
Abstract
Objective:
Robin sequence (RS) consists of micrognathia and glossoptosis that result in upper airway obstruction (UAO). In RS patients who undergo tracheostomy, long-term goals include natural decannulation (ND) without further surgical airway intervention. The objective of this study was to identify long-term trends in the rate and length of time to ND.
Methods:
Retrospective chart review on 144 patients with RS treated from 1995 to 2020 at a pediatric tertiary care center. Patients were grouped by year of tracheostomy. Demographic data, UAO management, postoperative care, complications, and time to decannulation were recorded.
Results:
Thirty-six patients met the inclusion criteria. Tracheostomy was performed at a median age of 45.5 days. 19 (53%) patients experienced ND at a median time of 66.1 months. ND rate was higher in non-syndromic patients (93% non-syndromic vs 27% syndromic; P < .0001) and during the first study period (1995-2006: 78%, 2007-2020: 28%; P = .003). Cox proportional-hazard regression demonstrated that white race [aHR 0.15 (0.03-0.8); P = .023] and higher birthweight [aHR 0.9 (0.8-0.98); P = .018] were associated with a higher likelihood of ND while a syndromic diagnosis had a negative association with ND [aHR 12.5 (3.3-50.0); P < .001].
Conclusions:
Our study documented that ND in patients with RS who underwent tracheostomy was significantly associated with ethnicity, birthweight, and syndromic status. The negative impact on successful ND was most observed in patients with syndromic associations. Additionally, ND rates are lower in the 2007 to 2020 subgroup. We suspect this is because alternative management techniques such as tongue lip adhesion and mandibular distraction osteogenesis became primary surgical treatment in severe RS upper airway obstruction at our institution starting in 2007.
Introduction
Robin Sequence (RS) is defined by micrognathia and glossoptosis resulting in upper airway obstruction (UAO) and is often associated with cleft palate.1,2 Treatment for UAO in patients with RS is often dependent upon the severity. While mild cases can be successfully managed with conservative measures such as prone positioning, nasopharyngeal airway, and nutritional support, patients with moderate and severe UAO may require surgical intervention. 3 Tongue-lip adhesion (TLA), mandibular distraction osteogenesis (MDO), and tracheostomy are different surgical strategies that successfully manage complex cases of UAO. 4
Tracheostomy can be required in RS patients unable to be managed conservatively or via other surgical techniques, as the procedure bypasses the UAO and can therefore serve as definitive airway management. However, long-term tracheostomy dependence is associated with higher levels of morbidity and mortality.5-7 Thus, management of RS typically has the goal of avoiding tracheostomy if able to provide adequate respiration, safe airway, and nutrition. Performing early decannulation is the goal if the procedure is deemed necessary, though it has been established that RS infants tend to need the tracheostomy in place for extended periods of time. Studies have shown that the time to natural decannulation (ND), defined as successful decannulation without the need for further surgical intervention, is between 28 and 37 months,5,8 and more than 73 months in patients with syndromic RS. 1
However, there remains a scarcity of information on factors associated with successful natural decannulation and how the rate and length of time to decannulation have changed over time. The trends over time are especially relevant with the shifts in surgical management to MDO or TLA in lieu of tracheostomy. The authors, therefore, set out to analyze a cohort of tracheotomized RS patients grouped by year of tracheostomy and syndromic diagnosis to identify factors associated with decannulation and trends in decannulation over time.
Methods
Following Children’s National Hospital Institutional Review Board (IRB) approval, a retrospective chart review was performed to identify patients with RS that underwent tracheostomy at a large free-standing pediatric hospital from 1995 to 2020. We included data from all patients who had at least 1 month of follow-up after tracheostomy. Patients with missing or incomplete medical records were excluded.
Demographic data gathered included age at admission, sex, race/ethnicity, and insurance status. Clinical characteristics, birth history (weight at admission, gestational age, birthweight, Apgar scores), hospital course, and associated syndromes, such as Stickler syndrome and Treacher-Collins syndrome, were also collected.
Length of hospital stay and time from tracheostomy to ND were recorded. Perioperative and postoperative complications including tracheitis, pneumonia, and wound breakdown were also obtained. Laboratory studies including maximum titratable bicarbonate (HCO3) and maximum carbon dioxide (CO2) levels were noted on arterial blood gas panels.
Descriptive summary statistics were presented as means with standard deviations (SD) or medians with interquartile ranges (IQR) for continuous variables, and frequencies with percentages for binary and categorical variables. Baseline demographic and preoperative hospital factors data were compared between syndromic and non-syndromic RS groups using unpaired t-test or non-parametric Mann-Whitney U test for continuous data and Chi-square and/or Fisher’s exact test (if any of the expected cell size <5) for categorical data. Normality assumptions were checked using a statistical test (eg, Shapiro Wilk test) as well as graphical methods (eg, histogram, q-q plot). A Chi-square test was used to compare the decannulation rates between groups. To examine the trend in weight gain between birthweight, admit weight, and discharge weight, a one-way ANOVA test was utilized.
Rates of surgical procedures to treat UAO varied throughout the study period. There was a clear shift toward performing more primary TLAs and MDOs following the arrival of a new surgeon at our institution in 2007. Therefore, patients were grouped by year of tracheostomy: 1995 to 2006 and 2007 to 2020. Using the Kaplan-Meier survival estimator, we estimated and compared the median time to decannulation between groups, and a log-rank test was used to assess the statistical significance.
Finally, a multivariable Cox proportional-hazard regression analysis was carried out to investigate if certain demographic factors were associated with a higher risk of not having natural decannulation, and the association was reported as adjusted hazard ratio (aHR) with corresponding 95% confidence intervals.
All statistical tests were two-sided and performed at the .05 level of significance. Statistical analysis was performed using R statistical software, version 4.0.3 (R Core Team, 2020).
