
Abstract
Objective:
To review the literature and our institutional experience regarding the risk of meningitis in patients with spontaneous lateral skull base cerebrospinal fluid (sCSF) leaks awaiting surgical repair, and the roles of antibiotic prophylaxis and pneumococcal vaccination, if known.
Methods:
A retrospective chart review and systematic review of the literature was undertaken to identify the incidence of meningitis in patients with sCSF leaks awaiting surgical repair. Adults managed surgically for sCSF leaks at an academic tertiary care center over a 10-year period were included. Data was collected on receipt of prophylactic antibiotics and/or pneumococcal vaccines during the timeframe between diagnosis and surgical repair.
Results:
Institutional review identified 87 patients who underwent surgical repair of spontaneous leaks, with a 0% incidence of meningitis over a median duration of 2 months while awaiting surgery (mean 5.5 months, range 0.5-118 months). Eighty-eight percent of patients did not receive prophylactic antibiotics. No studies in the published literature demonstrated the impact of prophylactic antibiotics or pneumococcal vaccine on meningitis risk.
Conclusions:
There appears to be a low risk of meningitis among patients with lateral skull base sCSF leaks awaiting surgery for short durations (≤2 months), even in the absence of prophylactic antibiotics. There is a substantial gap in the published literature assessing the risk of meningitis and roles of antibiotics and vaccination in this patient population, indicating the need for large-scale study to conclusively elucidate the nature of this risk.
Introduction
Compared to their traumatic, infectious, iatrogenic, and congenital counterparts, spontaneous (idiopathic) lateral skull base cerebrospinal fluid (sCSF) leaks are a poorly understood entity. A number of etiologic factors may contribute to thinning and dehiscence of the cortical interface between the dura and the temporal bone (tegmen), including increased intracranial pressure, obesity, and obstructive sleep apnea (OSA).1 -7 There are significantly increased odds of obesity and OSA among patients with sCSF leak compared to control patient populations, and both OSA and obesity have been correlated with diffuse skull base thinning—a factor which may underlie the development of sCSF leak.8 -13 In a proportion of cases, a breach in the associated temporal lobe dura will lead to CSF leak and/or encephalocele development. Lateral skull base sCSF leaks often present with nonspecific symptoms that can obfuscate diagnostic decision making, including hearing loss, aural fullness, tinnitus, otalgia, vertigo/dizziness, and headache. On examination, patients may exhibit clear otorrhea—especially subsequent to placement of a myringotomy tube—rhinorrhea, or unilateral middle ear effusion.14 -16 Rarely, patients may suffer meningitis as the presenting symptom of a previously undiagnosed CSF leak.
Pneumococcal meningitis is a rare but devastating complication of skull base CSF leaks. The incidence of meningitis in anterior skull base CSF leaks has been well-studied, and is accepted to be in the range of 10% to 36.5%. 17 In contrast, the risk of meningitis in patients with spontaneous lateral skull base CSF leaks is not well-established. It is generally agreed upon that operative closure/ repair of the dural defect and CSF leak reduces the risk of meningitis. 18
Current practice regarding antibiotic prophylaxis prior to operative repair of sCSF leaks extrapolates upon data from anterior skull base leaks, which largely suggest lack of benefit19 -24; though considerable practice variation likely exists.18,25 With streptococcus pneumoniae being the most common causative organism of meningitis complicating skull base CSF leaks, routine pneumococcal vaccination has been recommended by the CDC as an additional prophylactic measure in individuals with CSF leak.26 -29 The risk of meningitis and roles of antibiotic prophylaxis and pneumococcal vaccination in patients with sCSF leaks who are awaiting surgical repair have not been well-studied.
To address these questions, a systematic review of the literature and retrospective review of institutional data was undertaken. We aimed to: (1) evaluate the incidence of meningitis, and (2) assess the roles of prophylactic antibiotics and pneumococcal vaccination in reducing the risk of meningitis in patients with sCSF leaks awaiting operative repair. We hypothesized that a low proportion of patients would suffer meningitis in the time period between diagnosis and operative repair, regardless of antibiotic prophylaxis and pneumococcal vaccination.
Methods
The study was approved by our Institutional Review Board (IRB).
Search Strategy and Study Selection
The search methodology, study selection, and reporting employed in this study are in accordance with the Cochrane handbook and the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.30,31 An electronic search was conducted using the following databases: PubMed/MedLine, EMBASE, and the Cochrane Central Register of Controlled Trials. The search included all studies of patients with spontaneous lateral skull base CSF leaks published from January 1, 1946 to September 30, 2021. In addition to the electronic search, a hand search of the references from included articles was performed. An experienced librarian assisted with the literature search using the search strategy detailed in Supplemental Appendix 1.
Publications reporting the incidence of meningitis among patients with sCSF leaks who underwent surgical repair were included. The Patient, Intervention, Comparator, Outcome, Timing, Study design (PICOTS) framework was applied as follows for the systematic review:
Population
Adult patients with spontaneous lateral skull base CSF leak ± encephalocele(s).
Intervention
Surgical repair (any approach).
Comparator
No surgical repair.
