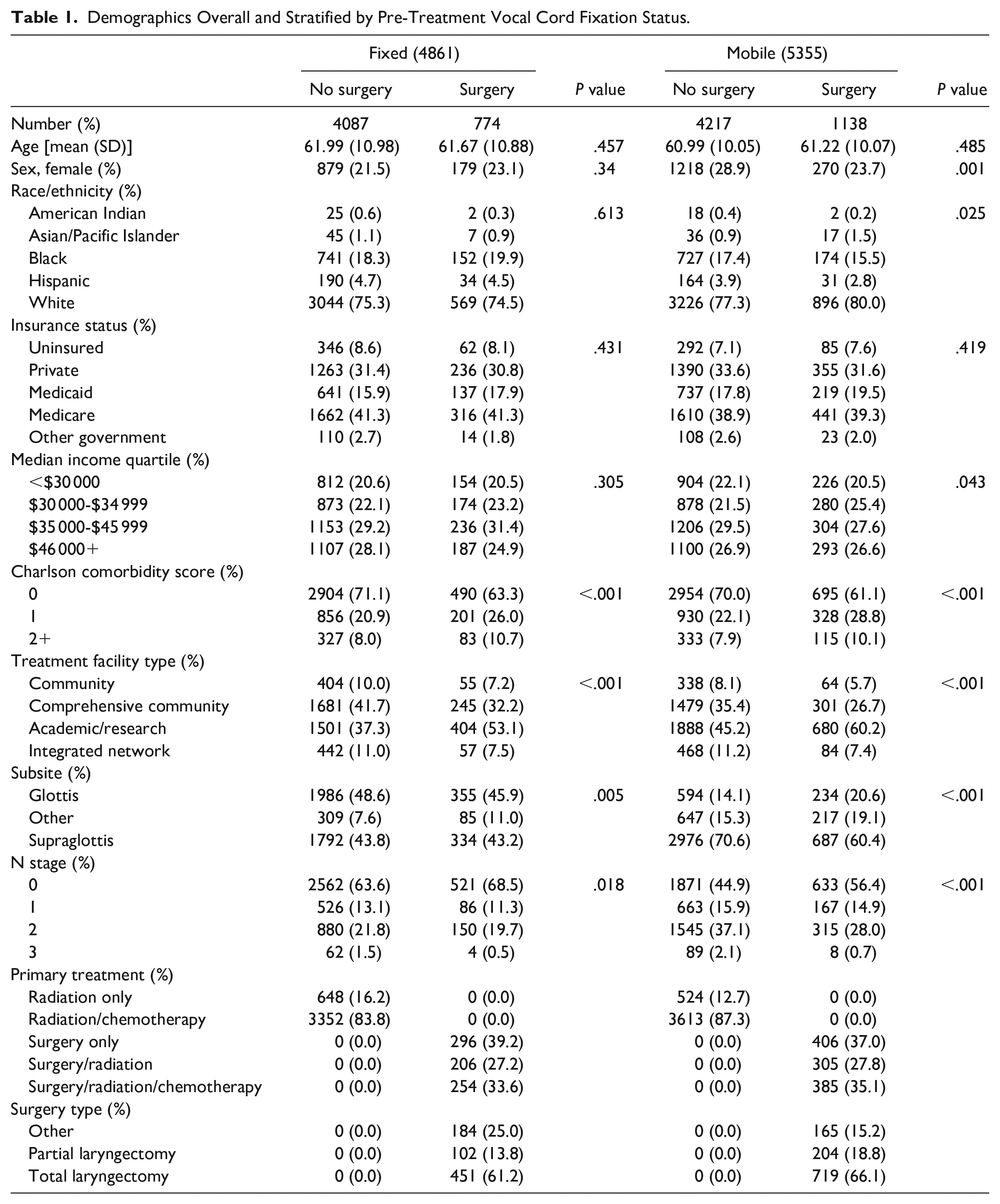
There were statistically significant differences in sex, race, and median income quartile between those undergoing surgical versus non-surgical management in the mobile cord cohort only.
