
Abstract
Objectives:
To investigate the etiology and ossicular pathology of traumatic ossicular injury in Taiwan and examine the hearing outcomes and predictive factors between the titanium prosthesis and autologous incus groups.
Methods:
We retrospectively analyzed patients with traumatic ossicular injury from 2011 to 2020 in Taiwan. Patients were divided into the titanium or autologous group according to the surgical materials used. The audiometric outcomes and predictive factors of ossiculoplasty were analyzed between groups.
Results:
Twenty patients with ossicular chain discontinuity were enrolled (8 in the titanium group and 12 in the autologous group). The postoperative hearing threshold (26.6 ± 8.9 dB) and air-bone gap (10.3 ± 5.6 dB) improved significantly compared with the preoperative hearing threshold (50.7 ± 13.3 dB) and air-bone gap (29.9 ± 11.0 dB). The improvements in the hearing threshold and air-bone gap were not significantly different between the titanium and autologous groups. Our patients presented an improvement in hearing restoration with 65% closure of the air-bone gap in 0 to 10 dB range and 30% in 11 to 20 dB range, without sensorineural hearing loss during surgery. Univariate regression analysis revealed that vertigo, benign paroxysmal positional vertigo, and temporal bone fracture may serve as negative factors influencing the air-bone gap gain.
Conclusions:
Ossiculoplasty with both titanium prosthesis and autologous materials demonstrated favorable hearing recovery in traumatic ossicular injury. Vertigo, benign paroxysmal positional vertigo, and temporal bone fracture may serve as negative predictive factors of the hearing benefit after surgery.
Introduction
Traumatic ossicular injury or a disconnected ossicular chain is a common cause of conductive hearing impairment that requires surgery. Traffic accidents are the most common etiology causing ossicular injury, and other reasons include falling from a height, head/ear trauma, and foreign body insertion. 1 Ossicular injury is of various types, such as incudostapedial (I-S) joint dislocation and separation (the most common ossicular pathology),2,3 fracture or erosion of the long process of the incus, absence or dislocation of the incus, fracture of the anterior crus or footplate of the stapes, and incudomallear (I-M) joint dislocation.1,4
High-resolution computed tomography (HRCT) of the temporal bone is the gold standard for the diagnosis of ossicular injury. However, this method cannot detect some minor lesions with or without temporal bone fracture due to hemotympanum or soft tissue swelling. Surgical exploration of the middle ear and ossiculoplasty is a common treatment. Different types of ossiculoplasty and materials can be chosen according to the lesion site and injury severity. The choices include autologous ossicular (incus) replacement, piston, partial ossicular replacement prosthesis (PORP), and total ossicular replacement prosthesis (TORP).
Most people (72%) experience hearing improvement after air-bone gap (ABG) closure within 10 to 20 dB after ossiculoplasty. 1 Studies have revealed that autologous incus groups have higher ABG improvement and lower complication rates than titanium PORP groups in patients having chronic otitis media (COM) with Austin type A ossicular defects. 5 Moreover, the integrity of the middle ear mucosa and the stapes superstructure were significant predictors of surgical success in patients with COM who received ossiculoplasty. 6 However, the efficacy of different materials used, such as ossicular autografts or titanium prosthesis, and the predictive factors of hearing improvement remain unclear in patients with traumatic ossicular injury.
In this study, we investigated the etiology and ossicular pathology of traumatic ossicular injury in Taiwan. The epidemiology, treatment efficacy, outcomes such as hearing benefit, and possible predictive factors were also examined between titanium prosthesis and autologous materials.
Materials and Methods
We retrospectively analyzed patients with traumatic ossicular injury from 2011 to 2020 at (Blinded for review) in Taiwan. Patients were divided into titanium and autologous groups according to the surgical materials used for ossiculoplasty. Patients with incomplete audiometric data or those lost to follow-up after surgery were excluded. Patients’ epidemiological profiles were reviewed, and the audiometric outcomes between the 2 groups and the predictive factors of ossiculoplasty were analyzed.
All patients underwent pure tone audiometry preoperatively and postoperatively at 3 months. The hearing thresholds of the air conduction (AC), bone conduction (BC), and ABG were calculated at frequency averages of 0.5, 1.0, 2.0, and 3.0 kHz; furthermore, the BC at frequency averages of 1.0, 2.0, and 4.0 kHz was used to evaluate the surgery-related damage to hearing according to the Committee on Hearing and Equilibrium guidelines. 7 The difference in the BC before and after surgery indicates surgery-related damage of the cochlea. The changes in the AC and ABG at a high frequency of 4.0 kHz may demonstrate the benefit gained from using prosthesis or autologous bone after ossiculoplasty. 8 This study was approved by the Institutional Review Board (Blinded for review).
