
Abstract
Objectives:
The benefits of breastfeeding are well established, yet complex infants are less frequently supported to feed direct or pumped breastmilk. This article aims to provide an algorithm to support complex infants in meeting breastfeeding goals.
Methods:
Two cases are presented to illustrate the breastfeeding support pathway. Each involves early identification of motivated caregivers, consultation of allied health, and assessment of swallowing safety with modification of position or route as appropriate.
Results:
Two infants presented herein successfully continued to receive breastmilk despite airway complexity—1 with oral aversion secondary to prolonged nil per os period in the setting of tracheoesophageal fistula, and 1 with a tracheostomy secondary to subglottic stenosis.
Conclusions:
It is both possible and imperative to support complex infants in continuing to breastfeed, either directly or via the safest possible route, for the benefits to both members of the dyad.
Keywords
Introduction
Human milk is the optimal infant nutrition. 1 Infants with medical challenges benefit more substantially from breastmilk, yet these children are less often supported to breastfeed. 2 Medically complex and preterm infants are commonly encouraged to bottle feed, in order to measure volumes and quantify calories. This may lead parents to exclusively pump (EP) and feed expressed breastmilk (EBM) rather than directly feed at the breast. Though some remain committed to this path long-term, EPing requires significant maternal time commitment, and may lead to early breastfeeding cessation. 3
Pediatric otolaryngologists are uniquely positioned to support breastfeeding dyads with airway complexity. As airway and swallowing experts, we have a responsibility to encourage the feeding team to promote oral feeding when safe. Oral feeding at the breast does not require more calories or coordination than bottle feeding, is more physiologic and increases potential for bonding between the members of the dyad.3,4 Even partial direct breastfeeding as a complement to bottle feeding may provide comfort to both parent and child. Non-nutritive benefits include bonding and comfort, pain control and reduction of post-partum depression.5,6 Interestingly, breastfeeding difficulties and a lack of support can worsen mental health outcomes postpartum, making support of patients at risk for breastfeeding difficulty of critical importance. 5 This article provides an approach to protecting and promoting breastfeeding in the complex pediatric otolaryngology patient illustrated with a discussion of 2 cases.
A note that the use of inclusive language to describe lactation is critically important. It may be necessary to clarify the preferred term with lactating parent, be it “chestfeeding” or “nursing.” 7 In this manuscript, “breastfeeding” and “breastmilk” will be used throughout.
Methods
Patient Selection
Institutional ethics board approval was not required for this work. Caregiver feeding goals should be elucidated on initial history. Those parents wishing to feed breastmilk (even if oral feeding may not be initially or foreseeably possible) should be identified early to implement appropriate support.
Multidisciplinary Feeding Plan
With any medically complex infant, feeding involves a multidisciplinary team. Lactation consultants (LCs) should be involved at birth if direct breastfeeding or provision of EBM is a goal. If the infant requires a period of nil per os (NPO), the lactating parent should be provided with a double electric breast pump (available through neonatal intensive care (NICU) or maternity units) and supported to obtain a hands-free pumping bra. Frequent breast emptying should be encouraged to maintain supply during NPO periods, surgeries, or separations.
When oral feeding is planned, speech language pathologists (SLPs) and/or occupational therapists (OTs) should assess the patient at bedside for safety for oral feeds. While other feeding modalities are still in place, such as nasogastric tubes (NGTs), direct breastfeeding can be attempted. SLPs can also assist with positioning the infant for feeds and support for sensory issues such as heightened gag reflex. Weighted feeds (pre- and post-feeding weights) can be used to assess transfer at the breast if volumes are uncertain, with a precise scale accurate to at least the nearest 5 g.8,9 Registered dieticians assists with monitoring calories and growth. Figure 1 details the decision pathway progressing to direct breastfeeds.