Results
Of the 152 patients with RS, 8 were excluded due to poor or absent data, yielding 144 patients who met inclusion criteria (Figure 1). Thirty-six patients (25%) were managed with tracheostomy, and the remaining 108 were managed conservatively (n = 69, 47.9%) or with other surgical methods, such as TLA (n = 26, 18.1%) or MDO (n = 25, 17.4%). Of note, some patients in the 2007 to 2020 group had multiple procedures and are included multiple times in the data set. For example, 8 patients were unsuccessfully managed with TLA and/or MDO and required a subsequent tracheostomy; 7 of these patients were syndromic (87.5%). Seventy-three patients out of the entire cohort (50.1%) were syndromic with 22 patients (30.1%) requiring tracheostomy. Eight of the 18 syndromic patients (44.4%) before 2007 and 14 of the 55 syndromic patients (25.5%) after 2007 required tracheostomy. Of the 36 total patients with tracheostomy, 22 patients (61.1%) were syndromic and 14 (38.9%) were non-syndromic.
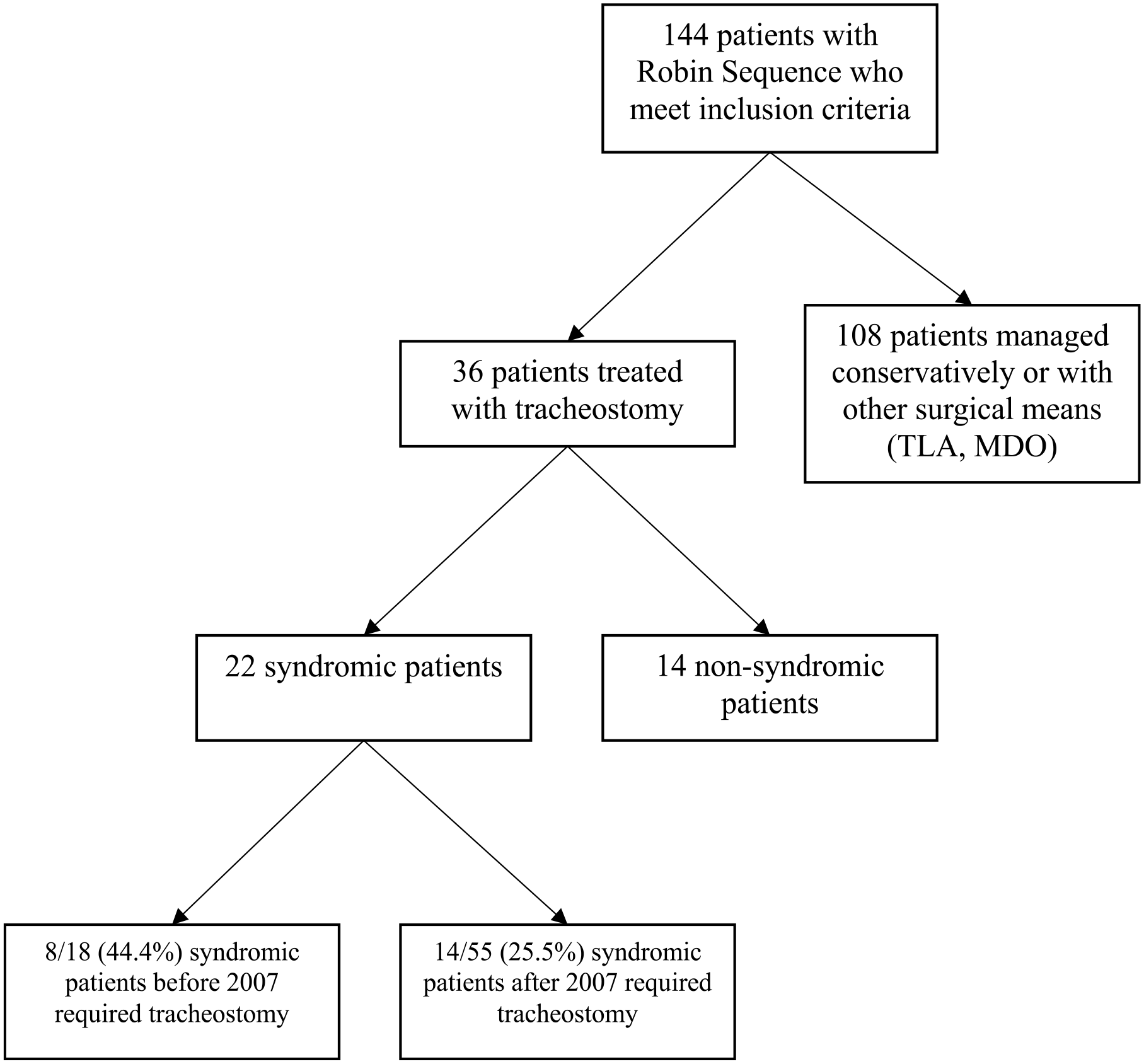
Of 144 RS patients who met inclusion criteria, 36 required tracheostomy, of whom 22 had syndromic associations. 44.4% of syndromic patients required tracheostomy before 2007, while 25.5% required tracheostomy after 2007.
Rates of primary surgical procedures to treat UAO varied throughout the study period. The rate of tracheostomy was significantly higher in the 1995 to 2006 group compared to the 2007 to 2020 group (50.0% vs 16.7%, P < .001). Conversely, the rates of both TLA and MDO were significantly lower in the 1995 to 2006 subgroup compared to the 2007 to 2020 subgroup (Table 1).
Comparison of Surgical Management Type by Time Period.