All surgical procedures were performed under general anesthesia and by the same senior experienced surgeon. Ossiculoplasty was conducted through the postauricular approach by using a microscope (HAAG-STREIT SURGICAL Hi-R 700, HAAG-STREIT SURGICAL GmbH & Co. KG, Wedel, Germany). Titanium prosthesis (PORP, Grace Medical, Memphis, TN, USA) or autologous materials (sculpted incus interposition graft) were chosen by the surgeon according to the lesion and the severity of injury. The temporal fascia was harvested, and an underlay graft was placed above the stapes medial to the malleus or cartilage for reconstruction. The conditions of the middle ear cavity and ossicle chain were assessed and recorded for subsequent analysis.
JMP 15.0 (SAS Institute, Cary, NC, USA) statistical software was employed for analysis. Two-sample t tests and paired t tests were used between the 2 groups and within each group for assessing continuous variables, such as age, operative time, and hearing threshold before and after surgery. Fisher’s exact test was used to assess categorical variables between the groups with small sample sizes, with a significance level of P < .05. Univariate linear regression analysis of various independent variables influencing the ABG gain (dependent variable) was performed. The predictive factors included age, sex, smoking, laterality, vertigo, benign paroxysmal positional vertigo (BPPV), tinnitus, ear drum perforation, facial palsy, concurrent temporal bone fracture, and the use of titanium prosthesis or autologous materials. We used the diagnostic criteria in the ‘‘Clinical Practice Guideline: Benign paroxysmal positional vertigo’’ 9 from the AAO-HNS in 2008 to define BPPV patients that were enrolled in this study. A P value of <.05 indicated statistical significance. A Glasgow benefit plot 10 of the AC was used to visualize the hearing benefit before and after surgery in the operative ear in comparison with the nonoperative ear by using the 4-frequency averages of 0.5, 1.0, 2.0, and 3.0 kHz.
Results
Twenty patients with ossicular chain discontinuity were enrolled, with 8 in the titanium group (40%) and 12 in the autologous group (60%). Traffic accidents accounted for 90% of the traumatic events, and penetrating trauma through the ear canal accounted for 10%. The ossicular pathology was I-S dissociation, I-M dissociation, and incus luxation in 60%, 25%, and 15% of the patients, respectively. The age range was from 20 to 63 years old, with a mean age of 37.8 ± 13.9 years old. Of the participants, 9 were men and 11 were women; 8 had ossicular chain discontinuity in the right ear and 12 in the left ear; and the average duration from traumatic injury to ossiculoplasty was 4.83 ± 3.28 months. The average follow-up time was 3.58 ± 1.94 months. No significant differences were observed in age, sex, smoking, laterality, operation time, concurrent temporal bone fracture (15 cases with longitudinal fracture and 1 case with transverse fracture), and related symptoms between the titanium and autologous groups. The demographic profiles and clinical findings of enrollees are presented in Table 1.
Demographic Data.
