
Abstract
Background:
Investigate the ability of frailty status to predict post-surgical outcomes in patients with cutaneous malignancies of the scalp and neck undergoing flap reconstruction.
Methods:
National Surgical Quality Improvement Program database was used to isolate patients with cutaneous malignancies of the scalp and neck who underwent surgical resection between 2015 to 2019. Univariate and multivariate analyses were performed to determine if frailty score correlated with negative post-operative outcomes. Receiver operating characteristic (ROC) curves allowed testing of the discriminative performance of age versus frailty.
Results:
This study demonstrated an independent correlation between frailty and major complications as well as non-home discharge. In ROC curve analysis, frailty demonstrated superior discrimination compared to age for predicting major complications.
Conclusion:
Our study demonstrated an association between increasing frailty and major complications as well as the likelihood of a non-home discharge. When compared to age, frailty was also shown to be a better predictor of major complications.
Keywords
Introduction
Cutaneous malignancies of the scalp and neck are generally comprised of basal cell carcinomas and squamous cell carcinomas, though they may also include melanoma, Merkel cell carcinoma, and more rare etiologies. 1 The primary risk factor for developing these malignancies is exposure to ultraviolet radiation. 1 Surgical excision with adequate margins is usually the mainstay of treatment for cutaneous malignancies of the scalp and neck.1,2 This often results in large defects which are not amenable to primary closure, especially with resection of scalp disease, thus requiring additional surgical interventions such as skin grafting, local flap reconstruction or free flap reconstruction. Risk factors for post-operative complications or extended length of hospital stay include poor immune function, exposure to pre-and/or postoperative radiation, or placement of titanium mesh during surgery. 3 It has been our experience that elderly patients with large cutaneous defects of the scalp, especially those requiring calvarial bone resection and free-tissue transfer, often have poor outcomes.
There is a growing body of literature utilizing the modified frailty index 5 (mFI-5) to predict postoperative outcomes for patients undergoing various types of surgery using data collected for the American College of Surgeons prospective registry, the National Surgical Quality Improvement Program (NSQIP).4-6 Age can be a useful predictor of postoperative outcomes but has shown to be worse than mFI-5 in some studies. 7 When mFI-5 has been studied specifically in microvascular reconstruction of the head and neck it has been shown to be a significant predictor of risk of longer hospitalization, reoperation, mortality, and unplanned readmission.8,9 To our knowledge, this is the first study to assess the ability of frailty scoring to predict postsurgical outcomes following the resection of cutaneous malignancies of the scalp and neck requiring flap reconstruction.
Materials and Methods
Data Source
The National Surgical Quality Improvement Program (NSQIP) database was queried for patients with cutaneous malignancies of the scalp and neck who underwent flap reconstruction between 2015 to 2019. The NSQIP database contains data collected from institutions employing a uniform protocol by trained surgical reviewers across many institutions. 10 NSQIP prospectively collects data from hundreds of sites, collects information on more than 200 variables, and is Health Insurance Portability and Accountability Act–compliant. 7 This is ideal for investigating patients with comorbid conditions used to create frailty indices, however, the veracity of each individual data point cannot be confirmed. The present study was performed under the data user agreement of the ACS with University of New Mexico Hospital and was approved and considered exempt from continuing review by the Institutional Review Board at the University of New Mexico.
Patient Population and Baseline Characteristics
The following Current Procedural Terminology (CPT) and International Classification of Diseases (ICD)-9 and ICD-10 codes that were used to identify patients who met study criteria; 11620-1 (Excision, malignant lesion, scalp, neck, hands, feet, genitalia; lesion diameter 0.6-1.0 cm), 11622-3 (Excision, malignant lesion, scalp, neck, hands, feet, genitalia; lesion diameter 1.1-3.0 cm), 11624 (Excision, malignant lesion, scalp, neck, hands, feet, genitalia; lesion diameter 3.1-4.0 cm), 11626 (Excision, malignant lesion, scalp, neck, hands, feet, genitalia; lesion diameter over 4.0 cm), 20969 (Bone graft with microvascular anastomosis; other bone graft), 15756 (Microvascular muscle or myocutaneous free flap), 15757 (Microvascular free skin flap), 15758 (Microvascular free fascia flap), 15734 (Muscle, myocutaneous, or fasciocutaneous flap; trunk), 15740 (Flap; island pedicle), 173.40 (Malignant neoplasm of bone, connective tissue, skin, and breast), C43.4 (Malignant melanoma of scalp and neck), C4A.4 (Merkel cell carcinoma of scalp and neck), C44.40 (Unspecified malignant neoplasm of skin of scalp and neck), C44.41 (Basal cell carcinoma of skin of scalp and neck), C44.42 (Squamous cell carcinoma of skin of scalp and neck), and C44.49 (Other specified malignant neoplasm of skin of scalp and neck).