Outcomes
Proportion of patients presenting with meningitis; prevalence of meningitis among patients awaiting surgery; rate of prophylactic antibiotic use; rate of pneumococcal vaccinations, or recommendations thereof; effect of prophylactic antibiotic use and/or vaccinations on meningitis incidence.
Timing
Meningitis occurring prior to surgical repair.
Study design
Randomized and non-randomized studies with n > 1.
Identified studies were screened independently by 2 reviewers (AEQ, EDR). Level 1 screening entailed a broad screen based on record titles and/or abstracts. A liberal accelerated process was adopted for Level 1 screening, whereby one reviewer was required to include a study, but 2 were required to exclude it. Studies deemed relevant based on initial title and abstract screen were obtained in full-text and underwent Level 2 screening in duplicate by the same 2 reviewers. Discrepancies were resolved by consensus or by involving a third team member (MJR).
Data Extraction, Analysis, and Bias Assessment
General study characteristics and outcomes data were extracted by one reviewer (AEQ). Outcomes data were independently verified by a second reviewer (EDR). Data extracted from included articles were: study country, design, total “n,” general patient demographics, symptom duration, history of meningitis, time observed prior to repair, repair approach, administration of antibiotics and pneumococcal vaccination, and leak recurrence. Data points not reported in individual studies are denoted by “-” in the included data tables.
Qualitative synthesis and descriptive statistics were employed to integrate the study results.
Internal validity of study design and conduct was assessed by 2 independent reviewers (AEQ, EDR). Study quality assessment was performed using the Newcastle-Ottawa Quality Assessment Tool for cohort studies, and the National Institutes of Health (NIH) Quality Assessment Tool for Case Series.32,33
Single Institution Retrospective Review
We queried the electronic medical record (EMR) for all patients who had undergone surgical repair of CSF leaks and/or encephaloceles at our institution from November 1, 2011 to October 31, 2021. Records were identified based on surgical procedures performed using the following current procedural terminology (CPT) codes: 62100, 62120, 62121. Corresponding patient records were individually screened, and only patients undergoing repair of spontaneous lateral skull base CSF leaks with or without the presence of encephalocele(s) were included. Patients were excluded if their leak had been traumatic or iatrogenic in origin, or occurred in relation to chronic otitis media (COM) or a congenital inner ear deformity (IED). Patients undergoing repair of encephalocele(s) in the absence of CSF leak were also excluded.
The majority of patients were diagnosed on the basis of a positive test for β2-transferrin on a fluid sample from the suspected leak, as well as imaging (CT and/or MRI) demonstrating the presence of a lateral skull base defect. However, in cases where fluid studies were negative or equivocal, if strong suspicion for a leak persisted based on clinical symptoms, the patient was diagnosed as such. All cases of sCSF leak were confirmed intra-operatively.
Data was extracted from the EMR pertaining to diagnoses of meningitis, antibiotics prescribed prior to surgery, and pneumococcal vaccine recommendations, in addition other applicable demographic and clinical variables.
Statistical Analysis
All statistics were performed using Stata version v15.1 (StataCorp, College Station, Texas). For the systematic review, qualitative review and descriptive statistics were used. For the institutional review, descriptive statistics (means, medians in cases of skewed data, and ranges) were used. T-tests and one-way ANOVA were used to compare means across groups. Logistic regression was used to assess for associations between recurrence rate and surgical technique. An alpha value of .05 was set as the threshold for statistical significance. Hypothesis testing regarding the impact of antibiotics and/or vaccines on the incidence of meningitis was not possible due to the lack of occurrences of the outcome of interest (meningitis).
Results
Institutional Retrospective Review
Eighty-seven instances of surgical repair of sCSF leaks were identified in 79 patients over a 10-year period. An additional 70 patients were excluded on the basis of non-spontaneous etiology of CSF leak (eg, traumatic, iatrogenic, associated with COM or congenital IED), anterior skull base CSF leaks, or repair of encephalocele in the absence of CSF leak. Demographic and clinical variables are summarized in Table 1.
Spontaneous Lateral Skull Base CSF Leak Patient Characteristics.