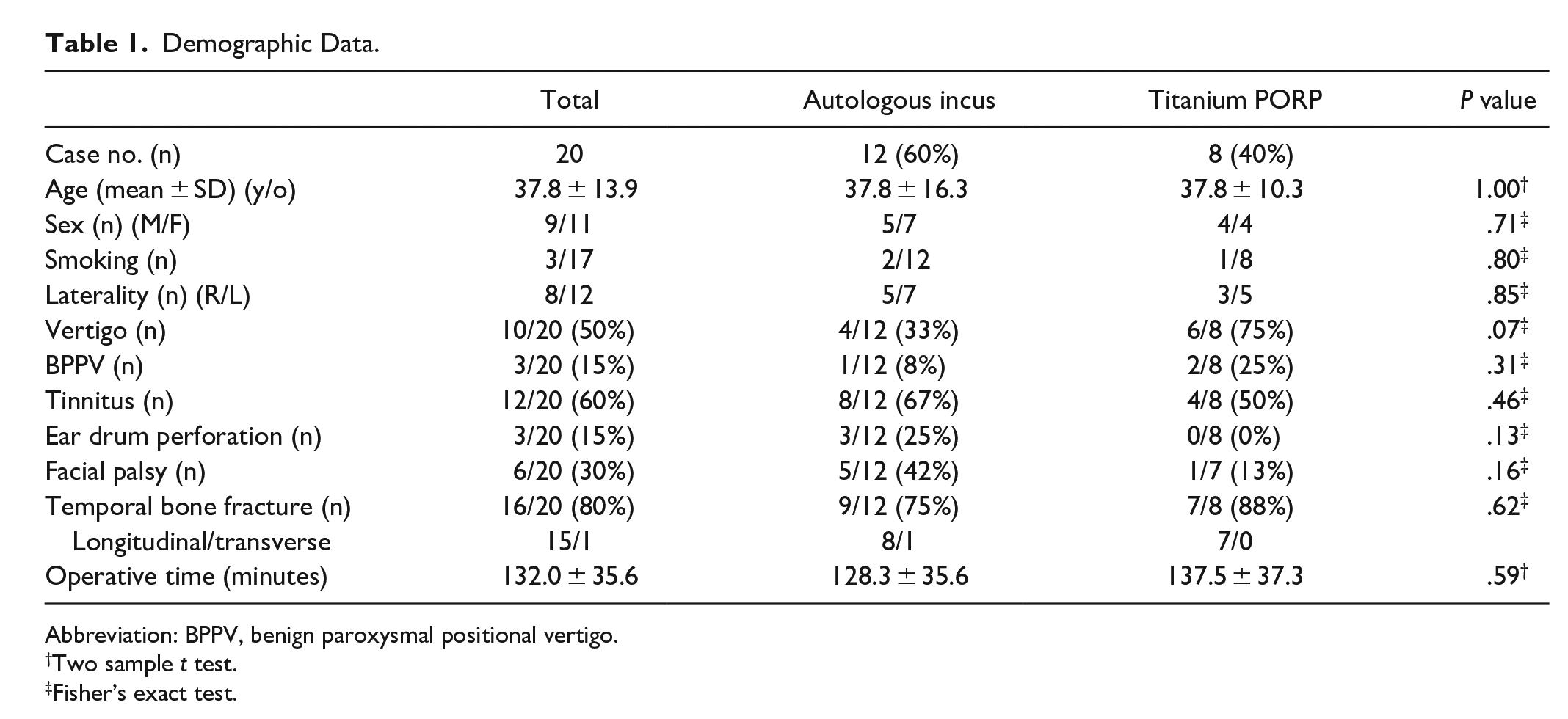
Abbreviation: BPPV, benign paroxysmal positional vertigo.
Two sample t test.
Fisher’s exact test.
The postoperative AC improved significantly compared with the preoperative AC in both the titanium (26.9 ± 8.9 and 50.6 ± 13.5 dB, respectively) and autologous groups (26.4 ± 9.2 and 50.7 ± 13.8 dB, respectively). Furthermore, the postoperative ABG improved significantly compared with the preoperative ABG in both the titanium (10.8 ± 5.1 and 25.9 ± 12.2 dB, respectively) and autologous groups (10.0 ± 6.1 and 32.5 ± 9.8 dB, respectively). Hearing restoration after surgery at an average 3-month follow-up was not significantly different between the titanium (AC gain = 23.8 ± 13.1 dB and ABG gain = 14.7 ± 11.6 dB) and autologous groups (AC gain = 24.4 ± 9.8 dB, ABG gain = 22.5 ± 9.4 dB; AC gain, P = .91, and ABG gain, P = .14, respectively), indicating that these 2 surgical materials offer similar hearing benefits (Table 2) and exhibit similar operation times (Table 1). The postoperative ABG distribution is illustrated in Table 3; 65% of the patients showed closure of the ABG in 0 to 10 dB, and 30% of the patients showed an improved ABG within 11 to 20 dB. No significant differences in the preoperative and postoperative BC were noted between the groups (Table 2, P = .0665 in the titanium group and P = .7896 in the autologous group), indicating no hearing impairment during surgery. Furthermore, our results showed significant improvements in the AC and ABG after ossiculoplasty (Table 2, total cases, AC, P < .0001; ABG, P < .0001), and similar results were found at the high frequency of 4.0 kHz, demonstrating that the use of both prosthesis and autologous materials is favorable for hearing restoration and sound transmission up to 4.0 kHz. Moreover, both groups exhibited an improved AC after surgery in the operative ear compared with that in the nonoperative ear, as illustrated in Figure 1.