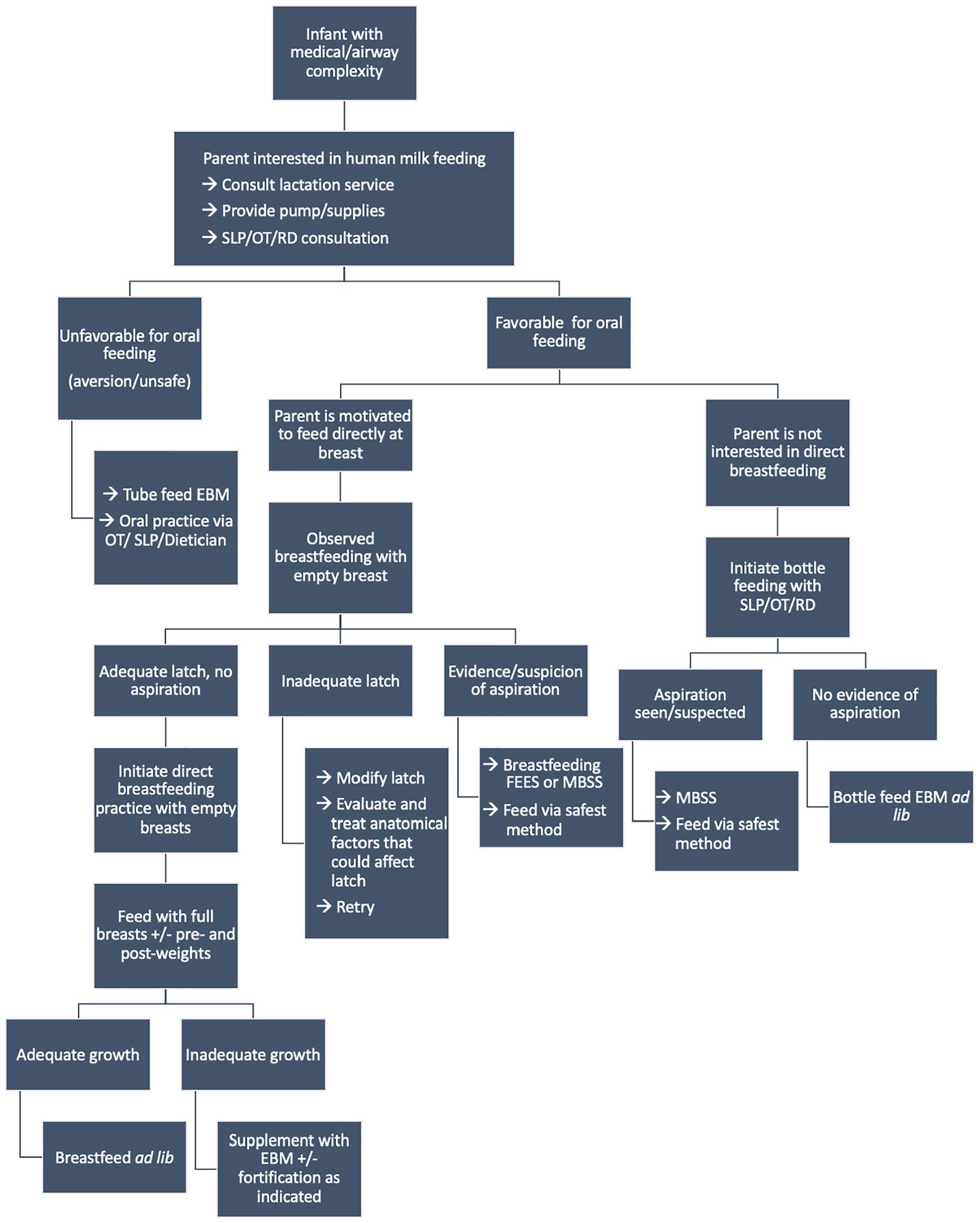
Decision pathway toward direct breastfeeding. This goal may not be achievable or desired for all breastfeeding dyads, for example those with craniofacial anomalies that preclude oral feeding, or those parents that prefer bottle feeding expressed breastmilk (EBM).
If bottle feeding is also planned, slow-flow bottle nipples and pacing the rate of the feed helps ensure this does not interfere with feeding directly at the breast. Assistance with pacing can be sought from SLP and lactation consultant team members. If bottle feeding is not required due to immediate adequate latch directly at breast, good milk supply, and demonstrated growth, it may be avoided completely.
Assessing and Optimizing Swallowing
Modified barium swallow studies (MBSS) cannot assess a breastfeeding swallow, and results from this study cannot accurately be extrapolated to what is occurring at the breast. The gold standard assessment for a breastfeeding infant is a functional endoscopic evaluation of swallowing (FEES) while breastfeeding, however there may be barriers to access for this test, and an experienced evaluator is required. Breastfeeding FEES detects real-time laryngeal penetration and aspiration, and is enhanced by applying blue or green non-toxic dye directly to the lactating parent’s nipple while feeding. Need and timing of swallowing evaluation, whether MBSS or FEES, are often dictated by the treating otolaryngologist. Bedside swallowing assessments may be preferable if a child is low risk for aspiration. MBSS or FEES may be preferable if a child is felt to be high risk for aspiration, or at significant risk of negative sequelae from aspiration.