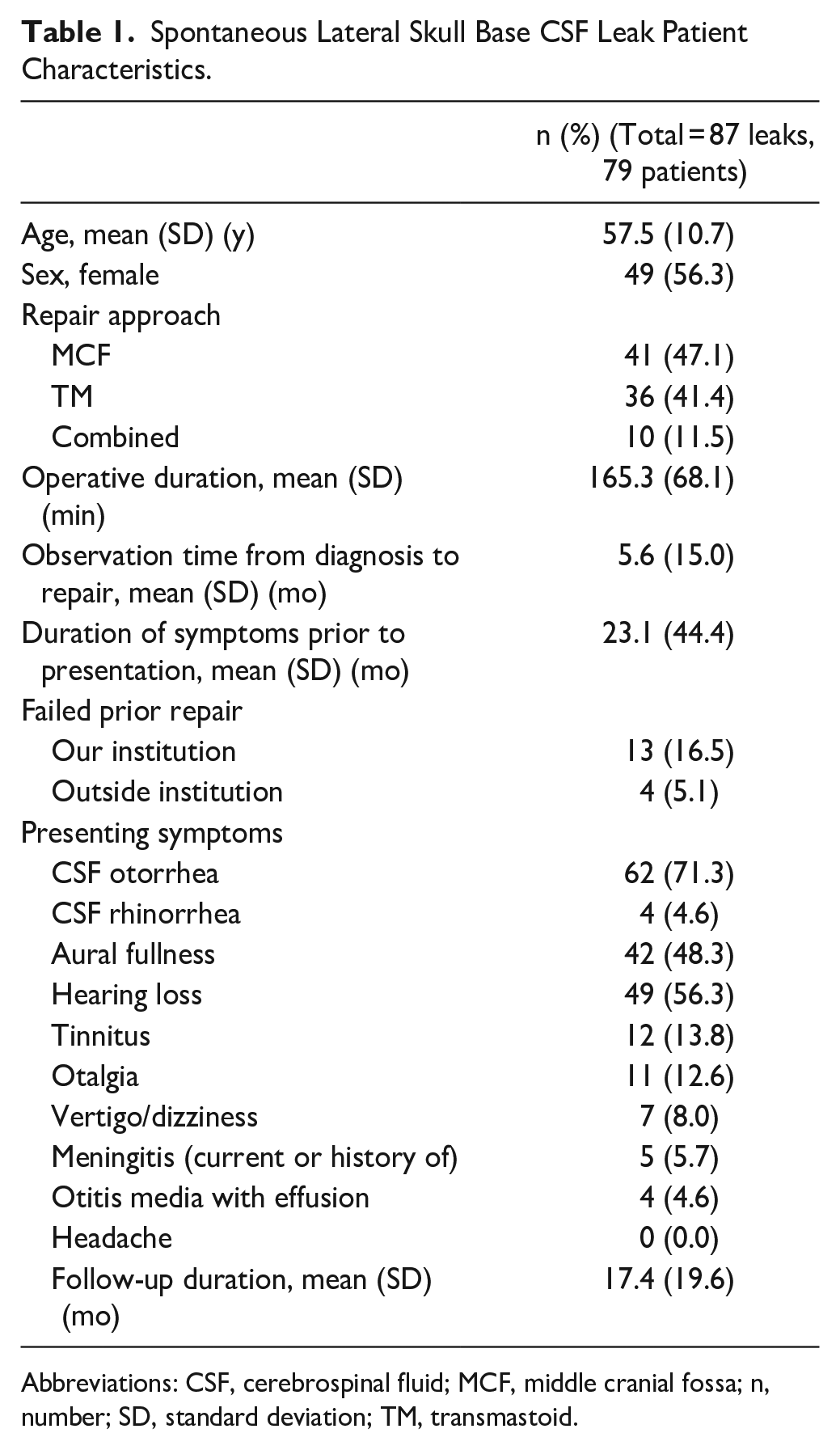
Abbreviations: CSF, cerebrospinal fluid; MCF, middle cranial fossa; n, number; SD, standard deviation; TM, transmastoid.
A total of 5 patients (5.7% of sCSF leaks) presented with or had a history of meningitis that had occurred prior to their diagnosis of sCSF leak. The duration of leak prior to the development of meningitis in these patients was not able to be ascertained. The median duration of symptoms prior to presentation was 6 months (mean 23.1 months; range, 0.5-240).
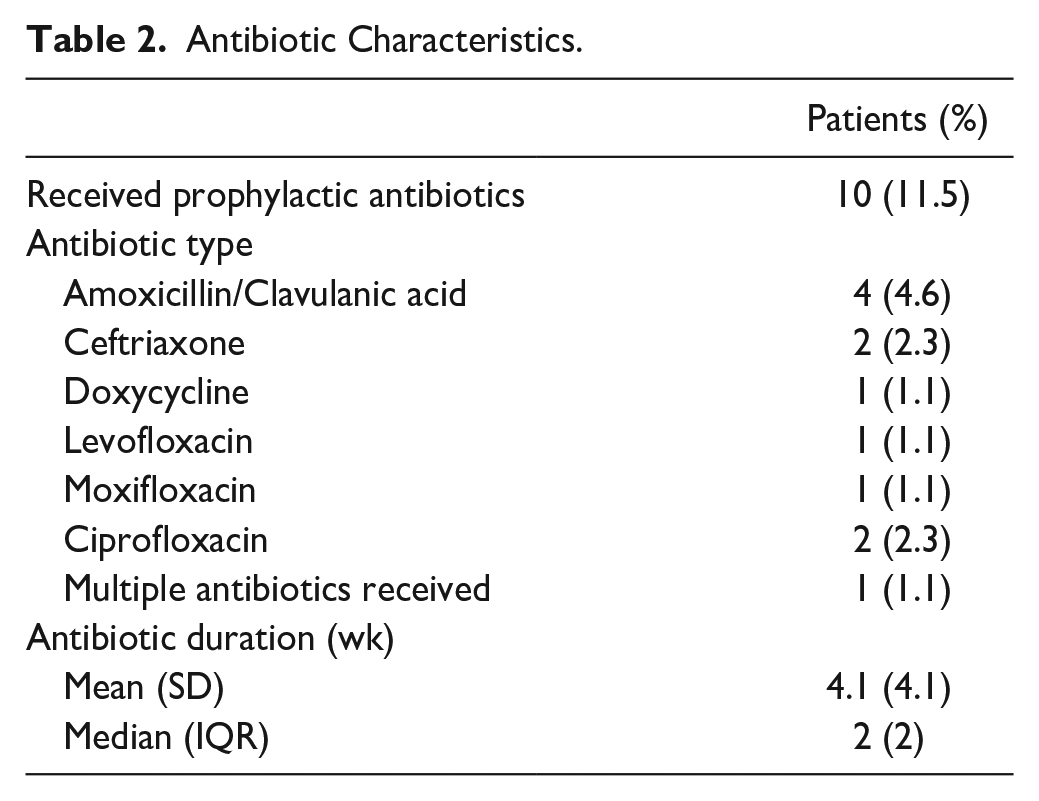
The median wait time from first presentation to surgery was 2 months (mean 5.6 months; range, 0.5-118) (Figure 1). Antibiotics were prescribed to patients awaiting surgery in 11.5% of cases (10 patients); the remaining 77 patients (88.5%) did not receive any prophylactic antibiotics during the period in which they awaited surgery. The median duration of prescribed antibiotics was 2 weeks (mean 4.1 weeks; range, 2-15). A variety of antibiotic agents were used (Table 2). Pneumococcal vaccination was documented to have been recommended to 26.19% of patients at the time of initial consultation. Actual rates of vaccination by patients could not be ascertained. No patient developed meningitis during the period of observation prior to surgery (0/40.6 people-years).
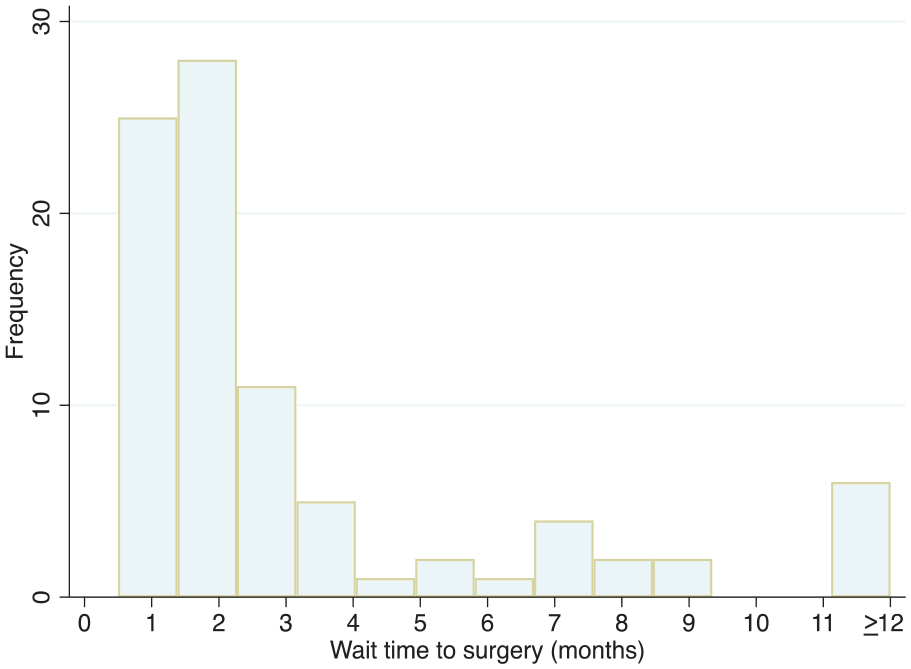
Distribution of wait times to surgery for lateral skull base CSF leak repair.
Antibiotic Characteristics.
The median duration of follow-up after surgical repair was 8 months (mean 17.4 months; range, 1-78).