Preoperative and Postoperative Audiological Data.
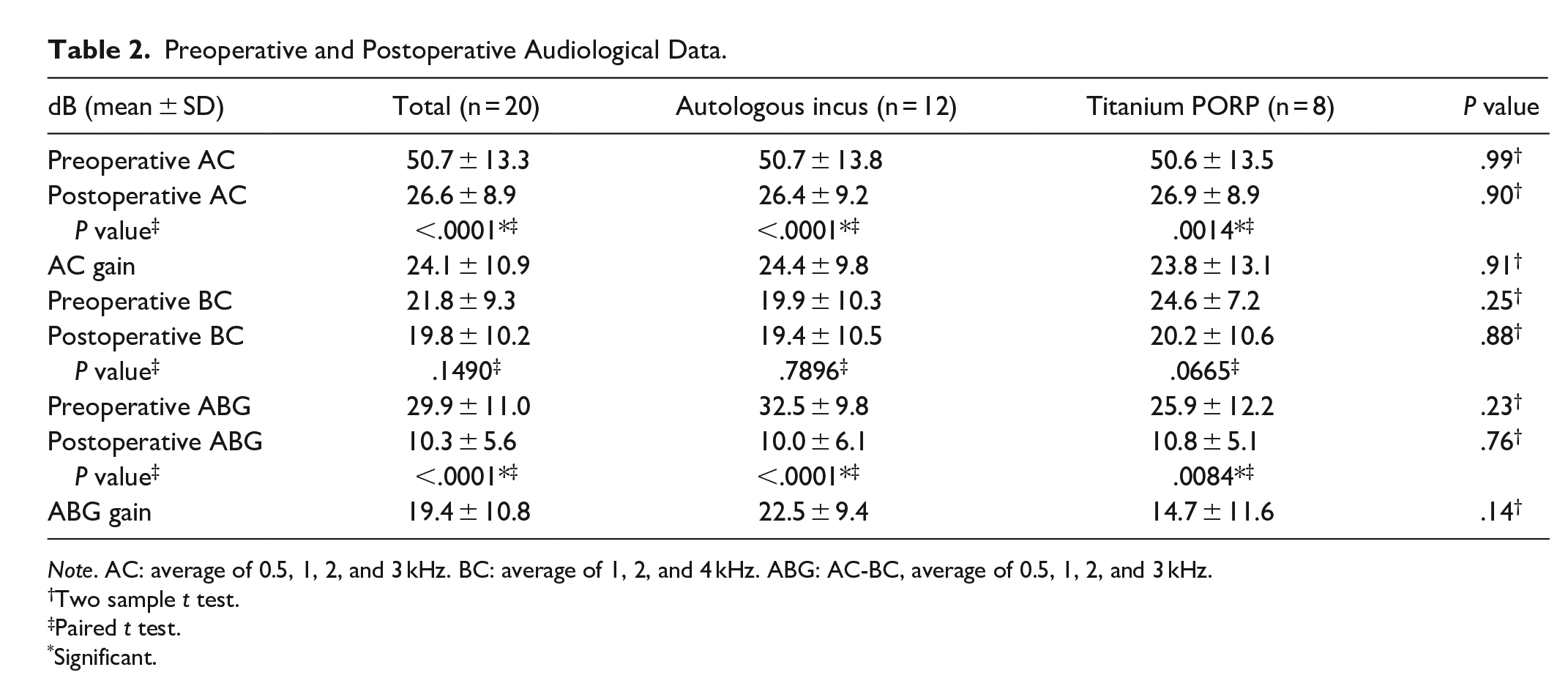
Note. AC: average of 0.5, 1, 2, and 3 kHz. BC: average of 1, 2, and 4 kHz. ABG: AC-BC, average of 0.5, 1, 2, and 3 kHz.
Two sample t test.
Paired t test.
Significant.
Postoperative ABG Distribution.