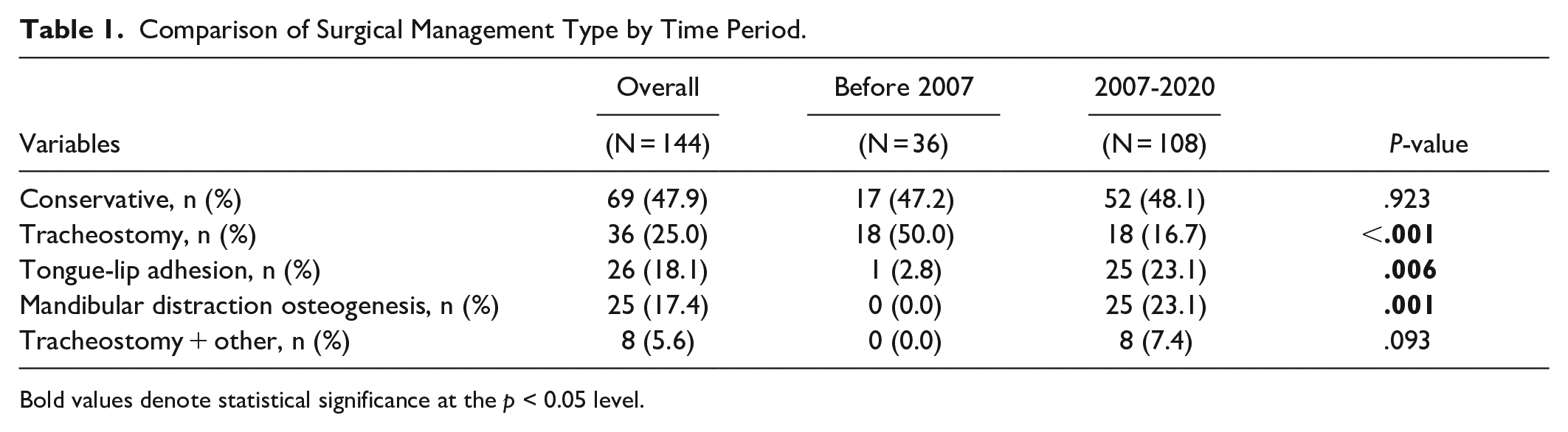
Bold values denote statistical significance at the p < 0.05 level.
Overall, 19 of 36 patients (52.8%) were naturally decannulated at a median time of 66.1 months (Figure 2). ND rate was 57.1% (16/28) in the patients treated only with tracheostomy and 37.5% (three-eighths) in patients with failed TLA or MDO and subsequent tracheostomy; this difference was not statistically significant (P = .326). ND rate was significantly higher from 1995 to 2006 than from 2007 to 2020 (77.8% vs 27.8%, P = .003). Time to ND from 1995 to 2006 was 21.3 months while median time to decannulation in the 2007 to 2020 group could not be determined as more than half of patients have not been decannulated. Cumulative ND probability was significantly higher in the 1995 to 2006 cohort compared to the 2007 to 2020 cohort (Log-Rank test P = .004). These findings are demonstrated in Figure 3.
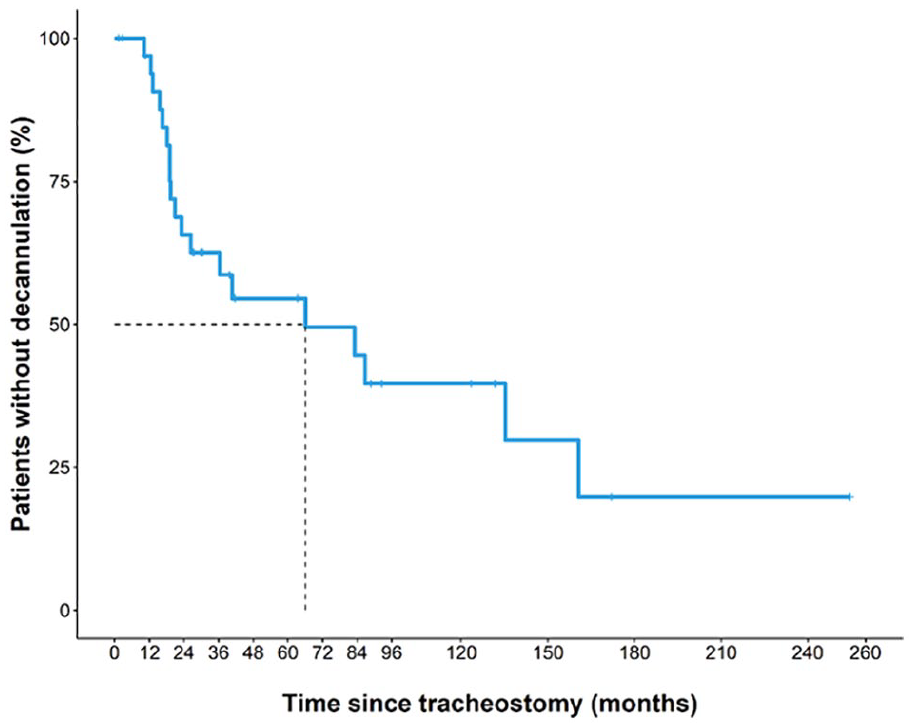
Nineteen of 36 patients (52.8%) were eventually decannulated and the median time to decannulation in all patients was 66.1 months.