Systematic Literature Review
Two hundred twenty-seven studies were identified after removing duplicates. Hand-search of bibliographies identified an additional 16 studies for review. A total of 30 studies met inclusion criteria for qualitative assessment (Figure 2). Pertinent characteristics of included studies are illustrated in Table 3.2,7,14 -16,34 -58
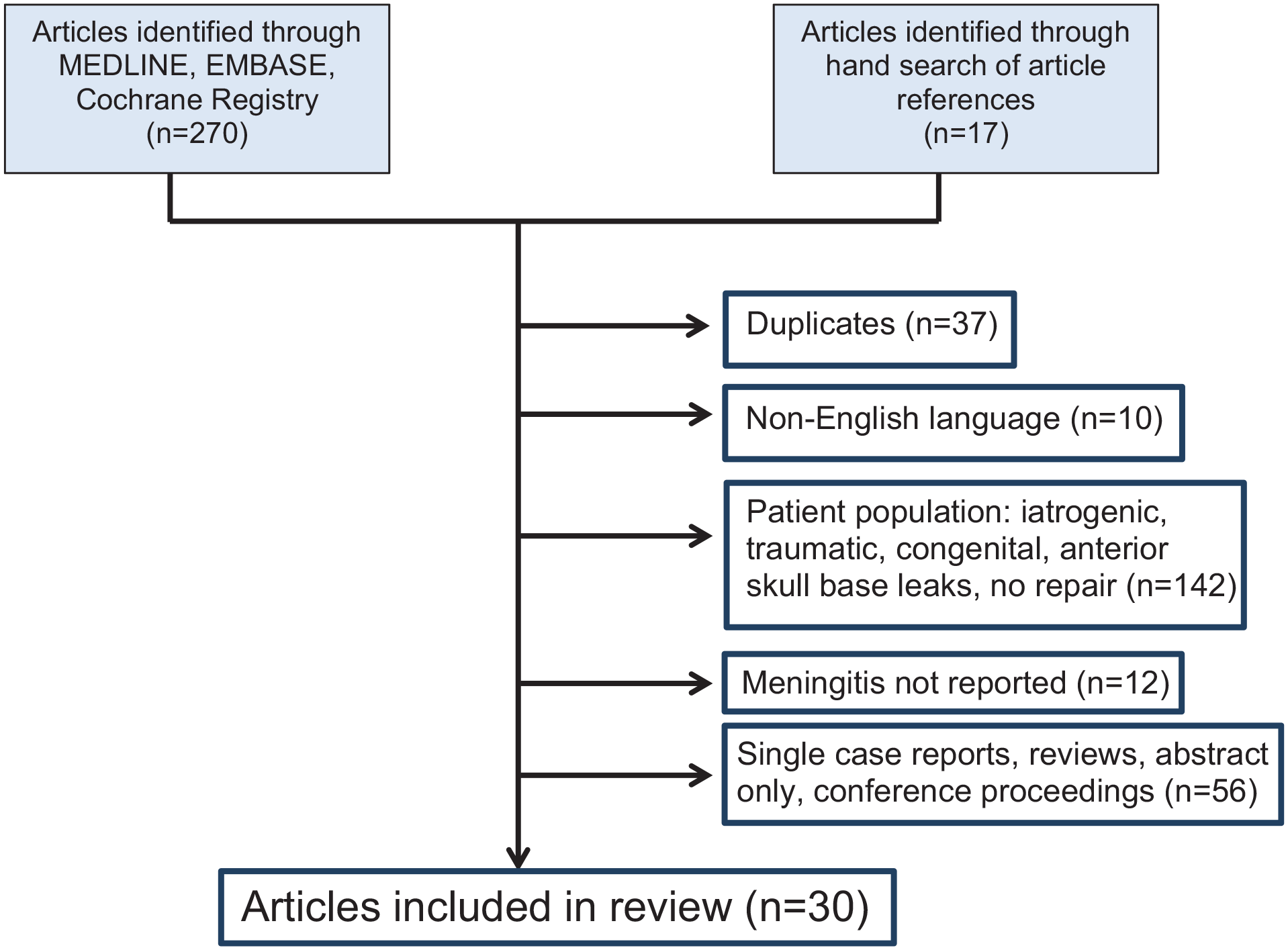
Search Strategy and Results of Systematic Review.
Systematic Review, Description of Included Studies.
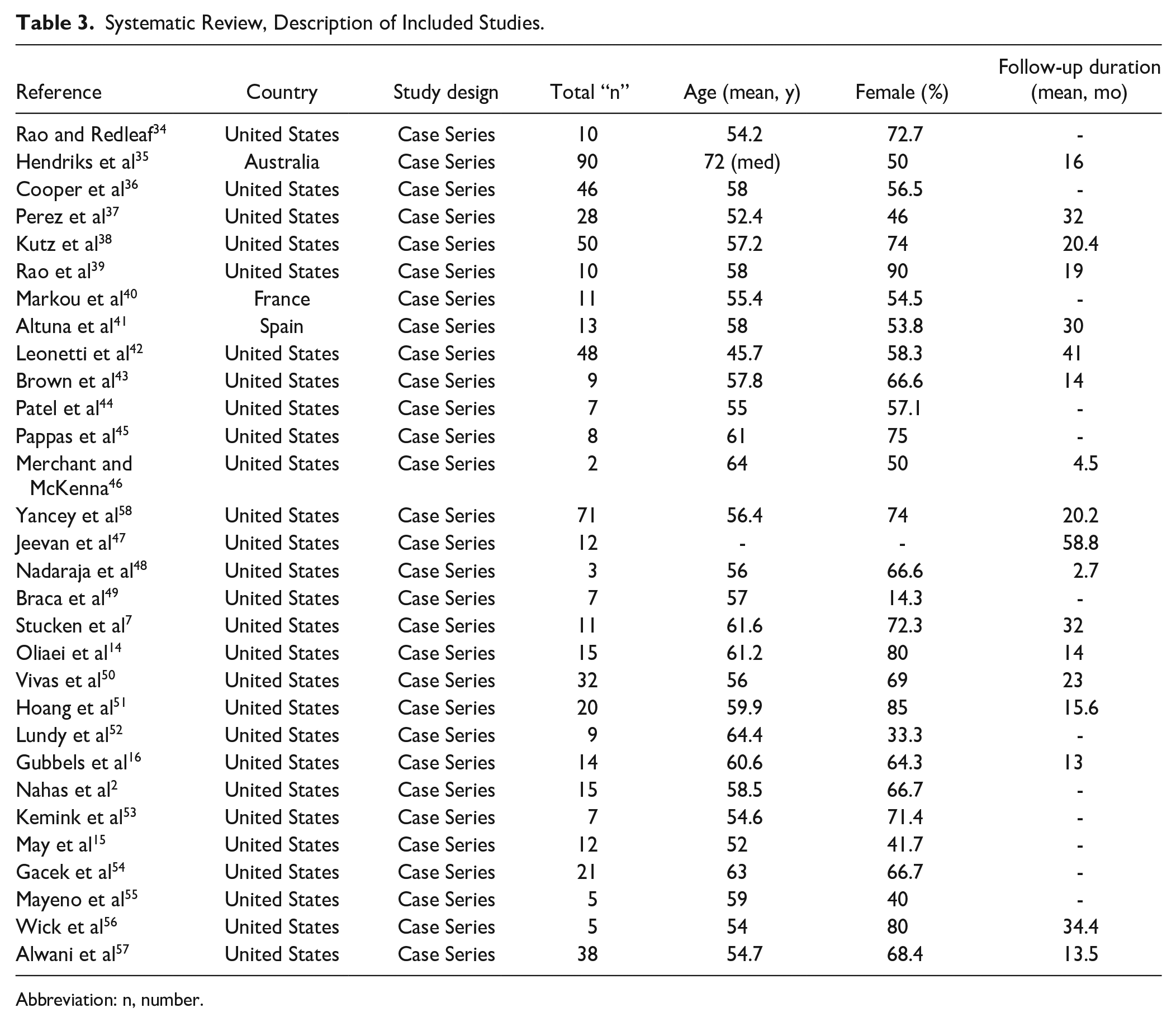
Abbreviation: n, number.
Two studies included a group of patients who underwent surgical repair as well as a group who were managed conservatively via observation without repair (due to either refusing surgery, or being deemed non-surgical candidates due to their age and/or medical comorbidities).34,35 In both, no cases of meningitis occurred in patients who were observed without surgical repair. It is not reported whether any or all of these patients received prophylactic antibiotics. The weighted mean observation time across these 2 studies, during which no cases of meningitis occurred, was 26.9 months.
Rao and Redleaf reported on a cohort of 10 patients (12 ears) with spontaneous temporal encephalocele and sCSF leak. Two patients (3 ears) were managed conservatively after refusing surgery, for a mean of 15.5 months (range, 15-16). Eight patients (9 ears) underwent surgical repair and were observed for a mean of 45.7 months (range, 4-132) prior to repair. In addition, at least 4 patients who underwent surgical repair (with 1 patient in their cohort having an uncertain outcome) continued to leak after surgical repair. No patient in either group developed meningitis during the observation period. 34
Hendriks et al reported on a cohort of 90 patients, of whom 38 underwent surgical repair, and 49 were managed conservatively for a mean of 12 months (range, 1-94) as they were deemed non-surgical candidates. Among the cohort who were managed conservatively, no patient developed meningitis. 35
Twenty-eight studies described cohorts of patients undergoing definitive surgical repair only, and reported the proportion of patients who presented either acutely or with a history of meningitis. None of these studies reported the duration of time that patients were observed between diagnosis and surgery, or the number of cases of meningitis that occurred during this period.
Across all 30 studies, the weighted mean proportion of patients who had a history of or presented with meningitis as their first sign of sCSF leak was 14.4% (range, 0%-63.6%). Seven studies reported the duration of patients’ self-reported symptoms prior to the diagnosis of CSF leak, with a mean duration of 41 months (range, 19.2-69.6) (Table 4).
Systematic Review, Spontaneous Lateral Skull Base CSF Leak Characteristics.
