
Abstract
Background:
Hereditary hemorrhagic telangiectasia (HHT) is a rare, autosomal dominant disease and epistaxis is the most common symptom. This can be treated conservatively but severe cases may require operative interventions. Endoscopic endonasal coblation of HHT lesions has been used successfully but postoperative pain management has not been well described.
Objectives:
This study aimed to assess levels of postoperative pain and opioid use among patients with HHT who underwent coblation of sinonasal lesions.
Methods:
This is a longitudinal, prospective cohort study of adult patients undergoing endoscopic endonasal coblation for treatment of HHT lesions with or without bevacizumab injection between November 2019 and March 2020 at a single academic university hospital. Patients were given preoperative questionnaires and contacted via telephone 48 hours after surgery. If they reported using opioids for pain control, they were called every 2 days until they no longer used these medications.
Results:
Fourteen cases, including 13 unique patients, were included in this study. Opioids were ordered on discharge in 4 cases and the average morphine milligram equivalent prescribed on discharge was 41. The median pain score on postoperative day (POD) 2 was 4 of 10. Twelve patients reported using acetaminophen and 4 were using opioid pain medications. Of those using opioid pain medications, only 1 patient was using opioid pain medication by POD 4 and denied any use after POD 10.
Conclusion:
This study is the first to analyze postoperative pain management and opioid prescribing patterns in HHT patients undergoing endonasal coblation of telangiectasias. Postoperative pain was mild to moderate and most patients stopped using opioid medications by POD 4, although the majority of patients solely used acetaminophen. Future studies with increased sample size will be useful to further identify predictors of need for analgesics postoperatively and other non-opioid adjuncts for pain control.
Keywords
Introduction
Hereditary hemorrhagic telangiectasia (HHT) is a rare, autosomal dominant disease. 1 Epistaxis is the most common symptom in this disorder and often is the presenting sign. 1 The severity of epistaxis is variable among patients with HHT, thus treatment options vary. Conservative measures, such as nasal humidification and moisturization, can be considered for mild cases. 2 For severe cases, cauterization with bipolar cautery, electrosurgical plasma coagulation (also known as coblation), and laser photocoagulation have been shown to provide benefit.3,4 Luk et al 4 found that coblation is as effective as laser photocoagulation, but with the added benefit of significantly less postoperative nasal obstruction. It is theorized that coblation provides superior benefits by decreasing the risk of damage to the healthy sinonasal mucosa surrounding the telangiectasias due to the lower temperature used to achieve ablation of the lesions. Despite successful use of coblation to treat intranasal telangiectasias, subsequent postoperative pain management has not been well described. It is important to consider appropriate pain management in patients with HHT specifically given the chronic nature of the disease and the likelihood that patients with severe disease may require ongoing procedures for disease control. Additionally, these patients often are instructed to avoid NSAIDS, so careful consideration of non-narcotic and narcotic pain medications is essential to improve postoperative quality of life and consider risks of opioid pain medications.
Opioid abuse and misuse is currently a public health crisis in the United States and prescription opioid abuse has been shown to be a major contributor. 5 In a national survey, 4 out of 5 people who use heroin reported first using prescription opioids. 6 Since opioid prescriptions often serve as the first opioid exposure, surgeons have a responsibility to prescribe opioids appropriately to reduce the risk of misuse.7,8 However, for many rhinologic conditions, optimal pain management strategies have not been identified. This creates a challenge as physicians attempt to balance appropriate analgesia with risk for over-prescribing and subsequent opioid misuse and abuse.