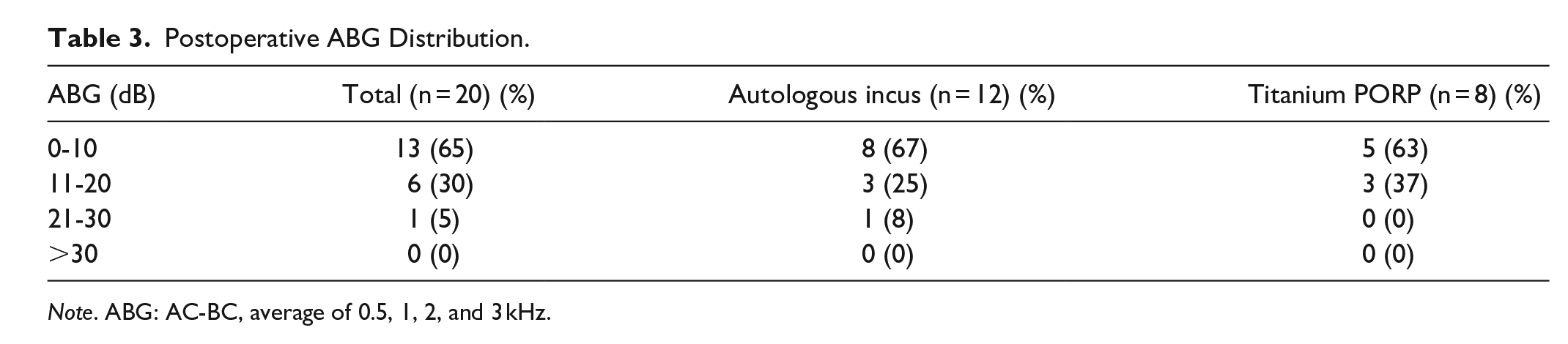
Note. ABG: AC-BC, average of 0.5, 1, 2, and 3 kHz.
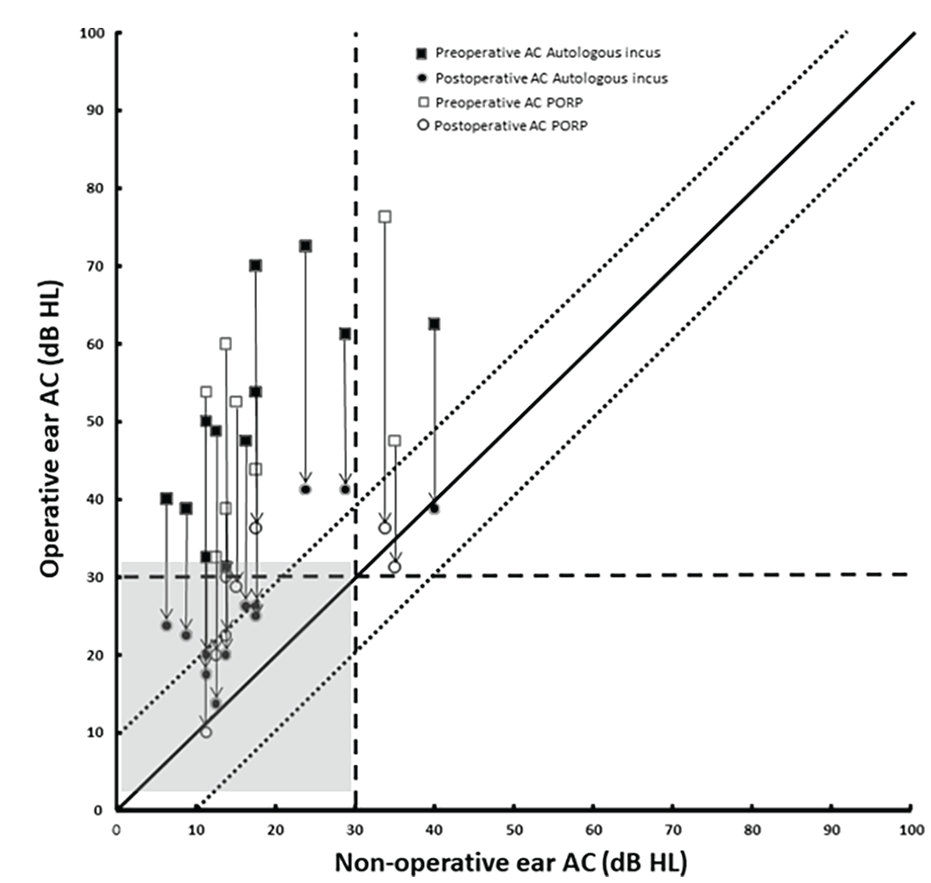
Hearing results demonstrated using the Glasgow benefit plot. Each line represents a different patient. The length of the line represents the change in air condition thresholds and the arrow show the direction of change.