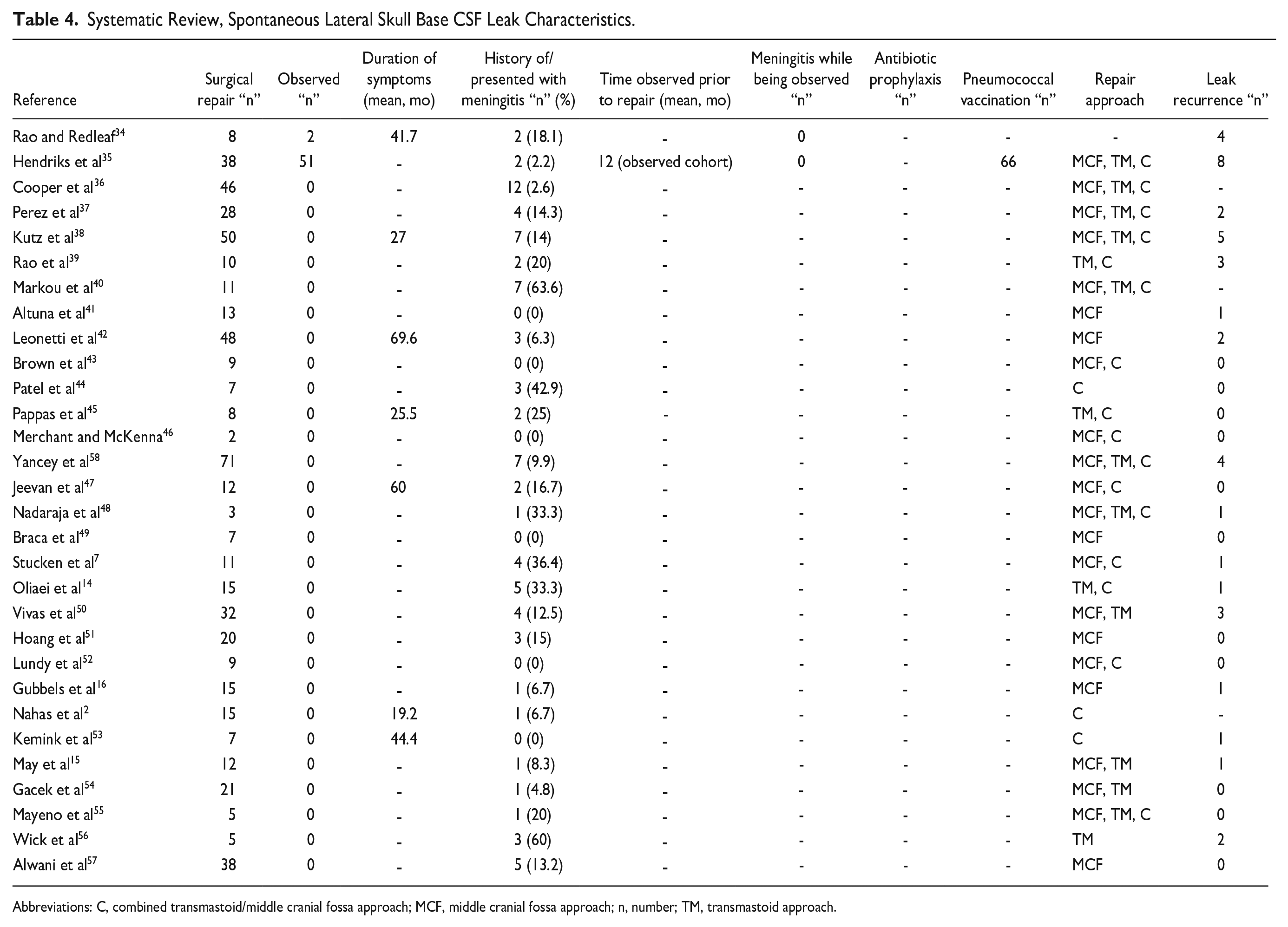
Abbreviations: C, combined transmastoid/middle cranial fossa approach; MCF, middle cranial fossa approach; n, number; TM, transmastoid approach.
No studies reported whether prophylactic antibiotics were routinely prescribed to patients following diagnosis (either prior to surgery, or as a part of conservative management in non-operated patients). One study reported rates of vaccination among patients awaiting surgery. 35 In this study, 73.3% of patients received immunizations. Specific immunizations received were not reported, but the authors described routinely recommending 7- and 23-valent pneumococcal vaccines.
Quality assessment of studies demonstrated the majority of included studies to be of fair (n = 14 studies) or good quality (n = 12 studies); a minority were deemed to be of poor quality (n = 3 studies). The most common shortcomings of included studies were no documented length of follow-up; unclear case definitions for spontaneous CSF leaks; and lack of demographic information for the study population (Supplemental Table 1).
Discussion
Our knowledge regarding the exact risk of meningitis and the value of prophylactic antibiotics and/or pneumococcal vaccination in patients presenting with sCSF leaks is limited, and largely extrapolated from literature on patients with anterior skull base CSF leaks. The potential benefit of prophylactic antibiotics in reducing the risk of meningitis must be balanced against the risk of developing resistant pathogenic organisms 24 ; the ramifications of such should not be understated.59 -61
Given that surgical repair is the generally-accepted management for patients with sCSF leaks in order to reduce meningitis risk, no large series of patients who have been managed non-operatively exist from which it would be possible to assess the risk of meningitis in unrepaired leaks. At our own institution, very few if any patients with sCSF leaks are managed via a non-operative approach. We therefore sought to assess the incidence of meningitis in patients who are awaiting operative repair, and whether differences exist between patients who do and do not receive prophylactic antibiotics and/or pneumococcal vaccines.
Two studies in the published literature presented groups of patients who were managed conservatively without surgical repair due to either having refused, or being deemed non-surgical candidates on the basis of age or comorbidities. Rao et al presented 2 patients (3 ears) who were observed for a mean of 15 months (range, 15-16 months), and Hendriks et al presented 49 patients who were observed for a mean of 12 months (range, 1-94 months). In both studies, no patients developed meningitis. 35 It is unclear whether any, or all, of these patients received prophylactic antibiotics for any duration.