Younger age, female sex, smoking, history of depressive or anxiety symptoms, sleep difficulties, higher body mass index (BMI), and presence of preoperative pain have been identified as significant predictors of poor postoperative pain control among a wide variety of non-rhinologic surgeries. 9 Recent studies evaluating postoperative opioid use in endoscopic sinonasal surgery found that the complexity of surgery was not associated with the amount of opioid medication used but was associated with younger age and concurrent septoplasty.10,11 Several studies have also found that patients often do not use all of the prescribed opiates after endoscopic sinus surgery.10,12 As discussed in other surgical fields, this increases the risk of opioid misuse and diversion. 13
Despite the work to understand opioid prescribing patterns and predictors of postoperative pain in endoscopic sinonasal surgery, there are no studies investigating perioperative pain in patients with HHT nor a discussion of the available options. Given that endoscopic sinus surgery has been demonstrated to result in minimal opioid use, it would be expected that nasal coblation would also require minimal opioid use. This study aimed to identify opioid prescribing patterns, perioperative pain control, and opioid use in patients with HHT undergoing coblation with or without bevacizumab injections.
Methods
This study was a longitudinal, prospective cohort study of adult patients scheduled to undergo endoscopic coblation for treatment of HHT telangiectasias of with or without bevacizumab injection between November 2019 and March 2020 at a single large academic university hospital. Oregon Healthy & Science University institutional review board approval was obtained. Exclusion criteria included age less than 18 years old, prior surgery within 60 days of coblation, inability to communicate in English, and vulnerable individuals (pregnant women, decisional impaired adults, inmates). Patients undergoing other combined open and endoscopic surgical procedures were excluded. Patients were also excluded if complete pain and opioid use data could not be obtained.
Patients completed preoperative questionnaires regarding medical history, the generalized anxiety disorder 2-item (GAD-2), and the patient health questionnaire-2 (PHQ-2). The GAD-2 is a screening questionnaire for generalized anxiety disorder consisting of 2 questions with scores ranging from 0 to 6. A score greater than or equal to 3 suggests that the patient should undergo further evaluation for generalized anxiety disorder. The PHQ-2, a screening questionnaire for depression, has 2 questions with a maximum score of six. A score greater than or equal to 3 is a positive screen and indicates that the patient should undergo further evaluation for major depressive disorder.
Patients were contacted via telephone every 48 hours after surgery and asked to quantify pain and opiate consumption. They were then contacted every 48 hours until they were no longer requiring opioids for pain control. If patients did not report opioid use at the first phone call, no additional calls were made. To quantify pain, patients were asked to rate their pain over the last 48 hours on a numeric pain rating scale (0-10). Patients were contacted again at 2 months post-operatively to inquire about opiate disposal.
The electronic medical record of each patient was reviewed to provide additional demographic and comorbidity information. Data collected included age, gender, operative details, post anesthesia care unit medication administration, and discharge medication regimen.
The primary outcome was total post-operative opioid consumption in morphine milligram equivalents (MME). The secondary outcome measurement was mean average facial pain on post-operative day (POD) 2 and 4. Descriptive statistics were performed to determine average cohort demographics and characteristics with Microsoft Excel ® 2010.
Results
Fourteen cases, including 13 unique patients, were included in this study. There were 9 men and 4 women with an average age of 65 years old. Six patients denied any alcohol use while 7 reported low to moderate use, defined as less than 7 drinks per week for women and less than 14 drinks per week for men. Three patients reported marijuana use and 1 patient endorsed smoking tobacco. Nine patients endorsed exercising at least 2.5 hours per week (Table 1).
Demographic Information and Intake Survey Results.