Charlson comorbidity scores and treatment facility type were significantly different between those undergoing surgical versus non-surgical management in both patient cohorts. For both patient cohorts, non-surgical management was generally more common in those with lower comorbidity scores, and surgical management relatively increased as comorbidity score increased. In the fixed cohort, 85.6% of patients with a comorbidity score of 0 were managed non-surgically, compared to 79.8% of patients with a comorbidity score of 2+. Similarly, in the mobile cohort, 81% of patients with a comorbidity score of 0 were managed non-surgically, compared to 74.3% of patients with a comorbidity score of 2+. Surgical management was more common among both patient cohorts in academic/research institutions than others (in the fixed cohort 53.1% of patients managed surgically occurred in academic institutions, and in the mobile cohort 60.2% of patients managed surgically occurred in academic institutions).
Tumor Characteristics and Primary Treatment Modalities
Among the fixed vocal cord cohort, the glottic subsite was relatively more common (48.1% glottic, 43.7% supraglottic, and 8.1% other) and more likely to be managed non-surgically (84.8% of glottic cancers among the fixed cord cohort managed non-surgically). Among the mobile vocal cord cohort, the supraglottic subsite was relatively more common (67.8% supraglottic, 15.5% glottic, and 16.1% other) and also more likely to be managed non-surgically (81.2% of supraglottic cancers among the mobile cord cohort managed non-surgically; Table 1).