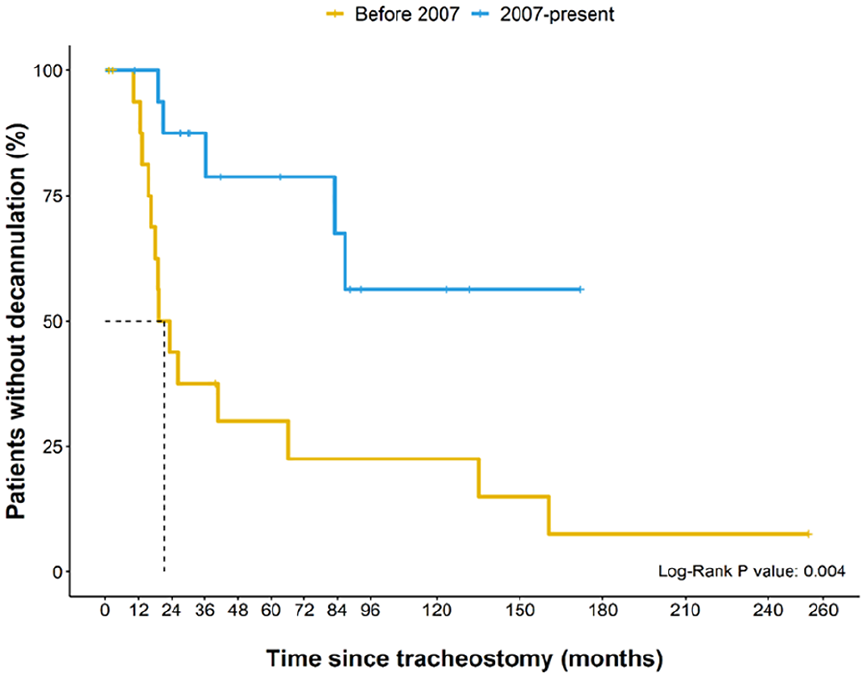
The median time to decannulation was 21.3 months in the 1995 to 2006 time period. The median time to decannulation from 2007-present could not be calculated since at least 50% of patients did not undergo decannulation. Cumulative decannulation probability was significantly higher in the 1995 to 2006 cohort compared to the 2007-present cohort (Log-Rank test P = .004).
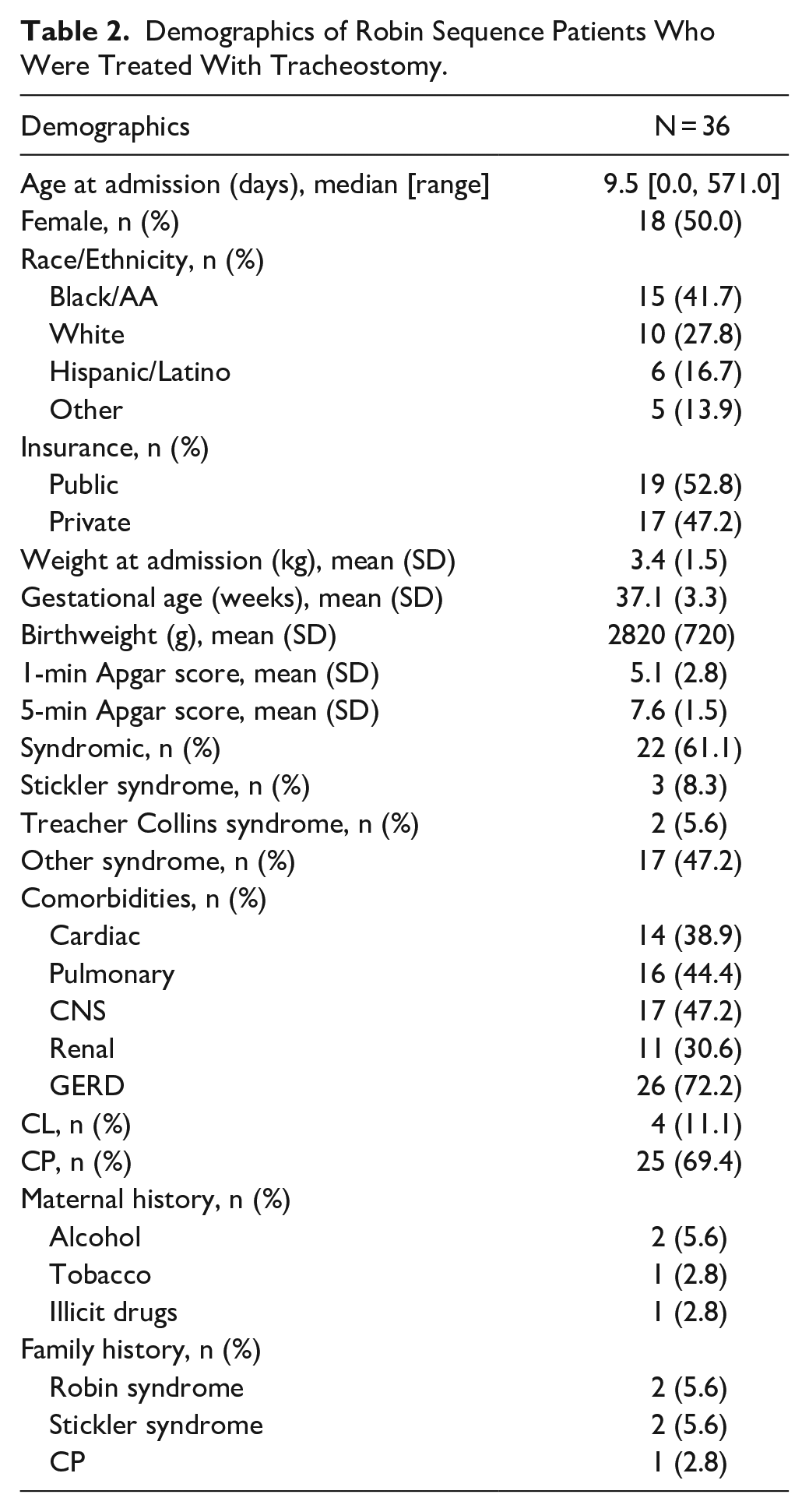
Most patients who underwent tracheostomy had a cleft palate (69.4%, n = 25) and syndromic association (61.1%, n = 22). Overall median age at admission and tracheostomy was 9.5 days [range, 0-571] and 45 days [range, 0-776], respectively. Patients with cleft palate had earlier median age at admission than patients without cleft palate (6 days [range, 0-15] vs 57 days [range, 8-66]; P = .037). Median age at tracheostomy did not significantly differ between the 2 groups (27 days [range, 14 and 73] vs 85 days [range, 36-106.5]; P = .164). When comparing syndromic patients to non-syndromic patients, neither median age at admission (12 days [range, 1.5-66.5] vs 8 days [range, 1.2-14]; P = .415) nor median age at tracheostomy (69.5 days [range, 25.5-103.5] vs 25 days [range, 14-50.2]; P = .149) were significantly different. Follow-up time after tracheostomy ranged from 42 days to 20 years, with a median period of 78.97 months. Demographic characteristics of patients who underwent tracheostomy are summarized in Table 2.