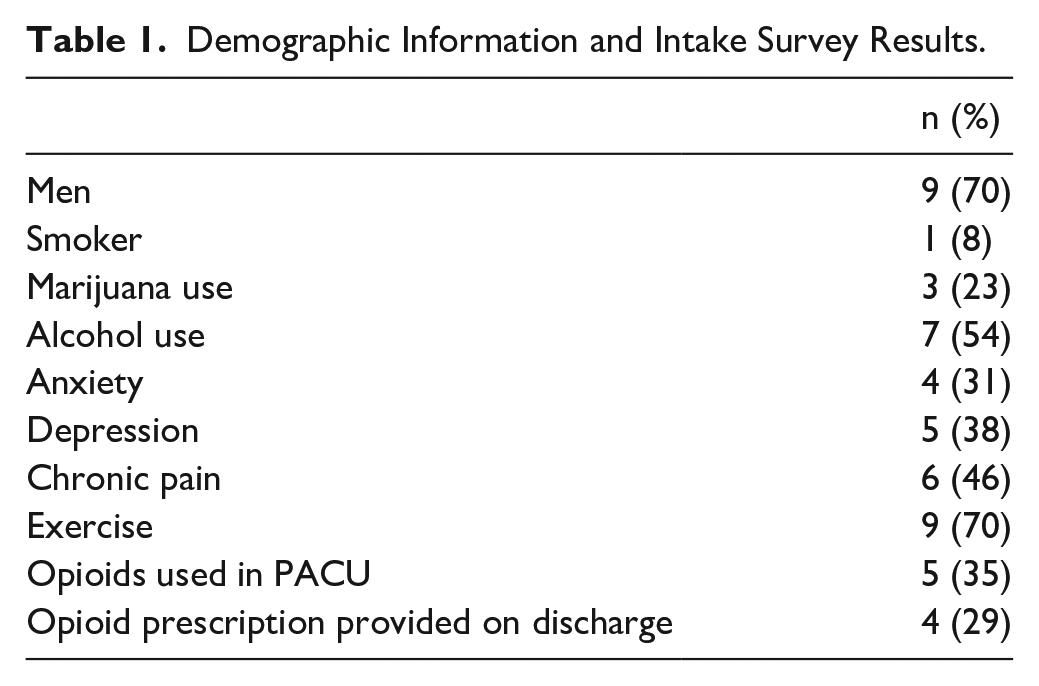
Four patients had a documented history of anxiety and 5 had a history of depression on chart review. However, on the GAD2 assessment all patients scored between 0 and 2. On the PHQ2, for which depression is more likely with a score greater than or equal to 3, 1 patient had a positive screen while all others scored less than 3.
Six patients in this study had a history of chronic pain due to arthritis, migraines, and back pain but all patients denied any opioid use within 60 days prior to their procedure. Many patients reported a history of in-office nasal cauterization at other institutions. Median prior operative procedures was 1, with a range from 0 to 13. The median preoperative pain score was 4, with a range from 0 to 4. Patients were asked what pain score would prompt them to use an opioid medication and the average response was 6.3 out of 10.
All patients underwent bilateral coblation of intranasal telangiectasias. Subsites treated included anterior and posterior nasal septum, lateral nasal sidewall, inferior turbinate, middle turbinate, middle meatus, nasal floor, and nasal roof. The coblator was used on a bipolar setting of 3 or 4 in all cases. Four patients also underwent concurrent intranasal bevacizumab injections. The median case length was 37 minutes with a range from 19 to 106 minutes. Of the 14 cases, 12 had opioid medications available for as needed us in the post-anesthesia care unit (PACU) and 5 patients used them. An average of 11 MME was used per patient in the PACU. Opioids were ordered on discharge in 4 cases but on chart review there was no clear indication other than provider variability. The average MME prescribed on discharge was 41. For reference, this is equivalent to about 5.5 doses of one 5 mg oxycodone tablet.
On POD 2, the median pain score was 4 with a range from 0 to 9. A total of 4 patients utilized opioids after discharge from the hospital: 3 of the 4 patients prescribed opioids on discharge and 1 additional patient, who used opioids from a prior surgery. The average pain score among these patients was 6 of 10 compared to 3.4 among patients that were not taking opioids. These 4 patients reported an average of 40 MME use (Figure 1). Twelve patients used acetaminophen for pain control, but only 2 of the 4 who reported opioid use also used acetaminophen for pain control. These patients underwent an average of 1.5 operative procedures before the procedure in this study and the average for patients who did not use opioids was 2.4. Additionally, among patients who used postoperative opioids, the case length was varied and included 19, 37, 71, and 106 minutes. The average case length among patients who used postoperative opioids was 58.3 minutes. The average for patients who did not use postoperative opioids was 39.4 minutes.