There were significant differences in nodal stage managed surgically versus non-surgically in both patient cohorts, with higher nodal stage generally being managed more non-surgically (in fixed cohort: 36.4% of patients treated non-surgically had nodal disease vs 31.5% treated surgically; in mobile cohort: 55.1% of patients treated non-surgically had nodal disease vs 43.6% treated surgically).
Most patients in both the fixed (69.0%) and mobile (67.5%) cohorts underwent chemoradiotherapy as the primary treatment modality.
Finally, when surgical management was pursued, both total laryngectomy (66.1% vs 61.2%) and partial laryngectomy (18.8% vs 13.8%) were performed slightly more often in the mobile cord cohort versus fixed cord cohort.
Survival Analysis
In univariable analysis of all T3 laryngeal cancers based on vocal cord fixation status, regardless of treatment modality used, the 5-year overall survival was similar for both the fixed cord cohort and the mobile cord cohort (Figure 1).
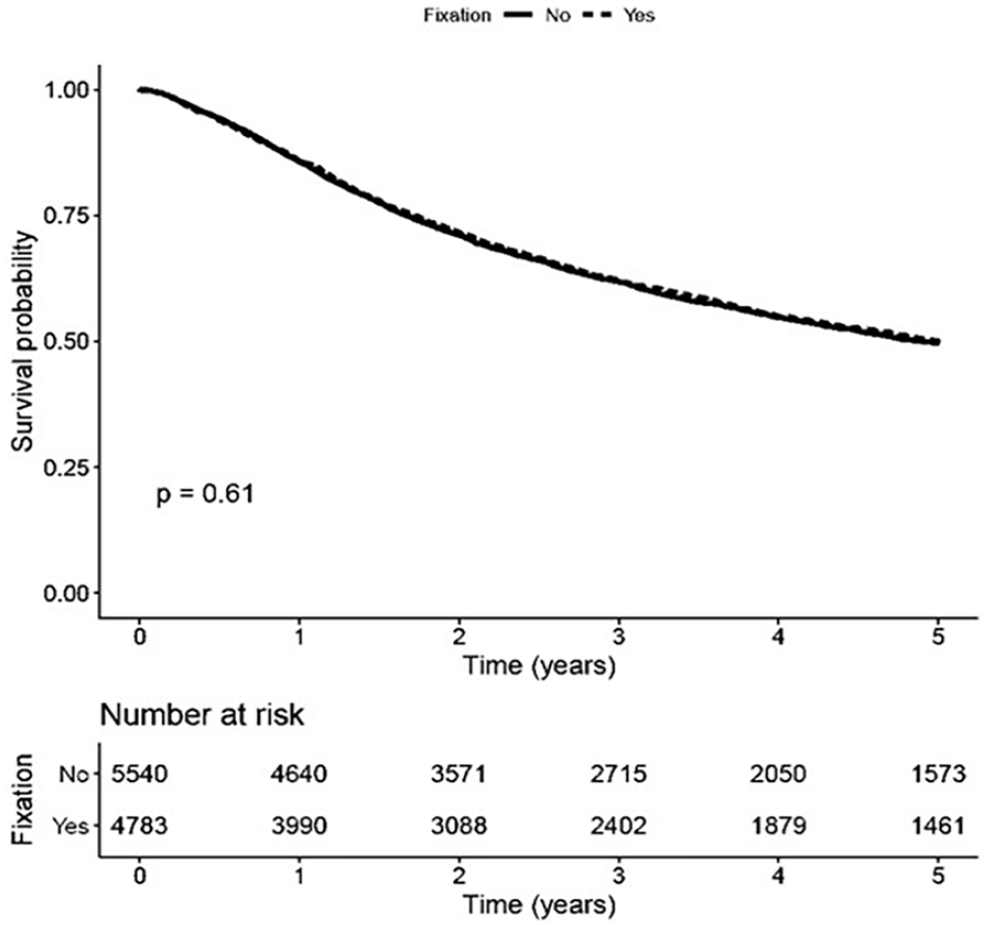
Survival analysis for all T3 cancers regardless of treatment modality, based on presence or absence of vocal cord fixation.
Among the fixed cohort alone, surgical management was associated with better overall survival (Figure 2). However, the benefit of surgical management was also present in the mobile cohort (Figure 3).
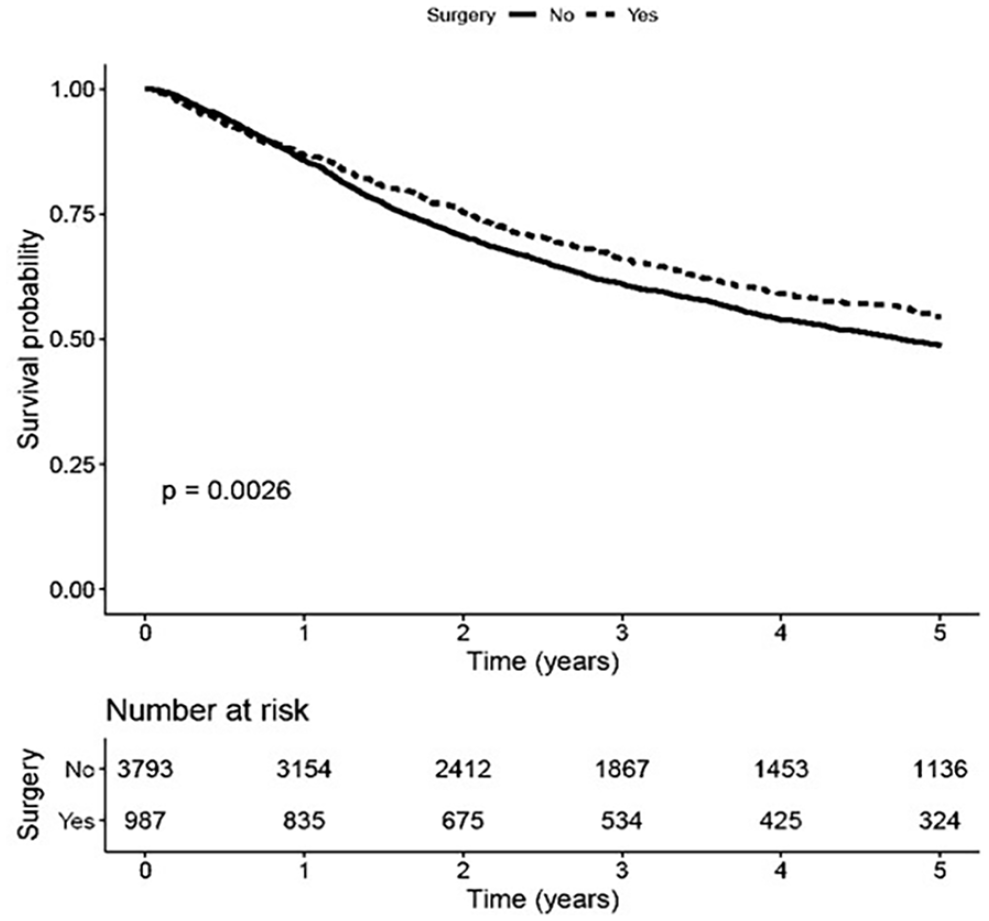
Survival analysis of T3 cancers with vocal cord fixation, based on treatment modality.