Demographics of Robin Sequence Patients Who Were Treated With Tracheostomy.
Compared to syndromic patients, non-syndromic patients were found to have higher rates of decannulation (92.9% vs 27.3%; P < .0001). Time to decannulation was 22.1 months in non-syndromic patients, while time to decannulation was undetermined in the syndromic group since most patients were not decannulated (Figure 4). Median length of hospital stay was significantly longer in syndromic patients compared to non-syndromic (51.5 days vs 29.0 days; P = .017). However, further analysis demonstrated that baseline demographic and clinical characteristics between syndromic and isolated RS were otherwise not significantly different including birth history, median number of oxygen desaturations, intensity of oxygen supplementation prior to surgery, and max HCO3/CO2 levels (Table 3).
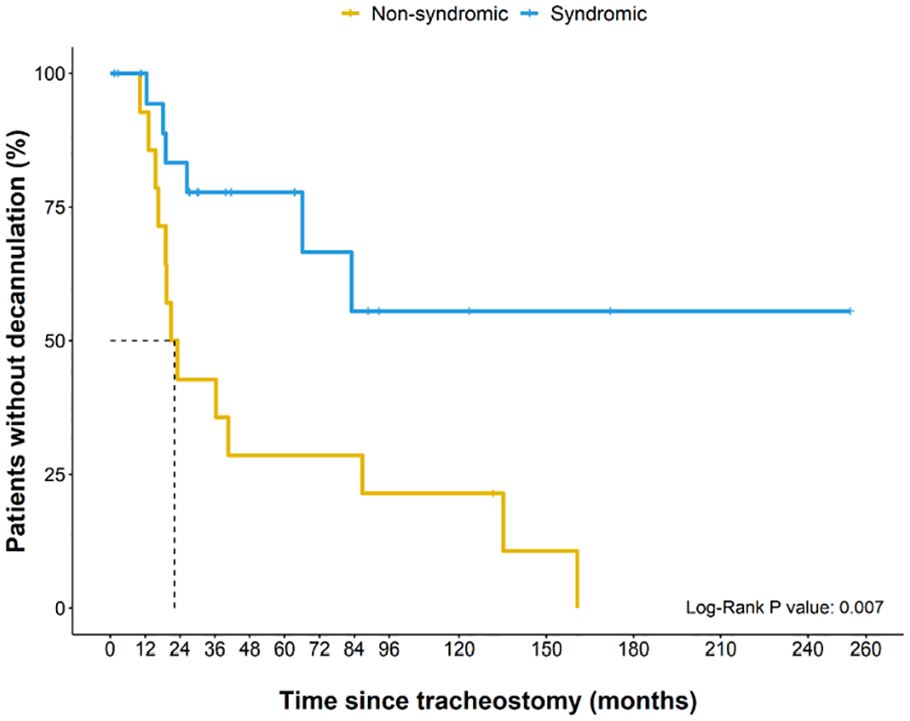
Patients with syndromic RS had an undetermined median time to decannulation, and patients with non-syndromic RS had a median time to decannulation of 22.1 months (P = .007).