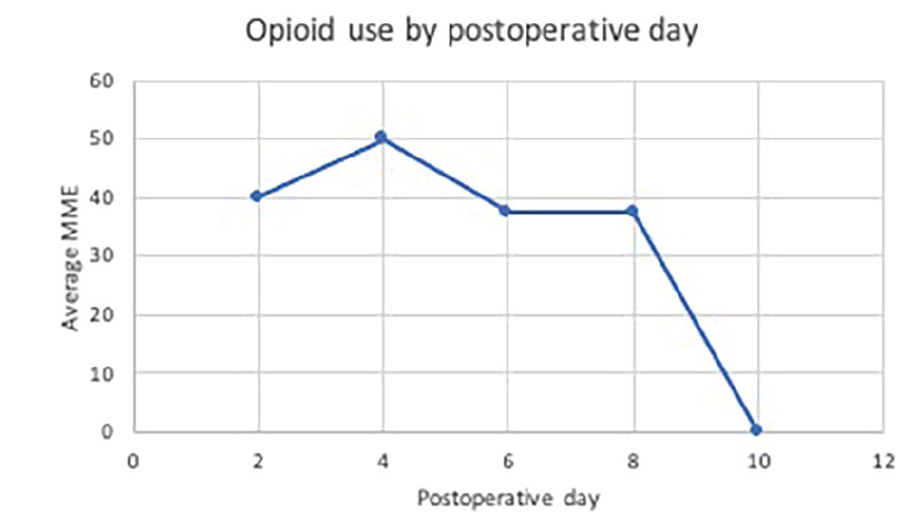
Opioid morphine milligram equivalent use by postoperative day. No patients reported using opioid medications after postoperative day eight.
The 4 patients who reported using opioids on POD 2 were called on POD 4. Median pain score of these 4 patients on POD 4 was 5 with a range from 4 to 6. Only 1 patient was still using opioids on POD 4 and reported use of 50 MME per day. This patient reported using opioids from a prior prescription. This patient reported a pain score of 4 and 37.5 MME opioid use on POD 6. On POD 8 this patient reported a pain score of 4 and 37.5 MME opioid use. On POD 10 this patient reported a pain score of 4 and denied any further opioid use. There were no significant differences in opioid use between patients who had coblation with or without bevacizumab injections.
The 4 patients that were prescribed opioids on discharge were called again 2 months postoperatively to inquire about opioid disposal. Among these patients, they were prescribed an average of 40.9 MME at discharge, about 5.5 dosease of 5 mg oxycodone tablets. Two patients reported using all of the provided tablets but the other 2 patients were not reached to answer this question.
Discussion
This prospective cohort study demonstrates cases of postoperative pain management and variability in opioid prescribing for patients with HHT undergoing coblation. Most patients had opioids available in the PACU but only 4 had discharge prescriptions ordered. These were prescribed because of patient request and provider variability but were not routinely given.
The majority of patients in this study did not require postoperative opioids for pain control and the median pain score on POD 2 was mild to moderate at 4 out of 10. Among the patients who used opioids, most stopped by POD 4, which is consistent with previously reported literature in septoplasty and endoscopic surgery discussing expected pain to be 2 to 5 days for those cases. 8 Of the 4 patients taking opioids for postoperative pain control, only 2 were using acetaminophen as an adjunct. This demonstrates an area for improvement in counselling patients about the efficacy of acetaminophen use for postoperative pain. Acetaminophen use has been shown to have synergistic effects with opioids so is a useful adjunct in management of perioperative pain. 14 Consideration of a scheduled regimen of acetaminophen should also be discussed with the patient first 1 to 2 days postoperatively given the early pain scores observed in this study.