The results of the univariate linear regression analysis of predictive factors influencing ABG gain are shown in Table 4. No significant differences in age, sex, smoking, laterality, tinnitus, ear drum perforation, facial palsy, and materials used were noted. However, we found the significant association between the variables of vertigo (regression coefficient, β = 5.56; 95% CI = 1.14 to 9.99; P = .0166), BPPV (regression coefficient, β = 11.02; 95% CI = 6.17 to 15.87; P = .0002), temporal bone fracture (regression coefficient, β = 6.33; 95% CI = 0.61 to 12.04; P = .0318), and the ABG gain. Even through the small sample sizes, these variables may be the potential predictive factors of hearing benefit after surgery. During the average 3-month follow-up, no titanium prosthesis or autograft extrusion was observed.
Univariate Linear Regression Analysis of Predictive Factors Influencing ABG Gain.
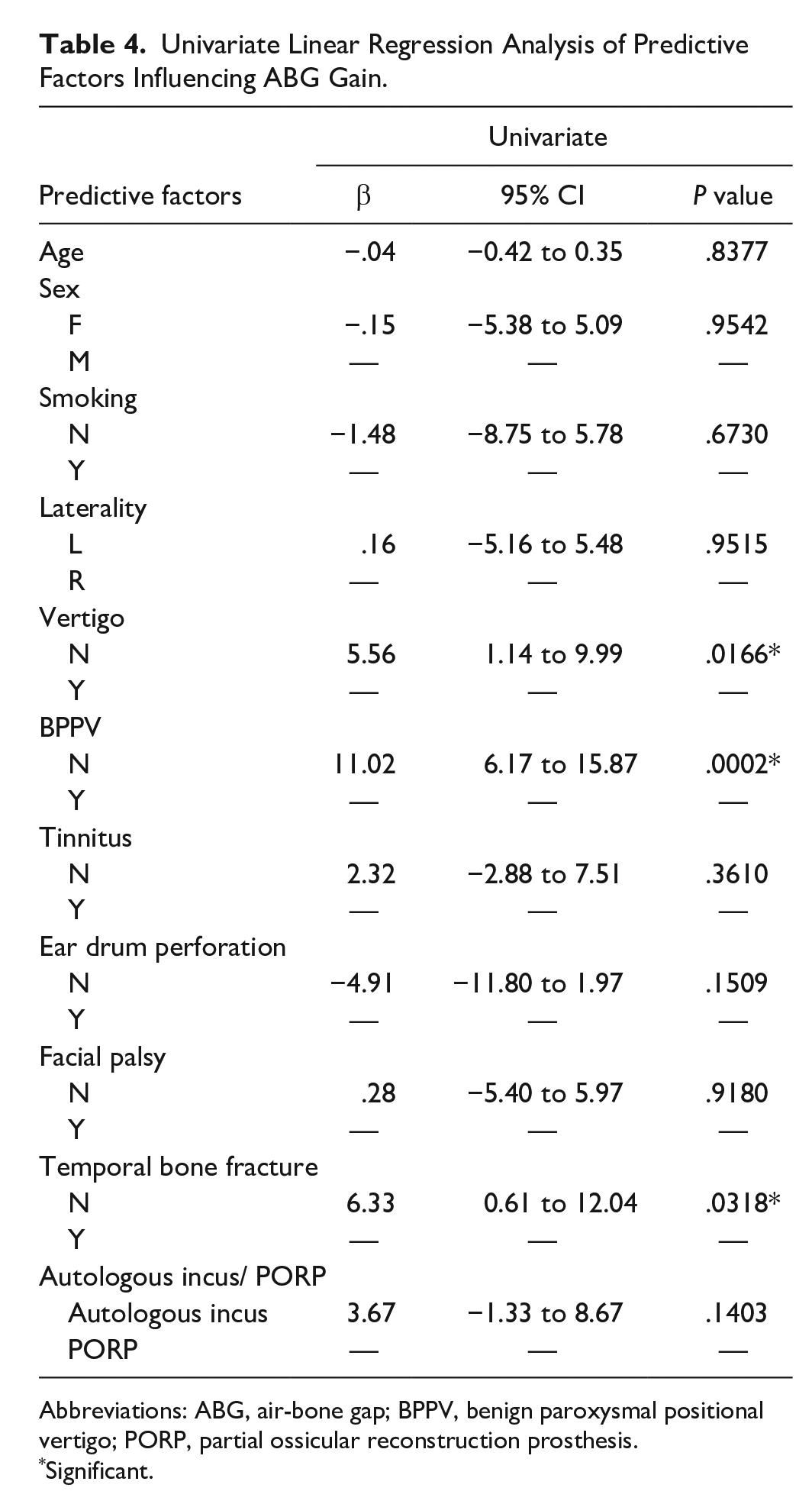
Abbreviations: ABG, air-bone gap; BPPV, benign paroxysmal positional vertigo; PORP, partial ossicular reconstruction prosthesis.