CPT codes were used to initially identify a pool of patients who underwent surgery for malignancies of the scalp, neck, hands, feet, and genitalia that required a local, pedicled, or free flap reconstruction. ICD-9 and ICD-10 codes were then used to further narrow down the study population to those with scalp and neck malignancies. Our original intention was to study frailty in patients with scalp malignancies, but the ICD 9 and 10 codes combine malignancies of the neck and scalp. We had to combine these groups but suspect, given the relative ease in closing neck as opposed to scalp defects, that most of these cases represent scalp malignancies. The baseline study population characteristics included age, sex, race, Hispanic ethnicity, smoking status, functional status, and operative time. Patient co-morbidities evaluated included diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), hypertension requiring medication, congestive heart failure (CHF), dyspnea, disseminated cancer (defined by the NSQIP as multiple metastases indicating that the cancer is widespread), an open wound, steroid use, weight loss (substantial unintentional loss in body weight [>10%]), bleeding disorders, preoperative transfusion, and preoperative sepsis/septic shock/systemic inflammatory response syndrome (SIRS). 7
Modified Frailty Index-5
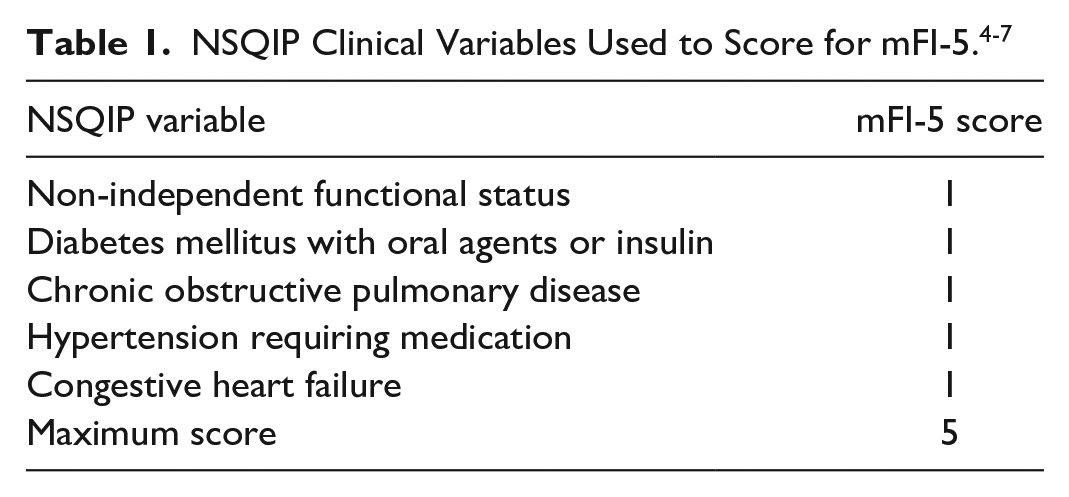
We used the modified frailty index-5 (mFI-5) as a measure of frailty based on the growing body of literature demonstrating mFI-5 as a predictor of postoperative complications in patients undergoing major surgery. 7 The mFI-5 score is easily calculated for each patient with 1 point given each for the presence of DM, hypertension, CHF, COPD, and dependent functional status (Table 2). Initial NSQIP input data for each of these 5 patient comorbidities was confirmed. This showed that 178 of 178 patients had initial input data for DM, COPD, CHF, hypertension, and 177 of 178 patients had initial input data for functional status. 11 The maximum mFI-5 score is 5 and based on previously established standards, a score of 1 is considered “prefrail,” 2 is “frail,” and 3 or more is “severely frail (Table 1).” 11
Outcome Measures
Outcome measures were 30-day post-operative mortality, major or life threatening (Clavien-Dindo grade 4) complications, unplanned reoperation, discharge to a non-home destination, and length of hospital stay (LOS). Complications specific to post flap reconstruction, such as anastomotic thrombosis or hemorrhage are not well captured by the NSQIP database and therefore not included in our study. Based on previous studies, major complications were defined as patients experiencing 1 or more of the following: prolonged intubation of 48 hours or more, unplanned reintubation, sepsis/septic shock, deep vein thrombosis/thrombophlebitis, pulmonary embolism (PE), coma, cerebrovascular accident/stroke with neurological deficit(s), myocardial infraction (MI) or cardiac arrest requiring cardiopulmonary resuscitation (CPR), surgical site infection (superficial/deep/organ space), wound disruption/dehiscence, acute renal failure, and pneumonia. 7 The Clavien-Dindo classification of surgical complications is based on the type of therapy needed to correct the complication and is well established in the general surgery literature. 12 Clavien-Dindo grade 4 complications include life threatening adverse events requiring ICU management, such as septic shock, acute renal failure, PE, MI or cardiac arrest requiring CPR, and ventilation for longer than 48 hours. Mean LOS and 75th percentile LOS was calculated in SPSS using total length of hospital stay collected in NSQIP database for each patient.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics ver. 27.0 (IBM Co., Armonk, NY, USA). The effect of mFI-5 on postoperative complications was measured by univariate analyses using simple logistic regression and performed on all outcome measures. A multivariable logistic regression, controlling for age, sex, race, Hispanic ethnicity, and operative time, was used to define the discriminative ability of mFI-5. Effect sizes are presented as odds ratios (OR) with associated 95% confidence intervals (95% CIs). Receiver operating characteristic (ROC) curve analysis was also performed to investigate whether frailty or age is a better predictor of post-operative complications. Curves were compared using DeLong’s test designed for empiric ROC curve comparison. For all purposes, a P-value of <.05 was considered statistically significant.