Comparison of Demographic and Preoperative Hospital Factors Between Syndromic and Non-Syndromic RS With Tracheostomy.
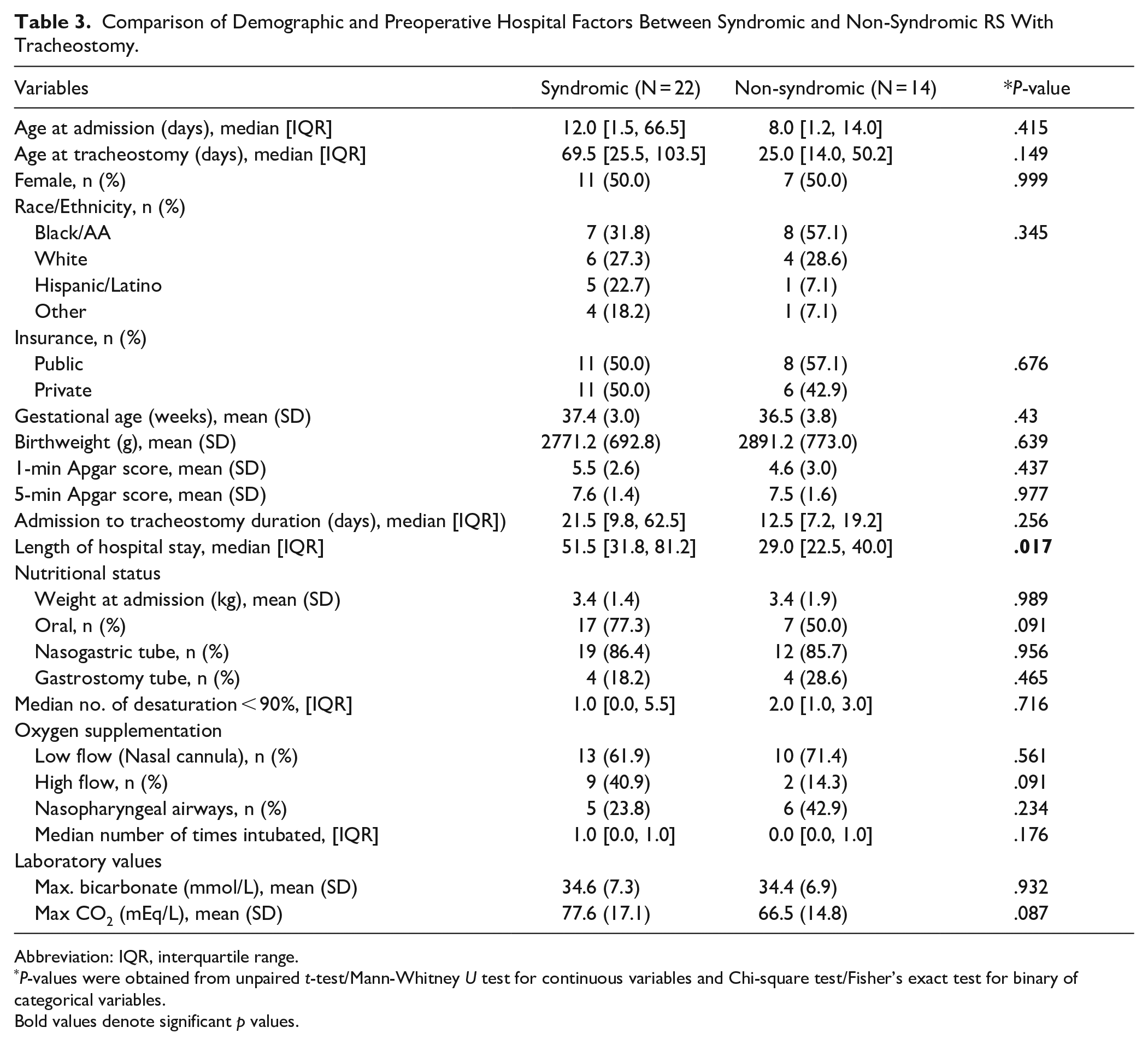
Abbreviation: IQR, interquartile range.
P-values were obtained from unpaired t-test/Mann-Whitney U test for continuous variables and Chi-square test/Fisher’s exact test for binary of categorical variables.
Bold values denote significant p values.
Cox proportions hazard ratio found that syndromic patients were associated with higher risk of not being naturally decannulated [aHR 12.5 (3.3-50.0); P < .001], while white race [aHR 0.15 (0.03-0.8); P = .023] and higher birthweight [aHR 0.9 (0.8-0.98); P = .018] were associated with a higher likelihood of having ND (Table 4).
Cox Proportional Hazard Model to Investigate the Potential Factors Associated With Barriers in Getting Natural Decannulation.
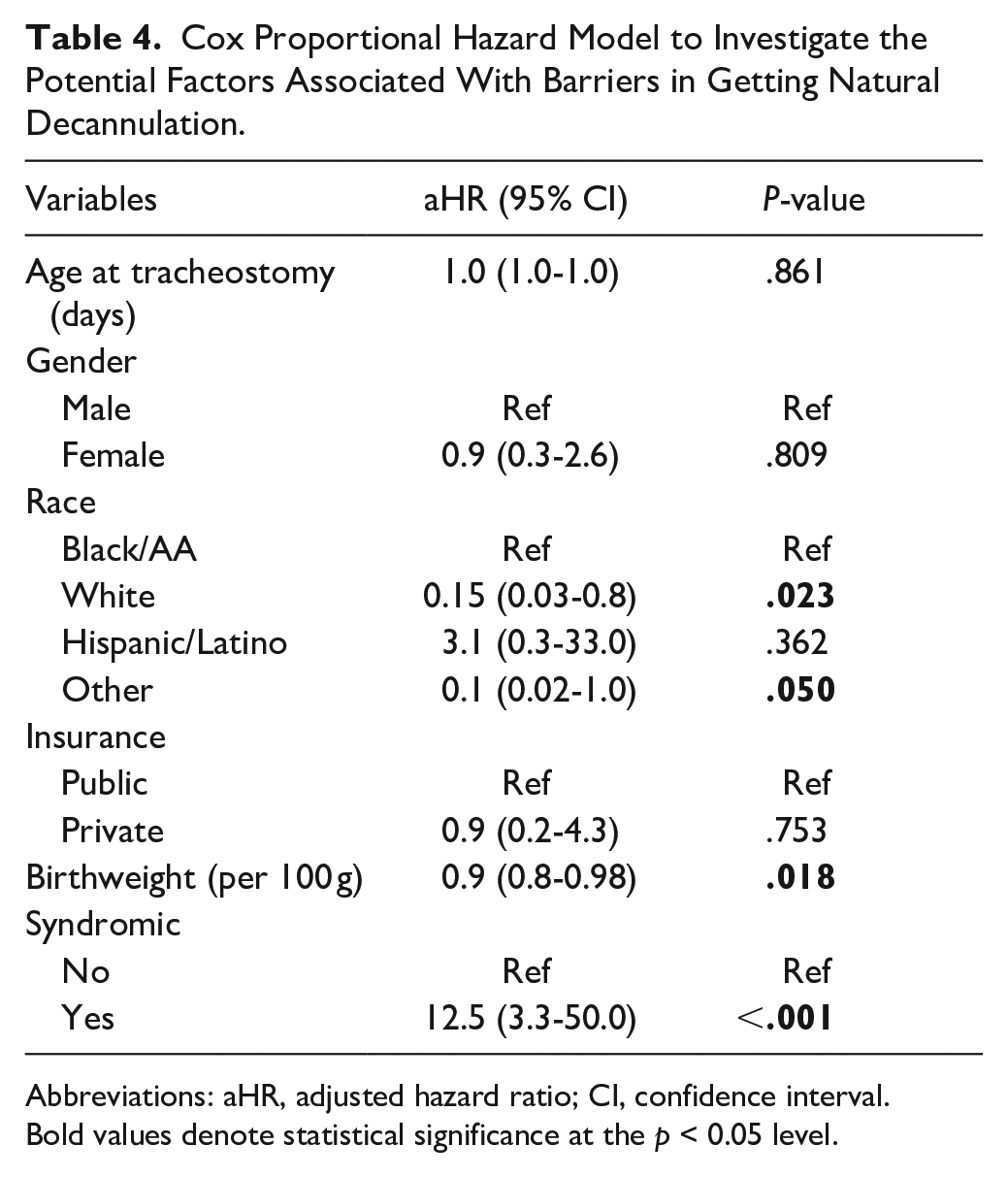
Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval.