Significant.
Discussion
In this study, we retrospectively analyzed 20 patients with traumatic ossicular injury who received ossiculoplasty for ossicular chain discontinuity. Our results revealed an improvement in hearing with 65% closure of the ABG in 0 to 10 dB and 30% in 11 to 20 dB, without hearing damage during surgery. Both the inserted materials were favorable for ossicular reconstruction, and the hearing threshold of operative ears reached recovery to the level of nonoperative ears in most patients. Moreover, vertigo, benign paroxysmal positional vertigo, and temporal bone fracture may be potential predictive factors of the ABG gain from surgery.
The most common etiology of ear injury is traffic accidents with temporal bone fracture and falling from various heights1,4; thus, the severity of injury may vary. In this study, 80% of the patients had temporal bone fracture with 15 cases of longitudinal fracture and 1 case of transverse fracture. Most cases with longitudinal temporal bone fracture resulted in conductive hearing loss, which is compatible with previous study. 11 We focused on patients with ossicle-chain injury after trauma who had persistent conductive hearing loss for at least 3 months. I-S joint separation is the most common posttraumatic abnormality.1-3 Meriot et al 3 reported 2 possible mechanisms. First, the incus has only tenuous suspension between the anchored malleus and stapes, and the I-S joint is a fragile enarthrosis that is easily movable after injury. Second, both the malleus and stapes have muscle tendons fixed on the cochleariform process and pyramidal eminence, respectively. During trauma, the resulting muscle contraction leads to the rotation of the I-S joint. Ossicular discontinuity, hemotympanum, or eardrum perforation after trauma affect hearing transmission.
Hearing impairment and vertigo are 2 common symptoms in patients with head injury. 12 To repair conductive hearing loss, ossiculoplasty is performed. Tos 4 reported favorable prognosis for hearing after ossicular injury, with 13 of 16 patients showing an improvement within 30 dB after ossiculoplasty (using incus interposition, polyethylene prosthesis, or Schuknecht’s steel-gelfoam prosthesis). Regarding the differences between prosthesis and autologous incus, the advantages of ossicular autografts are easy availability, low cost of preparation, high biocompatibility, and low extrusive rate.8,13 Spector et al 14 reported that 85% of the cases exhibit significant improvement after surgery, and the use of prosthesis resulted in more stable hearing results than ossicular reposition/interposition in the long-term (>2 years) follow-up. Moreover, titanium protheses demonstrated favorable acoustic characteristics, especially at high frequencies (2.0 and 3.0 kHz), for hearing restoration, 15 and the mass of titanium is lower, which causes sound to be transferred up to 4.0 kHz. 15 Therefore, Wu et al 8 used the hearing result at the high frequency of 4.0 kHz for representing the material efficacy for autologous ossiculoplasty and described that 90% of the patients using autografts had closure of the ABG within 20 dB, with a similar effect of titanium, especially in terms of high-frequency improvements at 2-year follow-up. 8 Even more, Sterrer and Loader 16 retrospectively analyzed large sample sizes of 115 patients with COM or cholesteatoma receiving incus interposition graft (N = 62) or PORP (N = 53), and demonstrated incus autograft may have better outcomes than PORP in specific frequencies of 0.25, 1.0, 2.0, and 3.0 kHz. In our study, both the autologous incus and titanium prosthesis groups showed significant hearing benefits in terms of the AC and ABG at 4.0 kHz and the 4-frequency averages, indicating that the material efficacy was similar in the 2 groups.