Results
Study Population Characteristics
There were 178 patients that met inclusion criteria for this study. Characteristics of the study population are presented in Table 2. The mean age was 68 years old with a range of 26 to over 89+. A large majority (78%) were male. Hypertension was the most frequently observed comorbidity (54.5%), followed by diabetes mellitus (19.7%) and open wound infection (19.6%). Additionally, 4.5% of patients were functionally dependent (partially or completely) at initial presentation defined as the patient needing some assistance with activities of daily living within the last 30 days (partially dependent) or requiring complete assistance with activities of daily living (completely dependent). The frailty distribution analysis showed that 37.6% were not frail, 38.8% were prefrail, 20.8% were frail, and only 4 (2.2%) were severely frail. Overall postoperative 30-day mortality was 1.7% and reoperation occurred in 9.6% of patients. The most common postoperative complication was superficial surgical site infection (5.1%), followed by wound disruption (2.2%), deep surgical site infections (1.7%), and deep vein thromboses (1.7%); 85.4% of patients were discharged home and 12.4% were sent to a non-home facility or expired. LOS ranged from 0 to 54 days, with a mean of 3.31 days and a 75 percentile LOS of greater than 6 days.
Descriptive Characteristics of Patients Extracted Based on CPT, ICD-9, and ICD-10 Codes From the NSQIP Database.
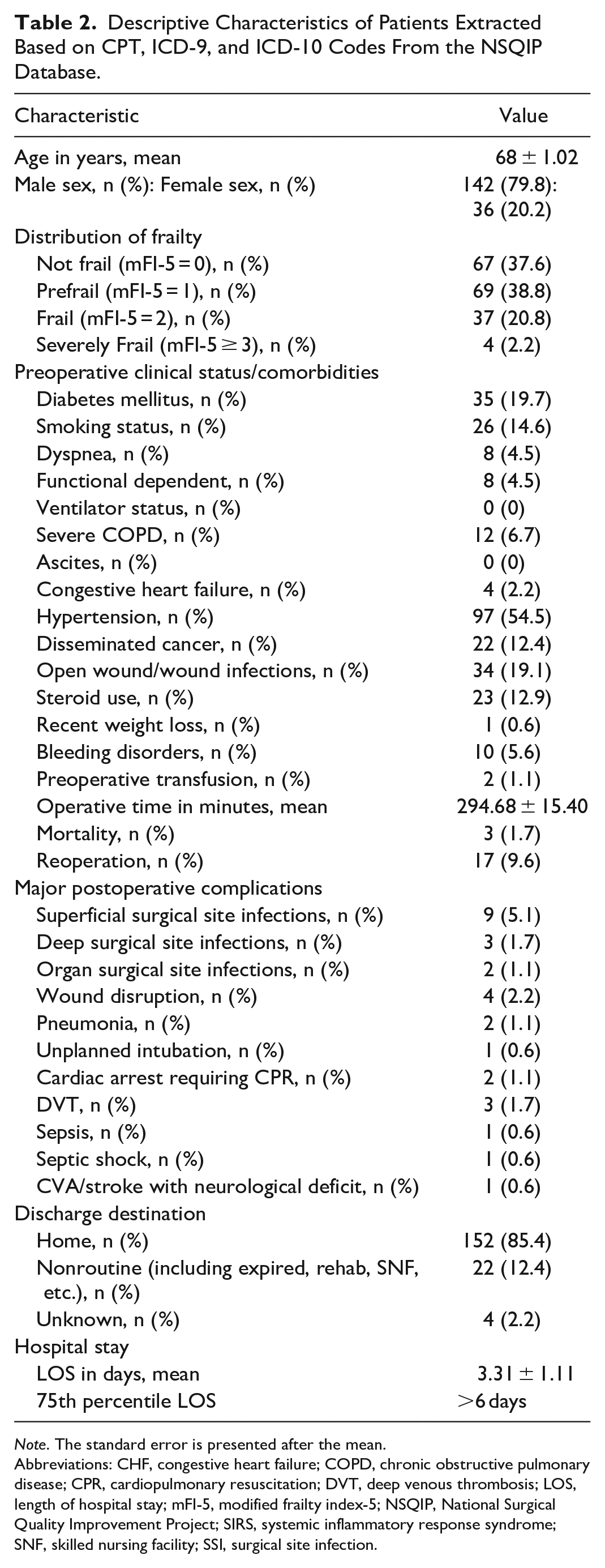
Note. The standard error is presented after the mean.