Bold values denote statistical significance at the p < 0.05 level.
The rate of any tracheostomy-specific complications (tracheitis, pneumonia, wound issues, mortality) was 54%, with a tracheostomy-specific mortality rate of 3% (Table 5). There was no statistically significant difference in any tracheostomy related complications between syndromic and non-syndromic patients (P = .739).
Comparison of Tracheostomy Related Complications.
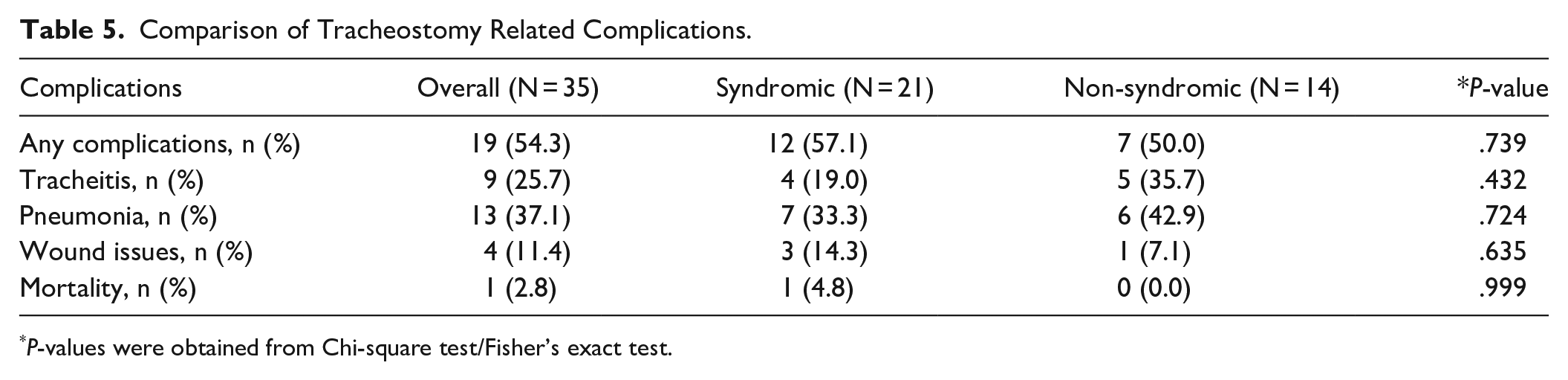
P-values were obtained from Chi-square test/Fisher’s exact test.
Discussion
Airway obstruction in infants with RS can lead to a variety of morbidities, including failure to thrive, developmental delay, feeding issues, dental anomalies, CO2 retention, heart damage, brain damage, and death.9-12 Reported mortality rates for RS range from 2% to 26% and are caused by several factors, including delayed identification of the UAO and securing of the airway.12-17
The core RS findings of glossoptosis, micrognathia, UAO, and typically cleft palate can occur in the presence of other congenital anomalies.4,17 Termed syndromic RS, this combination of anomalies has also been shown to be associated with higher rates of mortality, morbidity, and long-term tracheostomy dependence compared to isolated RS.1,13 Results from our cohort further support these findings; 93% of non-syndromic RS patients were naturally decannulated, while only 27% of the syndromic RS patients could be decannulated. Additionally, the median time to decannulation in non-syndromic RS patients was 22 months, while the overall time to decannulation in all RS patients was 66 months. The time to decannulation for syndromic RS patients could not be reliably determined since so many of the syndromic patients remain dependent on their tracheostomy. With that being said, the post-2007 cohort includes 55 syndromic patients while only 25.5% (n = 14) required tracheostomy; this supports the idea that altered management of UAO can result in ability to avoid tracheostomy in many of these patients.
Because of the morbidity and mortality associated with RS, clinicians have attempted to create standardized diagnostic and treatment protocols. Overjet measurement >4 mm should be used to diagnose micrognathia, 18 while pulse oximetry and/or polysomnography should be used to estimate degree of airway obstruction.18,19 Visualizing the airway before intubation via direct laryngoscopy with bronchoscopy, drug-induced sleep endoscopy, or other means is important in selecting the appropriate and least invasive treatment. 20
Prone positioning can help with mild respiratory obstruction by moving the tongue forward but is unlikely to be beneficial in severe cases. 21 Early nasopharyngeal tube placement can help open the airway and has minimal morbidity, and thus can be used to avoid tracheostomy.22,23 However, these are difficult to keep in place for long periods of time. 1 A shift in primary surgical management away from tracheostomy to TLA and/or MDO took place at our institution in 2007. TLA can stop the tongue from blocking the airway and can thus improve oxygenation parameters. However, some infants may still require further surgical management such as tracheostomy.24-27 Compared to TLA, MDO demonstrates superior outcomes, such as oxygen saturation and reduced need for subsequent tracheostomy.28-30 In syndromic RS, multiple MDOs may be required to fully clear the UAO.31,32 Like in patients who undergo TLA, tracheostomy may still be required for MDO patients with failed previous intervention, multiple sites of airway obstruction, central apnea, or other significant respiratory abnormalities.33-35 Indeed, in our cohort, 8 patients (7 with a syndromic association) initially treated with TLA and/or MDO (51 patients total) subsequently underwent tracheostomy. Three out of 8 were able to be decannulated. The difference in decannulation rate and time to decannulation did not significantly differ between patients treated with only tracheostomy compared to patients who required tracheostomy after TLA and/or MDO. This may be related to the low number of patients in our cohort who required subsequent tracheostomy; further studies analyzing decannulation outcomes in patients who require tracheostomy after TLA and/or MDO are warranted.