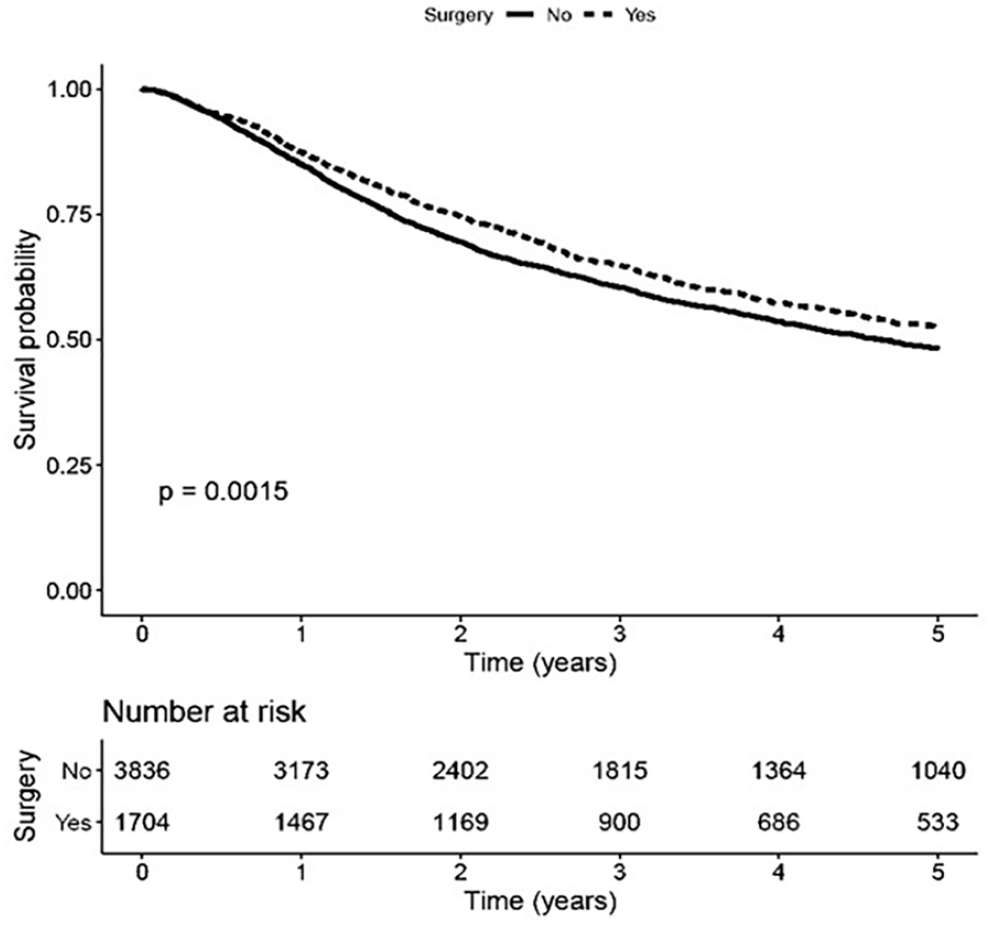
Survival analysis of T3 cancers with mobile vocal cords based on treatment modality.
When performing multivariable overall survival analyses, surgical treatment maintained a significant survival benefit compared to non-surgical treatment in the fixed cord cohort (HR = 0.843; 95% CI: 0.738, 0.962), but not the mobile cord cohort (HR 0.897; 95% CI 0.802, 1.003); Table 2). A sensitivity analysis excluding patients who received <45 Gy radiation dosing produced similar survival results (Table 3).