Abbreviations: CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CPR, cardiopulmonary resuscitation; DVT, deep venous thrombosis; LOS, length of hospital stay; mFI-5, modified frailty index-5; NSQIP, National Surgical Quality Improvement Project; SIRS, systemic inflammatory response syndrome; SNF, skilled nursing facility; SSI, surgical site infection.
Univariate Analysis of Frailty Status on Surgical Outcomes
Univariate analysis demonstrated that frailty status (based on mFI-5 score) was associated with major complications and non-home discharge, as determined by regression analysis and increasing odds ratios (Table 3). Frailty was not shown to be a predictor of mortality, Clavien-Dindo grade 4 complications, reoperation rates, or a patient having a greater than 75th percentile length of hospital stay in the selected patient population.
Univariate Analysis for Frailty Status (mFI-5 Score) on Outcomes After Surgery in Patients With Cutaneous Cancers of the Head and Neck Requiring Flap Reconstruction From NSQIP Database 2015 to 2019.
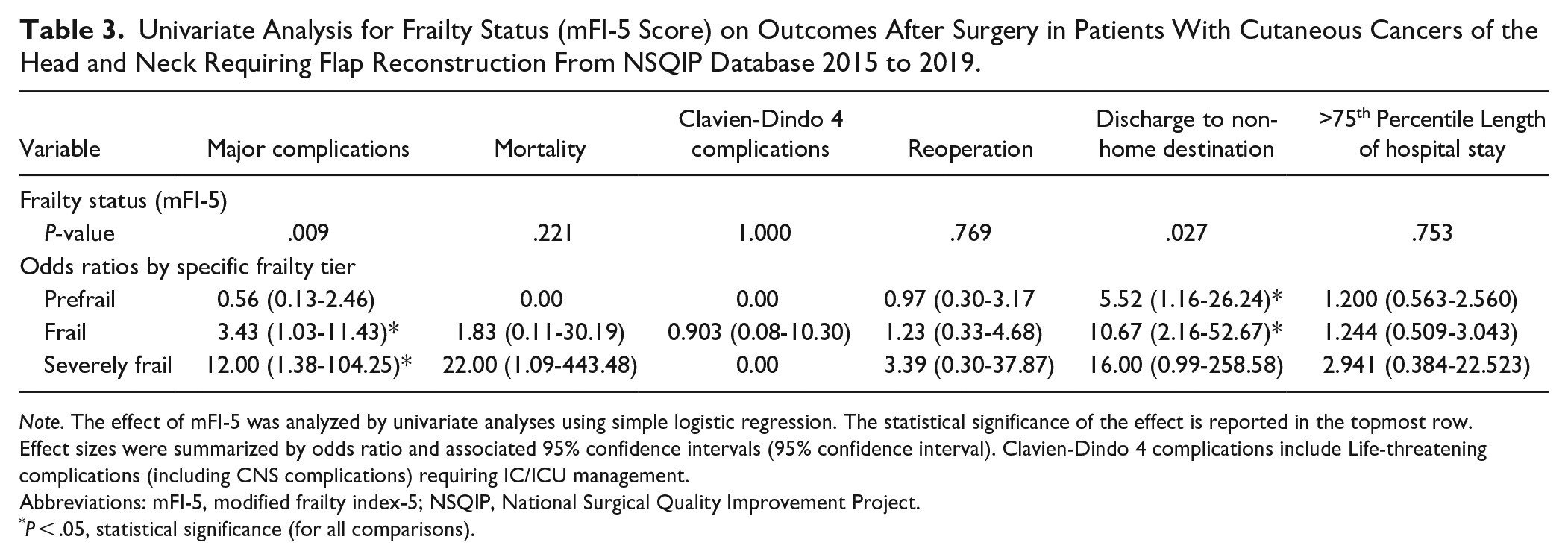
Note. The effect of mFI-5 was analyzed by univariate analyses using simple logistic regression. The statistical significance of the effect is reported in the topmost row. Effect sizes were summarized by odds ratio and associated 95% confidence intervals (95% confidence interval). Clavien-Dindo 4 complications include Life-threatening complications (including CNS complications) requiring IC/ICU management.
Abbreviations: mFI-5, modified frailty index-5; NSQIP, National Surgical Quality Improvement Project.