Positioning is a key component in airway patency and should be guided by otolaryngologists. Infants who benefit from prone positioning for airway protection can be encouraged to use laid-back nursing position, with lactating parent reclined and infant latched in a prone position on the parent’s abdomen (Figure 2). Gravity provides favorable effects on the rate of milk flow, managing faster letdowns. Infants with lower tone, laryngomalacia, and retrognathia may benefit from this position. If tone is adequate, “Koala” feeding position performs a similar function, with baby upright straddling parent’s lap. Side-lying position also can improve airway patency (infant and parent lay facing each other on the same surface). If ankyloglossia is present causing pain with latch or poor transfer, this can also be managed by the otolaryngologist.

Laid-back breastfeeding position. The infant pictured is well, without airway anomalies, however this position helped to reduce choking due to relatively fast let-down. In infants with laryngomalacia or retrognathia, the prone position of the infant helps with airway patency.
Results—2 Cases
Patient 1—Baby M
Baby M is a term neonate born to a G2P2 mother. Aspiration episodes led to the diagnosis of H-type tracheoesophageal fistula (TEF) by NGT pullback esophagogram on day of life (DOL) 7 (Figure 3). The patient’s mother was experienced and motivated to breastfeed. LC was consulted, and electric pump provided. Frequent breast emptying was encouraged, with establishment of a good milk supply (defined as 24-30 oz/day). Baby M was encouraged to practice sucking with a soother with OT support.
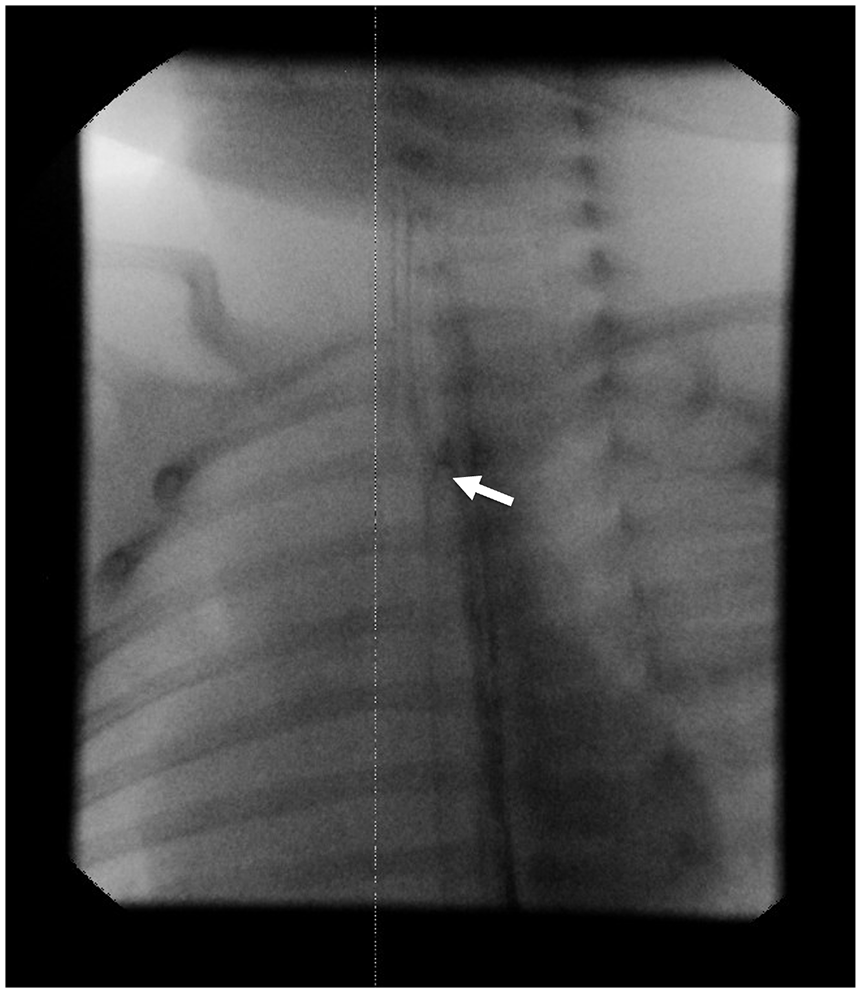
Nasogastric tube pull-back esophagogram, lateral view. An H-type TEF is demonstrated (white arrow), with contrast outlining the trachea (left, anterior).