Multivariate Overall Survival Analyses Stratified by Pre-Treatment Vocal Cord Fixation Status.
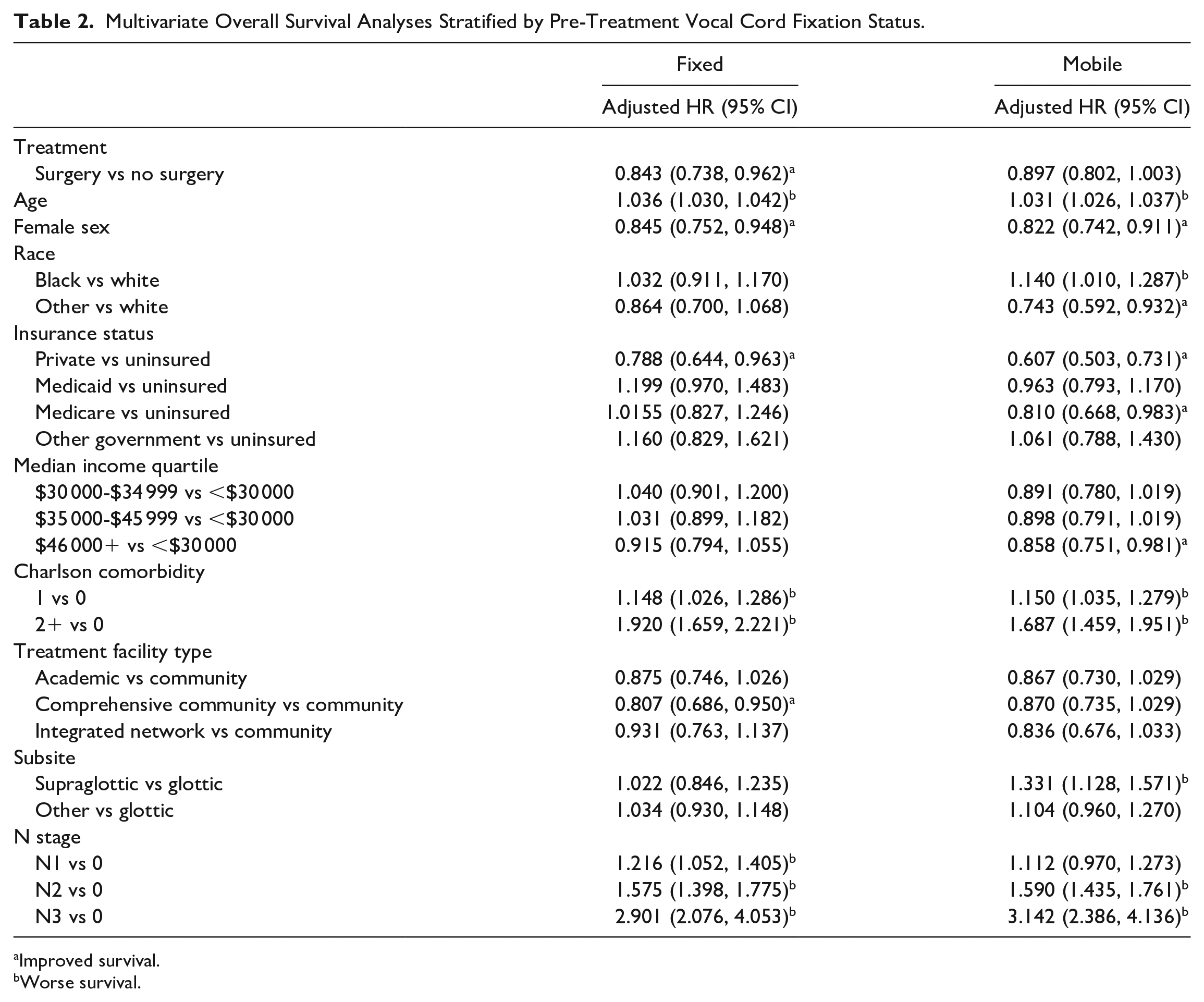
Improved survival.
Worse survival.