Review of our institutional data demonstrated a nil incidence of meningitis during the brief time period between diagnosis and surgical repair (with a median duration of 2 months, range 0.5-118 months). This finding was despite the majority of patients (88.5%) not receiving any antibiotics during the wait-time to surgery. Given that no patient in either group (10 who received antibiotics, 77 who did not) developed meningitis, we could not ascertain whether antibiotics modify the risk of meningitis while awaiting surgery. No conclusions can be made on the impact of pneumococcal vaccination, given that we were unable to ascertain actual rates of vaccination in our population, only the proportion of patients to whom vaccination was documented to have been recommended. No other study in the published literature reported the duration of the wait time from diagnosis to surgery during which patients had an active leak, or whether any patient suffered meningitis during this period. One might assume that this is because no instances of meningitis occurred in this timeframe, as was our institutional experience, but this cannot be concluded with certainty. Similarly, none of these studies reported whether prophylactic antibiotics were prescribed to patients awaiting surgical repair. Only 1 study reported rates of routine vaccination, with 73.3% of patients receiving 7- and/or 23-valent pneumococcal vaccines. Therefore, antibiotic and pneumococcal vaccine prescribing in this population are both severely underreported in the literature, and the impact of both on meningitis risk while awaiting surgical repair of sCSF leaks remains unclear. However, based on our own data, the risk of meningitis from unrepaired lateral skull base sCSF leaks over short durations of observation (eg, median 2 months in our cohort) appears low even in the absence of prophylactic antibiotics.
In contrast to the paucity of meningitis cases during the wait time from diagnosis to surgery, some patients with unrepaired sCSF leaks may develop meningitis as their first presenting symptom of a leak. At our own institution, there was a 5.7% prevalence of meningitis either by history or at the time of diagnosis of sCSF leak. Review of the literature demonstrated this prevalence to be 14.4% when considering a weighted mean across all identified studies (n = 30 studies). The duration of CSF leak prior to diagnosis, based on patients’ reported duration of symptoms, was a median of 6 months in our series (mean 23 months; range, 0.5-240). Only 7 of the other studies we identified reported this metric, with a mean symptom duration of 41 months (range, 19.2-69.6). Of course, it is impossible to ascertain the true duration of an undiagnosed CSF leak prior to a patient developing meningitis. The lower prevalence of patients presenting with meningitis in our series may therefore be due to a shorter average duration of symptoms prior to diagnosis, or differential rates of patient recall bias. Regardless, these cases point to the non-negligible risk of meningitis over long durations in lateral skull base sCSF leak.
Given these findings, including the lack of literature on the topic, we are unable conclusively determine the absolute risk of meningitis from an unrepaired sCSF leak, or the degree of risk reduction that prophylactic antibiotics and pneumococcal vaccination offer while patients are awaiting surgical repair. Our own institutional data suggests a low risk of meningitis from an unrepaired leak over short durations of observation even in the absence of prophylactic antibiotics. No firm conclusion can be made on this basis, though, since the overall cohort size is small, there is a 0% occurrence of the outcome in either group, and the risk period is relatively brief. We have identified a substantial gap in available evidence regarding meningitis risk, and the value of antibiotic prophylaxis and pneumococcal vaccination in the sCSF leak population. Studies specifically addressing these questions – either randomized controlled trials, or well-designed cohort studies—are required to better inform clinical practice.
Limitations of the present study include our lack of a purely observational cohort in which to compare rates of meningitis; an overall short duration between diagnosis and surgery during which patients are at risk of meningitis from an unrepaired sCSF leak; non-uniform antibiotic prescribing practices; potential for bias in patients’ abilities to recount or properly ascribe their duration of symptoms of leak prior to diagnosis; and inability to ascertain true pneumococcal vaccine uptake rates. In addition, we were unable to identify a cohort of patients who were treated via an observational rather than surgical approach at our institution.
Conclusions
The risk of meningitis in sCSF leaks and the roles of prophylactic antibiotics and pneumococcal vaccination while awaiting surgical repair have not been well-studied. While up to 63.6% of patients may suffer meningitis from an undiagnosed sCSF leak, among patients awaiting surgery for short durations of time (median 2 months at our institution) there appears to be a low risk of meningitis even in the absence of prophylactic antibiotics. Despite this, there remains insufficient evidence—including a paucity of published literature—to form conclusions or make recommendations regarding the roles of prophylactic antibiotics and vaccination in this population.
Supplemental Material
sj-docx-1-aor-10.1177_00034894231177756 – Supplemental material for Meningitis Risk and Role of Prophylactic Antibiotics in Spontaneous Lateral Skull Base CSF Leaks
Supplemental material, sj-docx-1-aor-10.1177_00034894231177756 for Meningitis Risk and Role of Prophylactic Antibiotics in Spontaneous Lateral Skull Base CSF Leaks by Alexandra E. Quimby, Emma De Ravin, Steven J. Eliades, Jason A. Brant, Douglas Bigelow and Michael J. Ruckenstein in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-docx-2-aor-10.1177_00034894231177756 – Supplemental material for Meningitis Risk and Role of Prophylactic Antibiotics in Spontaneous Lateral Skull Base CSF Leaks
Supplemental material, sj-docx-2-aor-10.1177_00034894231177756 for Meningitis Risk and Role of Prophylactic Antibiotics in Spontaneous Lateral Skull Base CSF Leaks by Alexandra E. Quimby, Emma De Ravin, Steven J. Eliades, Jason A. Brant, Douglas Bigelow and Michael J. Ruckenstein in Annals of Otology, Rhinology & Laryngology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.