Typical postoperative pain regimens include acetaminophen and opiates as needed. HHT patients are often instructed to avoid non-steroidal anti-inflammatory drugs (NSAID), due to the fear of precipitating bleeding, thus these are not routinely used postoperatively. However, HHT consensus guidelines suggest that anticoagulant or antiplatelet use is reasonable if used for a specific indication and balanced with the risk of bleeding for individual patients. 15 It may be useful to identify preoperatively if patients have been instructed to avoid NSAIDs and work collaboratively with the patient’s primary care provider to determine if NSAID avoidance is truly necessary. The combined use of ibuprofen and acetaminophen was specifically studied in endoscopic sinus surgery where it was found that the combined use of ibuprofen and acetaminophen provided improved analgesia than acetaminophen alone. 16 Additionally, use of scheduled acetaminophen and NSAIDS provides additive analgesia, demonstrated in a variety of surgical patients, and could be considered for this patient population along with other adjuncts such as celecoxib, instead of ibuprofen, and gabapentin. 14 Future studies to include trials of NSAIDs and acetaminophen in the HHT patient population will be useful for further study of non-opioid adjuncts in this patient population.
Interestingly, the median pain score preoperatively was 0, despite many patients presenting with significant crusting and potential for pain. There was not an association of increased preoperative pain and postoperative opioid use. Additionally, there was not a relationship to suggest that higher number of previous operative procedures, suggesting longstanding severe disease, was associated with postoperative opioid use. Additionally, the case length, a proxy for procedural severity, was not a predictor for postoperative opioid use. The 4 patients who used opioids postoperatively underwent cases with varying lengths that were shorter, at, or longer than the median time among all patients in the cohort. Despite the findings in this small cohort, these factors may contribute to postoperative pain and should be studied further with larger cohorts.
In regards to opioid disposal, 2 patients reported using all tablets provided but 1 patient, who was not prescribed any opioids after the procedure, reported using opioids from a prior surgery for pain control. A known risk for opioid misuse is keeping previous unused opioid prescriptions and, despite our small sample size, we identified 1 patient doing just this. This patient reported using opioids when reporting a pain score of 4 but reported stopping also when the pain score was still a 4, on a later postoperative day. This raises the question of the true utility of opioids versus use due to availability. A recent systematic review of 810 patients found that only 4 to 30% of patients disposed, or planned to, their unused opioids. 17 Only prescribing the necessary amount of opioids is a method to mitigate the risk of unused opioids, which often stored unlocked locations. 17 Additionally, patient education regarding the importance of, and options for, disposal of unused opioids significantly affects the proportion of patients who dispose of these medications. 18 Improved understanding of postoperative pain allow us to prescribe what is necessary and decrease the risk of opioid misuse while adequately treating postoperative pain. In our study, the minority of patient required opioid prescriptions with an average opioid use of 20 MME, about 2.5 doses of a 5 mg oxycodone tablet. This finding demonstrates a significantly lower use of opioids compared to the findings in a recently published action clinical practice guideline which demonstrated a mean consumption rate of 9.7 doses of 5 mg oxycodone tablets, 72.8 MME, for septoplasty with or without turbinate reduction. 8 Therefore, we suggest counseling patients to rely primarily on acetaminophen for postoperative pain and prescribing opioids, such as a 2 to 3 doses of 5 mg oxycodone tablets, only if needed.
This study has several limitations, including small sample size, provider variability, and reliance on patient description of opioid use at home. However, this is the first study to specifically evaluate postoperative pain in HHT patients after endoscopic endonasal intervention for epistaxis. Future studies with increased sample size and multi-institution cohorts will be valuable to improve generalizability while studying the management of patients with HHT. Several patients in this study had risk factors for poor postoperative pain control, such as history of anxiety and depression, but had negative screening on questionnaires at the time of surgery. In our small sample this did not appear to be a risk factor. Future studies with larger sample sizes are needed to further analyze these risk factors. Opioids were prescribed in the PACU and on discharge by several different providers which inherently leads to variability in prescribing practices. A standardized approach will be useful in the future and will improve identification of patients who are experiencing more severe pain necessitating medications for analgesia rather than potentially masking this group with routine prescriptions.
Conclusion
This study is the first to analyze postoperative pain, perioperative pain management, and opioid prescribing patterns in HHT patients undergoing endonasal coblation of telangiectasias. Postoperative pain was mild to moderate and most patients stopped using opioid medications by POD 4, although the majority of patients did not use any opioid medications. Future studies with increased sample size will aid in identifying predictors for need for postoperative analgesics in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.