Multivariate Overall Survival Analyses Stratified by Pre-Treatment Vocal Cord Fixation Status, Excluding Patients Receiving <45Gy.
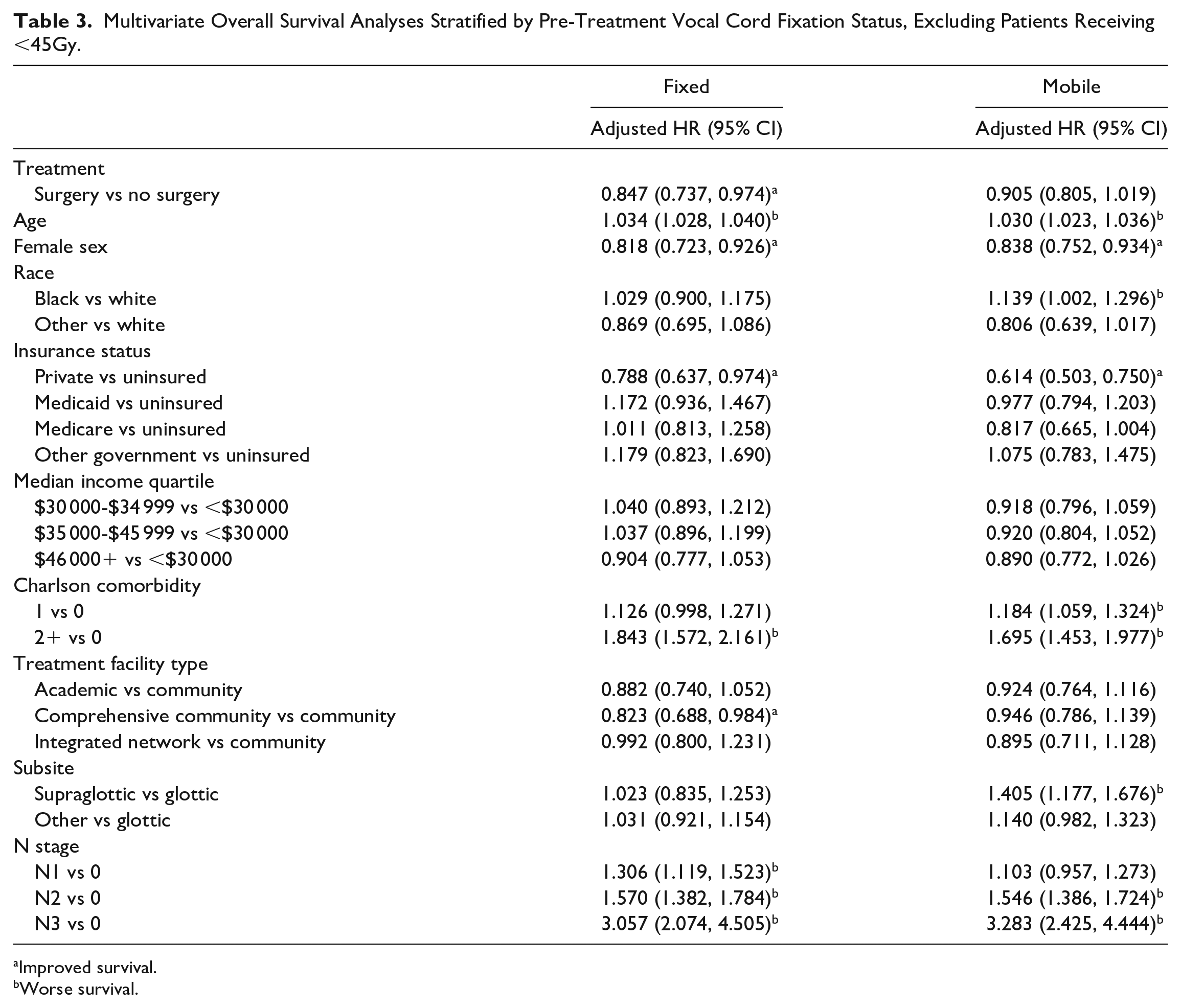
Improved survival.