Baby M was fed EBM with fortification due to poor growth via NGT until 3 weeks of age, at which time her weight and size was sufficient for transcervical ligation of her TEF by otolaryngology and pediatric general surgery. Patient’s mother continued to pump, and NGT feeds of EBM were started post-operative day (POD) 1. Oral feeding was attempted POD7 after contrast swallow confirmed TEF closure. However, Baby M had not orally fed for 4 weeks, leading to significant oral aversion despite soother use. When intake was sufficient to allow assessment, aspiration was not seen on repeat MBSS, however oral aversion persisted. Tube feeding was continued with EBM. Comfort nursing was encouraged, with Baby M’s parent allowing her to latch at the breast for non-nutritive sucking, which both members of the dyad enjoyed, but no milk transfer. Mom intended to continue provision of fortified EBM via tube feeding, with periodic attempts at comfort nursing on emptied breasts, and continued outpatient oral bottled EBM trials with OT. Given Baby M’s enjoyment of comfort nursing, when the NG tube was lost after hours, her mother elected to try direct nursing rather than NG tube reinsertion at 5 months of age. Milk transfer was observed without her typical observed discomfort with oral feeding. Close pediatrician follow-up revealed that her growth continues to follow between the 5th and 10th percentile, with an initial dip below the 10th during the transition period. A previously scheduled G-tube insertion was cancelled and she has continued to feed directly at breast since this time, a success mom attributes partially to the encouragement she received from her caring team.
Patient 2—Baby V
Baby V is a term male infant born to a G1P1 healthy mother after a pregnancy monitored for borderline polyhydramnios. Emergency Cesarean delivery was required for non-reassuring fetal trace, with transfer to NICU for continuous positive pressure (CPAP) support secondary to intermittent biphasic stridor and respiratory distress. Bedside scope at DOL1 failed to diagnose any abnormality. CPAP was weaned at 14 hours of life, with ongoing intermittent stridor. He was fed directly at the breast and with EBM and formula by bottle, transitioning to exclusive direct breastfeeding with adequate growth by DOL6. At DOL8 he was diagnosed with significant subglottic stenosis by repeat flexible nasopharyngoscopy to reassess the stridor, and underwent tracheostomy at under bag-mask ventilation at DOL15. Chest computed tomography and microlaryngoscopy confirmed grade 3 subglottic stenosis.
Baby V’s mother was encouraged to continue pumping. Beginning POD1, he was fed EBM via NGT. After first tracheostomy change, OT and dietician were involved for consideration of oral feeds. He began trials of feeding directly at breast on POD6 as per our protocol (Figure 1). There was no evidence of aspiration beyond the first trial feed (small volume breastmilk from tracheostomy) so he continued to advance in direct feeding. He was initially supplemented following feeds with EBM by NGT. Baby V progressed to full breastfeeds by POD8 without supplementation, with adequate growth. He was discharged when home supports were implemented, with a diagnosis of VACTERL syndrome. His growth remained adequate (Figure 4) and he continued to exclusively breastfeed until 6 months, when complementary foods were introduced with ongoing breastfeeding beyond 1 year (Figure 5). Laryngotracheal reconstruction is planned at 13-months of age.