P < .05, statistical significance (for all comparisons).
Multivariate Analysis of Frailty Status on Surgical Outcomes
Multivariable regression analysis revealed frailty status to be an independent predictor of major complications (P = .024) and non-home discharge (P = 0.039). For major complications, no specific tier of frailty was statistically significantly predictive on its own. However, frail patients were more likely to have a non-home discharge when compared to all other categories (OR frail: 30.59 (2.45-358.54), P = .008) (Table 4).
Multivariate Analysis for Frailty Status on Major Complications and Discharge to a Nonhome Destination After Surgery in Patients With Cutaneous Cancers of the Head and Neck Requiring Flap Reconstruction From NSQIP Database 2015 to 2019.
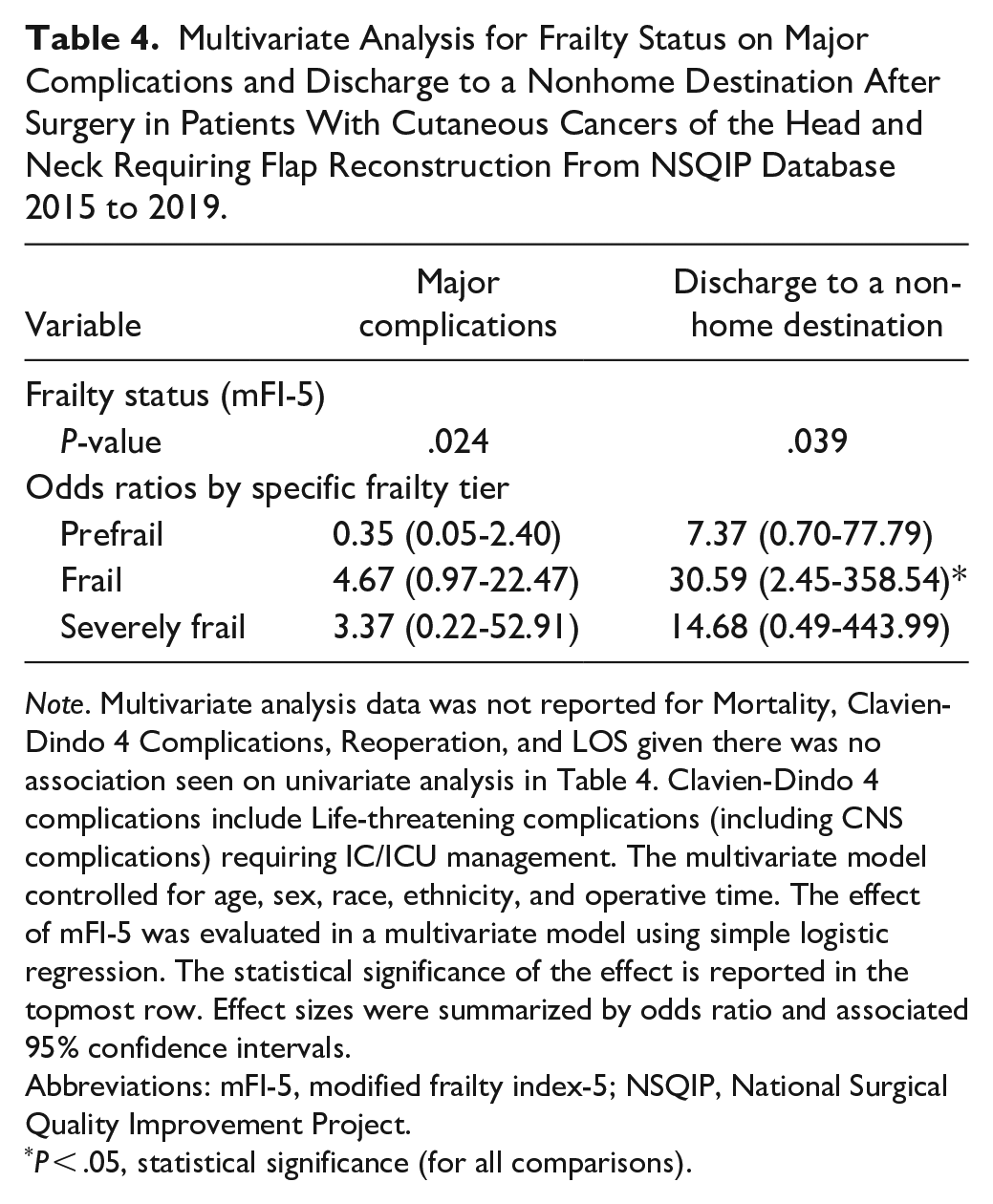
Note. Multivariate analysis data was not reported for Mortality, Clavien-Dindo 4 Complications, Reoperation, and LOS given there was no association seen on univariate analysis in Table 4. Clavien-Dindo 4 complications include Life-threatening complications (including CNS complications) requiring IC/ICU management. The multivariate model controlled for age, sex, race, ethnicity, and operative time. The effect of mFI-5 was evaluated in a multivariate model using simple logistic regression. The statistical significance of the effect is reported in the topmost row. Effect sizes were summarized by odds ratio and associated 95% confidence intervals.