Worse survival.
Laryngeal subsite was not associated with a difference in overall survival, except for “supraglottic” in the mobile cord cohort, which was associated with a worse overall survival (HR = 1.331; 95% CI: 1.128, 1.571; Table 2).
Discussion
Existing research has not reliably determined an optimal treatment modality for T3M0 laryngeal cancer, and treatment choice often entails difficult conversations between patient and physician. Our results indicate a significant improvement in overall survival associated with surgical management in this population, specifically among the fixed vocal cord cohort. Furthermore, this survival benefit has a large effect size (HR = 0.843; 95% CI: 0.738, 0.962) that the authors believe is clinically significant. However, surgical management was used in a minority of patients in this cohort and at a similar rate for those with mobile cords, which reflects the preferential use of laryngeal preservation treatment modalities.1,11
Although prior randomized trials have shown similar survival between surgical and non-surgical management in advanced laryngeal cancer, subsequent real-world observational data has demonstrated more heterogenous results. 5 The reasons for this discordance may be that the randomized data is not generalizable to the real-world setting, the randomized data is not being applied appropriately, or the observational data is biased.
Indeed, the landmark VA study demonstrated similar 2-year survival outcomes between surgical versus non-surgical management (68% for both) in stage III/IV laryngeal cancer. 4 However, this study's inclusion criteria do not reflect current staging classifications, making application to the T3 cancer population difficult.4,12 Later retrospective studies of the NCDB and SEER database also demonstrated similar survival rates among stage III laryngeal cancer patients undergoing surgical versus non-surgical management.11,13 However, Megwalu et al 14 concluded that surgical therapy leads to better survival outcomes in stage III/IV laryngeal cancer, even after adjustment for stage and year of diagnosis. Subsequent studies specific to T3 disease concluded similar survival outcomes between the 2 modalities.15,16 Hoffman et al 1 specifically analyzed the overall survival of T3N0M0 laryngeal cancer treated with surgery and radiation (65.2%) versus chemoradiation (59.3%), which showed a survival benefit from surgery that was not statistically significant (P = .067). Later, an analysis of patients with T3/T4a disease in the Alberta Cancer Registry found that surgical management had statistically superior survival compared to non-surgical management in both T3 and T4a cohorts with large effect sizes (HR = 3.1 and 2.6 for radiation or chemoradiation compared to surgery with adjuvant therapy). 12 Finally, Al-Gilani et al 17 found a statistically significant survival advantage with surgical management of T3M0 glottic cancer compared to non-surgical management (HR = 0.68; 95 CI: 0.49, 0.94).
The heterogeneity of these survival outcomes among various studies reflects the different patient populations analyzed with a wide range of staging criteria, the difficulties applying a regimented treatment protocol to this subset of patients, and the limitations inherent to retrospective reviews. Therefore, the primary treatment approach can be very challenging and highly tailored to the patient at hand. 18 Furthermore, it is paramount to make the ideal management choice correctly early on in treatment, as salvage surgery is more challenging and associated with worse outcomes. 19
Ultimately, treatment decision depends on an accurate assessment of pre-treatment laryngeal function with the understanding that T3 patients with a nonfunctional larynx or evidence of cartilage invasion are likely poor candidates for a larynx preservation approach. 18 Vocal cord fixation is an easily identifiable physical exam finding, implies impaired laryngeal function, and has shown evidence of portending worse prognosis. Despite this fact, none of the aforementioned studies specifically analyze pretreatment vocal cord fixation status and its relation to treatment selection and survival outcomes.