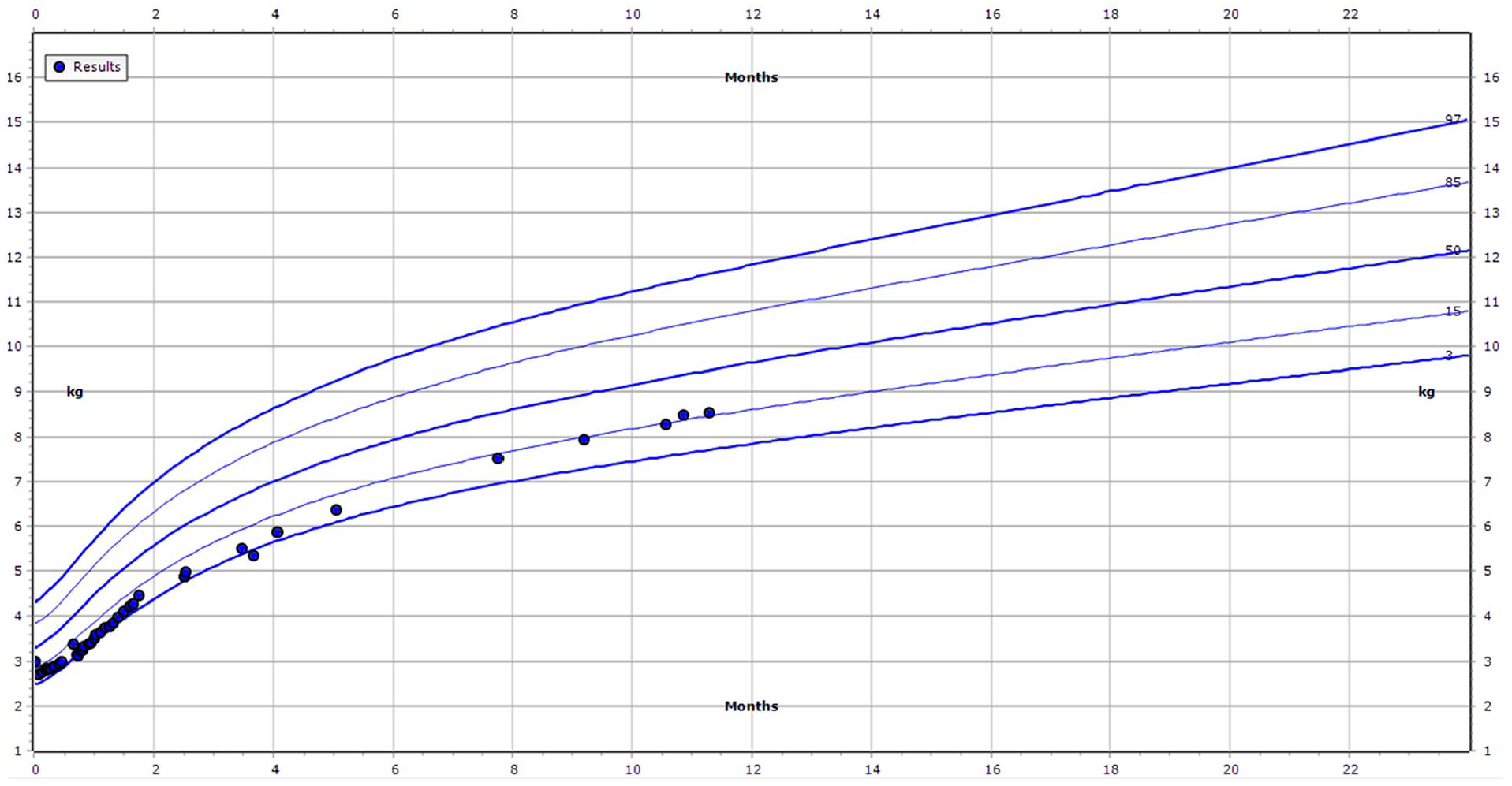
World Health Organization weight-for-age growth chart, boys 0 to 2. Baby V was born at the 23rd centile. During his early hospitalization and up to 3 weeks of life, he dropped to the third centile and continued to track on the third to fifth centile until his discharge at 2 months, at the fifth centile. At later visits, he measured between 12th and 18th centiles. Importantly, he maintained or exceeded his growth curve once established.

Baby V Direct Breastfeeding. Note FlexTend tracheostomy with heat/moisture exchanger allows close proximity to parent without occlusion of tracheostomy. Parental permission was obtained for the use of this photograph.
Discussion
Breastfeeding has innumerable benefits to lactating parent and infant. 1 However, there are many barriers to breastfeeding that are amplified in medically complex children, when other aspects of the infant’s health are prioritized over feeding modality. This may be the time when provision of breastmilk is most important. 2 Our group previously described supporting inclusive breastfeeding in an infant with a tracheostomy, with medical, and quality of life benefits to both members of the dyad. 10 This article demonstrates that exclusive breastfeeding without formula supplementation is also a possibility in complex airway patients. Other airway conditions that may be compatible with direct breastfeeding include vocal fold immobility and laryngomalacia. 11
Breastfeeding may not be straightforward in complex infants. Oral aversion is a concern in infants with prolonged periods of NPO, which was seen in the first case. There is a relative paucity of literature around prevention of oral aversion after periods of NPO, and aversion is frequently seen in the esophageal atresia population. 12 Language of support around breastfeeding and continued encouragement of oral tastes may increase the likelihood of success with oral feeding, as well as the quality of life of the parent. Other strategies described for management include positive non-nutritive oral stimulation, engaging in mealtime routines, and keeping caregiver-child interactions around feeding positive. 13 EPing and bottle or tube-feeding EBM is a viable, though labor intensive, method of feeding, and parents should be supported and celebrated if this is their chosen path. Any breastmilk that can be provided to the infant offers immune and other benefits to support optimal growth, and breastmilk fortification may allow continued breastfeeding with sufficient calories to avoid complete transition to formula if this is what caregivers desire.
Otolaryngologists are feeding and swallowing experts. We function as core members of the multidisciplinary teams driving oral feeding success. Breastfeeding is the biologic gold standard and our specialty should be educated and vocal advocates for direct breastfeeding where possible, or provision of EBM via the safest desired route if oral feeding is not possible.
Footnotes
Acknowledgements
Thank you to the families of Baby M and Baby V, that allowed their stories to be shared for this article, as well as KB and OB who shared their nursing photo.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.