Abbreviations: mFI-5, modified frailty index-5; NSQIP, National Surgical Quality Improvement Project.
P < .05, statistical significance (for all comparisons).
Receiver Operating Characteristic Curve Analysis of Age and mFI-5 for Major Complications and Non-Home Discharge
Frailty was a better predictor (mFI-5) of major complications (AUC = 0.662; 95% CI 0.509-0.816; P = .038) on ROC curve analysis as compared to age. In fact, age was not a significant predictor of major complications in this study (AUC = 0.553 [0.425-0.681], P = .420) (Figure 1). For non-home discharge, both frailty and age were equally predictive (Figure 2).
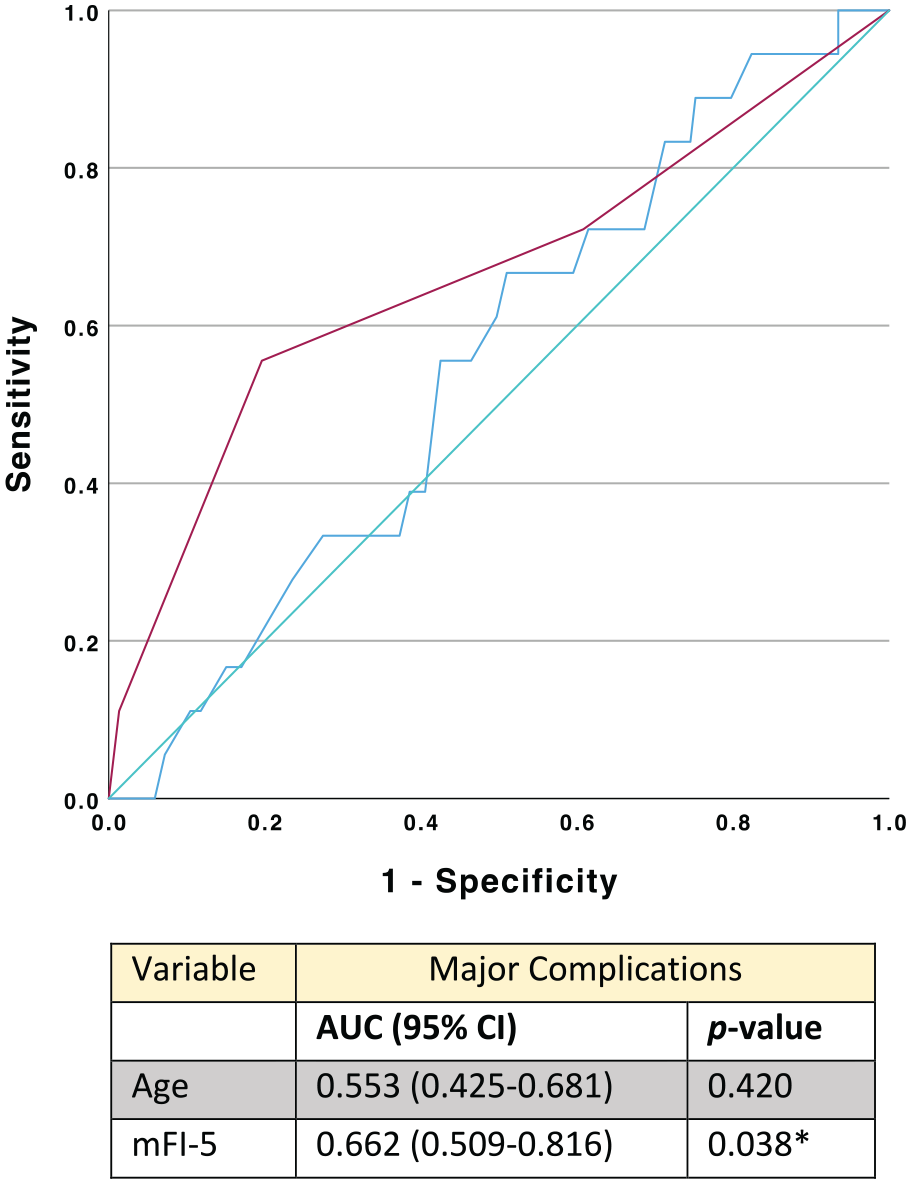
ROC curve analysis of age versus mFI-5 for postoperative major complications. (A) Receiver operating characteristic (ROC) curve analysis. (B) Comparison of areas under the curve (AUC) of mFI-5 and age for major complications. Blue line = Age, red line = MFI-5, and green line = reference.