Indeed, although the landmark VA trial demonstrated similar survival between surgical and non-surgical management in advanced laryngeal cancer, salvage laryngectomy was ultimately required in 35% of patients and was required more often in those with fixed vocal cords and in those with gross cartilage invasion. 4 Staton et al 20 demonstrated that vocal cord fixation was the strongest predictor of poor functional outcome in advanced laryngeal cancer patients receiving chemoradiation therapy. Failure for vocal cord mobility to return after treatment portends a high likelihood of persistent disease.6,21
Based on the above evidence, we hypothesized that T3M0 laryngeal cancer with vocal cord fixation has improved survival when treated surgically. Our results support this hypothesis. However, these results should be interpreted cautiously given the retrospective nature of this study. We also assessed the survival benefit of surgery in the mobile vocal cord cohort to better understand if the observed association with improved survival and surgical treatment was specific to those with fixed vocal cords. While the adjusted hazard ratio for surgery in the mobile cohort was not statistically significantly different from the null hypothesis, the effect size was still similar to the fixed vocal cord cohort. In both cases, the overall survival benefit associated with surgery could be due to unaccounted confounding variables such as incomplete or lower dose chemo/radiation therapy (although we attempted to control for this with our additional sensitivity analysis), non-standardized treatment, or poor treatment compliance.
There were significant differences in treatment based on Charlson comorbidity score, treatment facility, laryngeal subsite, and nodal stage, each of which could contribute to the improved survival benefit seen with surgical management. However, the survival differences persisted after controlling for these. Interestingly, while non-surgical management was overall more common in both cohorts, surgical management relatively increased as comorbidity score increased, which is evidence against the argument that surgical management is associated with improved survival due to the selection of healthier patients.
Regarding tumor-specific factors, the supraglottic subsite was seen more commonly than the glottic subsite (5789 patients, 56.7% vs 3169 patients, 31.0%, respectively). Glottic subsite was relatively more common in the fixed cord cohort, likely because glottic tumors are more likely to cause vocal cord fixation by nature of their location. However, non-surgical management was most commonly utilized for all laryngeal subsites.
Ultimately, further research is needed to elucidate which patients with T3M0 disease are treated optimally with surgical versus non-surgical management, as the answer to this question has implications on survival outcomes and quality of life. Indeed, the likelihood of achieving a functional larynx must be considered before choosing non-surgical therapy over surgical management in these patients, as organ preservation oftentimes does not correlate with preservation of function. Timme et al 22 found a 2-year laryngoesophageal dysfunction-free survival of only 40% in patients with T3 lesions and the landmark VA trial demonstrated a larynx preservation rate of only 66% in the chemotherapy group. 4 An added benefit of surgical management is that it both serves therapeutic and diagnostic purposes, as patients may be subsequently more accurately staged pathologically and receive stage-appropriate adjuvant treatment.
This study has many significant limitations, largely related to the database and the nature of a retrospective review. For example, there have been reports that there is less than 90% agreement between T stage reporting in the NCDB versus what is recorded in the original hospital chart. 1 Additionally, the accuracy of vocal cord fixation status as recorded in the NCDB is unknown. Vocal cord fixation is described as immobility of the arytenoids noted on endoscopy, vocal cord paralysis, or deviation of the larynx to the fixed side (according to CS data extension codes). It is unclear how reliable the clinician is at documenting this or how reliable the coding is. However, there is no better large data source for this research question. Furthermore, this study analyzes a broad time range among multiple hospitals where surgical and non-surgical management could involve treatment heterogeneity, including partial laryngectomy or local tumor excision, non-standardized or sub-efficacious radiation dosing and incomplete treatment, interrupted treatment, or delay in treatment initiation. This database also does not allow measurement of disease-specific survival and does not investigate quality-of-life outcomes or laryngoesophageal function outcomes. Future directions to investigate this research question may include prospective studies with a narrower focus on specific laryngeal subsites, specific nodal status, and standardized chemoradiation therapy dosing.
Conclusion
For T3M0 laryngeal cancer, the most common treatment modality used was chemoradiation therapy, regardless of vocal cord fixation status. This study demonstrates a significant survival benefit of surgical management compared to non-surgical management in patients with pre-treatment fixed vocal cords. Ultimately, further research is needed to elucidate which of these patients benefit more from surgical therapy and if vocal cord fixation status should be a factor in this decision-making process.
Footnotes
Author Contributions
Henry C. Ideker, MD: analysis, writing, revision; Ronald J. Walker, MD: analysis, revision
Angela Mazul, PhD, MPH: analysis, writing, revision; Sean T Massa, MD: design, conduct, analysis, writing, revision./
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.