Tracheostomy provides definitive management by bypassing the UAO. Tracheostomies in children have a variety of indications, most commonly cardiopulmonary disease, neurological impairment, airway obstruction, and craniofacial/traumatic injury. 36 Patients in the 1995 to 2006 cohort required tracheostomy because they experienced repeated oxygen desaturations even with conservative management. Patients in the 2007 to 2020 cohort underwent tracheostomy because they failed conservative management, TLA, and/or MDO. Regardless of indication, tracheostomies can have severe complications. These have been reported in up to 58% of cases and include infection, granuloma formation, pneumonia, bleeding, accidental decannulation, and even death in up to 8% of cases.37-40 In our cohort, 54% of patients experienced complications with their tracheostomies. The most common complications in our cohort were pneumonia (68% of patients with complications) and tracheitis (47% of patients with complications).
Given the complications associated with tracheostomies, decannulation is an important milestone in the recovery of patients. Criteria for decannulation readiness include adequate airway exam, absence of oxygen requirements, and successful capping trials. 41 Factors contributing to failed decannulation are inability to tolerate secretions, pulmonary comorbidities, hypotonia, and persistent airway obstruction. 41 Syndromic patients in our cohort had lower likelihood of decannulation. We suspect that this difference is due to non-syndromic patients having fewer comorbidities and anatomic abnormalities, resulting in increased ability to clear decannulation milestones. The difference in management of UAO in syndromic and non-syndromic RS patients requires further research, especially in the context of avoiding tracheostomy in syndromic patients treated by alternative measures.
We also found that white race, “other” race, and higher birthweight were associated with increased likelihood of decannulation. Racial influence on pediatric tracheostomy outcomes has previously been documented with black children undergoing higher rates of tracheostomy and higher comorbidity burden compared to white or Hispanic children.42,43 However, there was no difference seen in rates of decannulation or mortality after tracheostomy.42,43 The difference in decannulation rates between white children and other racial or ethnic groups in our cohort highlights potential health disparities and the impact of social determinants of health on comorbidity burden. Further research is needed to assess for any differences in treatment efficacy among racial and ethnic groups including the associated socioeconomic influences and implicit biases. Addressing these factors can contribute to more equitable healthcare and improved outcomes for all children with RS.
Published median times to decannulation have widely varied; reported figures range from 28 to 97 months.1,5,8 Patients who could not be decannulated were not clinically stable; they have continued to experience airway symptoms even with tracheostomy in place. Reasons for this include low levels of consciousness and reduced ability to clear secretions.
In our cohort of 148 RS patients, 36 required tracheostomy to manage their UAO. This cohort of RS patients managed with tracheostomy is amongst the largest analyzed for decannulation data and the first to be considered in the context of tracheostomy’s displacement as primary surgical management for severe UAO in favor of TLA and MDO.
Our study helps clarify the sequelae associated with tracheostomy dependence and further reinforces differences in decannulation outcomes between syndromic and non-syndromic RS patients. We also categorized our cohort into 2 groups based on year of tracheostomy (1995-2006, 2007-2020) to find trends in decannulation over time. We found that 78% of patients in the 1995 to 2006 group were eventually decannulated, a rate that was higher than in the 2007 to 2020 group (28%). Patients who underwent tracheostomy from 1995 to 2006 had significantly shorter median times to decannulation and higher cumulative decannulation probabilities compared to patients in the 2007 to 2020 group. We suspect that these results are because tracheostomy was the sole surgical management option for RS infants with severe UAO at our institution before 2007. TLA and MDO have become accepted primary surgical treatment options for severe RS UAO due to their improved outcomes when compared to tracheostomy.
Our study had several limitations. The cohort was small, retrospective, and not all the patients were followed with a standardized management protocol. As in all retrospective studies, the patient information may have been inconsistently reported or with different criteria as the management teams changed over time. Documentation of conservative management of UAO in RS patients is also inconsistent but it is standard protocol to sequentially escalate care per each patient’s individual needs (prone positioning, nasopharyngeal airway, supplemental O2/positive pressure, intubation). This limitation is especially relevant in the reporting of complications as it is difficult to discern if morbidity and, occasionally, mortality are directly attributable to the tracheostomy itself or if the patient had a tracheostomy at the time of the complication. This reduces statistical power and may confound the decannulation data. Additionally, the fact that this is a single-center study limits generalizability.
Conclusion
Patients who underwent tracheostomy from 1995 to 2006 had significantly higher decannulation rates and lower median times to decannulation. This is likely because of the introduction of TLA and then MDO as primary surgical management for severe UAO in infants with RS. Tracheostomy for UAO in RS patients, especially those with syndromic RS, has higher rates of morbidity and long-term dependence. Thus, it is important to further study and address factors that lead to failed TLA and MDO to minimize patient morbidity and mortality associated with the use of tracheostomy in RS patients. Tracheostomy is now only reserved for the most critical syndromic airway obstruction cases and remains the gold-standard in patients with refractory severe UAO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Children’s National Hospital IRB number: 14271