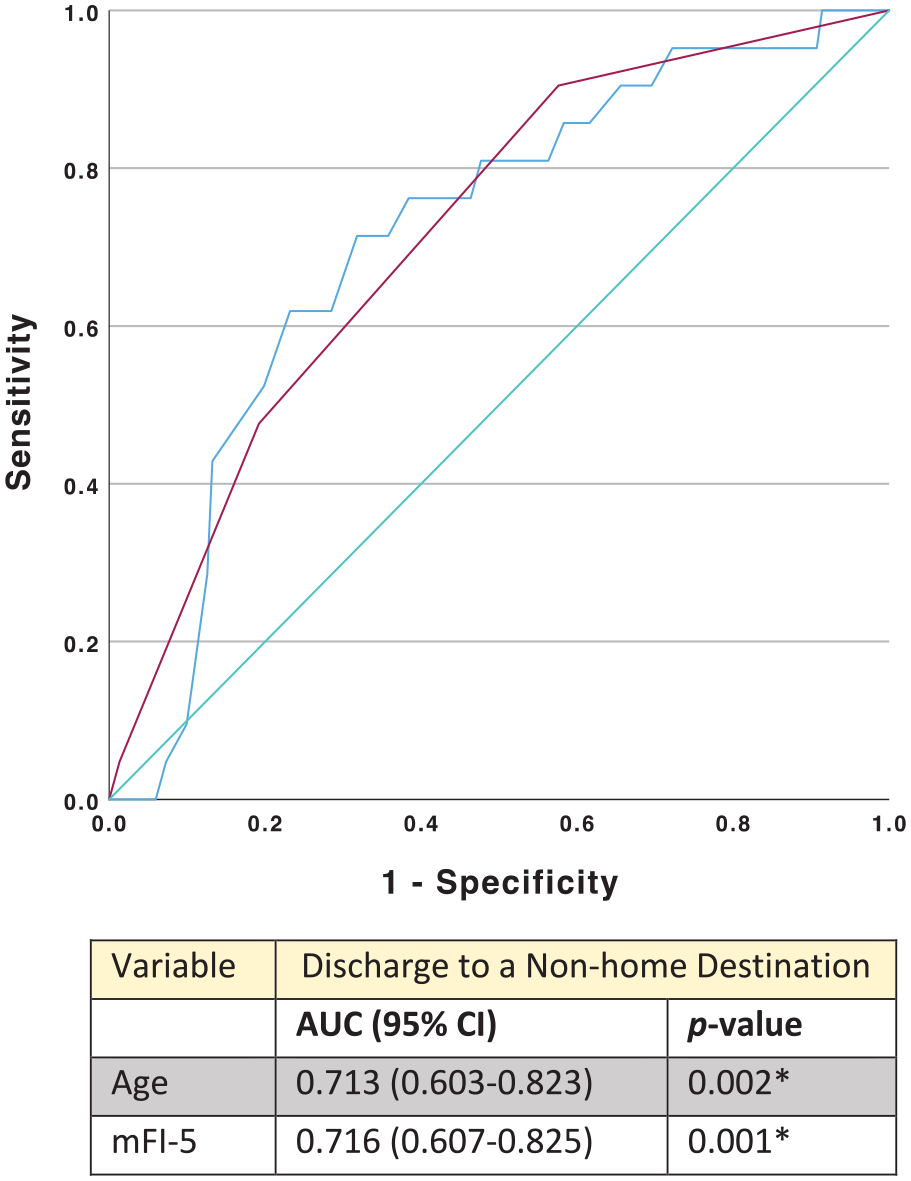
ROC curve analysis of age versus mFI-5 for postoperative non-home discharge. (A) Receiver operating characteristic (ROC) curve analysis. (B) Comparison of areas under the curve (AUC) of mFI-5 and age for Discharge to a Non-home Destination. Blue line = Age, red line = MFI-5, and green line = reference.
Discussion
Scalp and neck malignancies present several unique challenges for surgeons. The convex shape of the cranium and the lack of distensible skin means that many defects require flap closure. While age is often an important factor in determining a patient’s suitability for surgery, there is an emerging body of literature that suggests frailty may be a better predictor of post-operative outcomes in some circumstances.8,9,13-15 Many elderly patients undergo major surgery without issue, while sometimes younger patients do very poorly.13-15 The use of mFI-5 frailty scoring allows clinicians to better assess a patient’s physiologic reserve compared to the use of age alone. The mFI-5 combines comorbidities that have long been associated with poor post-surgical outcomes into one scoring system to help physicians evaluate risk as opposed to attempting to assess the contribution of each comorbid condition individually. Our data demonstrated a convincing association between frailty and both major complications and non-home discharge. Our data also suggest that frailty is a better predictor of major post-operative complications than age in patients with cutaneous malignancies of the scalp and neck requiring local or free flap reconstruction. In this data set, age was in fact not predictive of major complications, as the confidence interval of the area under the curve (AUC) in ROC analysis for this model was 0.425 to 0.681. Whereas, the confidence interval of the AUC for mFI-5 in ROC analysis was 0.509 to 0.816, thus showing mFI-5 to be a better predictor of major complications than age based this analysis. However, the mFI-5 was equivocal to age when predicting non-home discharge.