Consistent with previous studies,8,17 we used a Glasgow benefit plot to illustrate the hearing improvement in the operative ear and compared with that in the nonoperative ear. In Figure 1, each line represents a different patient. The length of the line represents the change in AC thresholds and the arrow show the direction of change. Both the titanium (White) and autologous groups (Black) had favorable hearing outcome after surgery. Also, most of the patients recovered the hearing compared to the level of nonoperative ear (Gray square). The results showed these 2 groups have similar hearing outcome.
Regarding the symptom/sign of dizziness/nystagmus, posttraumatic vertigo may be caused by head concussion, and vestibulocochlear involvement should be examined to rule out perilymph fistula. 13 Hough and Stuart 2 reported that 13% of patients with middle ear injury after an accident had severe vertigo. However, this symptom subsided within 3 weeks without obvious vestibular damage. In an animal experiment, Schuknecht and Davison 12 demonstrated that positional nystagmus may persist after head injury due to the rupture of the membranous labyrinth of the utricle and saccule or degeneration of the macula of the saccule. Positional nystagmus was found in 25% of the patients with dizziness after trauma and in 50% of the patients with longitudinal fractures of the temporal bone. 18 In our study (Table 1), 50% of the patients had vertigo, and 15% of the patients had BPPV with longitudinal fractures of the temporal bone. These diverse findings highlight the difference in the mechanisms or severity of head injury. Some patients may have head concussion causing temporarily vestibular symptoms and the others may have temporal bone fracture with vestibular injury triggering persistent vestibular symptoms.
Furthermore, our study showed that patients with vertigo, BPPV, and temporal bone fracture presented a poor prognosis of the ABG gain (Table 4), indicating that these factors may be potential predictive factors of the hearing benefit. In previous studies, Spector et al 14 reported that the lesion sites may be predictive of the prognosis of surgical success. Lesions of incus dislocation or I-S separation have more favorable prognosis, but epitympanic trauma and fibrosis of the middle ear have poorer outcomes. Dornhoffer and Gardner 19 reported that among 185 patients who received Dornhoffer HAPEX PORP and TORP, mucosal fibrosis, wound drainage, revision ear surgery, and type of surgical procedure may predict the outcome of hearing. In summary, recent studies have predicted the prognosis from the surgical findings or middle ear condition. We demonstrated that vestibular symptom and sign may be a potential predictor for the hearing benefit from the surgery. These findings may help surgeon identify and explain the outcome preoperatively.
This study has some limitations. First, the sample size was small because of the rarity of traumatic ossicular injury. Second, some inherent bias may exist because the materials used were selected by surgeons. Finally, the postoperative follow-up duration may not be sufficiently long to assess the complications and hearing influences of different materials, impeding the prediction of long-term outcome. Further studies are still needed to address these issues.
Conclusion
Complete examination and treatment are crucial for traumatic head injury, especially in patients with ossicular injury. Ossiculoplasty with both titanium prosthesis and autologous materials presented favorable hearing recovery in terms of the AC and ABG. Vertigo, BPPV, and temporal bone fracture may be potential predictors of hearing benefit after ossiculoplasty. These findings can help physicians identify and communicate the possible outcome to the patient before surgery. In this small study, there was 1 additional case of BPPV in the group with poorer hearing outcomes. While this was statistically significant, we caution the reader about drawing significant conclusions from these results. Further study is warranted to better understand this association.
Footnotes
List of Abbreviations
I-S: Incudostapedial
I-M: Incudomallear
HRCT: High-resolution computed tomography
PORP: Partial ossicular replacement prosthesis
TORP: Total ossicular replacement prosthesis
ABG: Air-bone gap
COM: Chronic otitis media
AC: Air conduction
BC: Bone conduction
BPPV: Benign paroxysmal positional vertigo
Author Contributions
Chien, Chen-Yu: data collection, analysis and interpretation, and manuscript writing and revision; Tai, Shu-Yu: discussion and manuscript revision; Chan, Leong-Perng: discussion and manuscript revision; Wang, Hsun-Mo: discussion and manuscript revision; Chang, Ning-Chia: discussion and manuscript revision; Wang, Ling-Feng: discussion and manuscript revision; Ho, Kuen-Yao: discussion and manuscript revision; Li, Kuan-Hui: data collection, data interpretation, and manuscript revision.
Data Availability Statement
The data presented here are available upon reasonable request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Kaohsiung Medical University Hospital (KMUH110-0M51) and Ministry of Science and Technology (MOST 108-2314-B-037-087).
Ethical Approval
This study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (IRB number: KMUHIRB-E(II)-20210112).