This study has several limitations, not least of which is the relatively small sample size. NSQIP studies typically involve patient populations in the thousands, however, because our clinical question was so narrow, our data set was much smaller. This may explain why there were not impressive correlations between individual frailty categories and poor post-operative outcomes. Another possible limitation of the study is related to the use of large national databases. NSQIP only records postoperative outcomes within the first 30 days of surgery, therefore long-term outcomes are difficult to evaluate. In addition, NSQIP does not collect data on tumor size specifically, making it difficult to compare outcomes based on T stage. We also acknowledge there is a possibility our study population includes a small number of primary malignancies of the neck based on limitations inherent to the use of ICD codes to extract data from NSQIP. However, because these codes exclude the face and since it is relatively uncommon for primary malignancies of the neck to require local, pedicled, or free flap reconstruction, we feel confident our study population is comprised largely of scalp malignancies. Finally, this is a retrospective study of data collected in a prospective fashion and therefore may be subject to inherent selection bias.
Surgeons often emphasize mortality and major complications when counseling patients. However, many patients are more concerned about quality of life and are extremely motivated to avoid long term hospital or intermediate care stays. Surgical oncologists are often forced to grapple with this issue when helping patients make decisions about whether or not to undergo major surgery. Overall, our study suggests that frailty may be helpful in personalizing a patient’s risk assessment to help them decide whether or not surgery is appropriate in the context of their overall goals of care. Most convincingly, frailty was associated with non-home discharge, which could prove useful in preoperative counseling if this is an outcome a patient would like to particularly avoid. On multivariable modeling, the odds of a frail patient discharging to a non-home destination was thirty times higher than that of a non-frail patient. Frailty scoring, in addition to age, could be useful in counseling patients about the likelihood of being discharged home or to an intermediate care facility after surgery.
Based on our experience treating patients with scalp malignancies, we have noticed that some patients, particularly those who are frail and require calvarial bone resection, often exhibit a noticeable cognitive decline. While this could not be directly evaluated with NSQIP data, non-home discharge may serve as a surrogate marker for this observed outcome. Other scoring systems seen in the literature such as the Groningen Frailty Indicator (GFI) and Geriatric 8 (G8) frailty scores, may have the potential to further elucidate this question as they include inquiries into the patient's cognition.16,17 Additional studies comparing mFI-5 to these other frailty methods for predicting non-home discharge may be of utility.
As with any patient assessment tool, a major barrier to adoption is its ease of use in a clinical setting. In this case, mFI-5 is an ideal scoring measure as it can be calculated quickly by virtually any type of health care provider and, depending on one’s EMR, could potentially be generated by computer algorithm. For frail or severely frail patients, use of a frailty index could give a health care provider an additional tool to help guide a risk versus benefit discussion with patients who are considering surgery for removal of cutaneous scalp and neck malignancies. This could help facilitate a Best Case/Worst Case scenario discussion with patients to compare outcomes of having surgical intervention versus no intervention. This tool has been shown to be a potentially useful way for patients to understand specific risks of their procedure, such as need for admission to an intermediate care facility. 18 On the other hand, use of a frailty score could also allow surgeons to feel more confident about recommending surgery to older patients with low frailty scores, thus increasing access to surgical treatment in a group who may have been previously overlooked or who felt ambivalent about surgery due to older age. Given the limited sample size of this study, we recommend inclusion of frailty markers in informed consent discussion, but not their overemphasis. In addition, variables known to increase surgical risk, such as poor immune function, preoperative radiation, calvarial bone involvement, and tumor size and location must also be factored into patient counseling.19,20 Future studies could potentially combine frailty with disease specific risk factors to create an even better surgical risk assessment tool.
As the incidence of cutaneous skin malignancies continues to rise, so will the number of patients requiring surgical resection. 1 Therefore, continued development of fast and effective measures to help predict outcomes in this patient population is of great utility.
Conclusion
Our study demonstrates an association between increasing frailty and both major complications and non-home discharges following hospitalization for patients undergoing resection and flap reconstruction of cutaneous malignancies of the scalp and neck. In our study, age was not a predictor of major complications. This information may help guide pre-operative decision making for patients with cutaneous malignancies of the scalp and neck who are considering surgical treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.