
Abstract
Objective:
This review provides a summary of the current understanding of the health and well-being of the head and neck cancer (HNC) caregiver. Our goal is to understand the healthcare needs required by the caregivers of our oncologic patients, which may ultimately influence quality of care and support that cancer patients require during treatment and recovery.
Methods:
Independent database searches were conducted to identify articles describing HNC caregiver health and healthcare utilization. Search terms included key synonyms for head and neck cancer, caregiver, psychological stress, anxiety, depression, mental health service, and delivery of healthcare in the title/abstract.
Results:
After following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Protocol, a total of 21 studies were included. Among the 21 studies in the review, a total of 1745 caregivers were included. The average age was 57 years, the majority were female (58%-100%), and spouses/partners of the patients (77%). The literature demonstrates significant anxiety, depression, post-traumatic stress disorder (PTSD), and physical health decline in addition to multifaceted unmet physical and mental health needs among HNC caregivers.
Conclusion:
There is no standard for examining HNC caregiver healthcare needs, while there is evidence of increased healthcare utilization. The literature is limited regarding medical burdens faced by caregivers. Future research is needed to assess the physical health and comorbidities of HNC caregivers and their engagement with the healthcare system to guide further implementation of support models to address the needs of this population.
Introduction
The incidence of Head and Neck Cancer (HNC) is estimated at 650 000 cases worldwide, accounting for 3% of cancer diagnoses in the United States. 1 HNC is linked with substantial morbidity including disfigurement, and contributes to significant physical problems including impaired speaking, chewing, and swallowing.2,3 This can negatively influence psychological outcomes for the patient, potentially impairing quality of life.
A cancer diagnosis may cause immense lifestyle changes necessitating extensive support from caregivers.4,5 Caregivers are often responsible for demanding tasks including help with finances, communication, transportation, and tasks of daily living.6,7 Patients with HNC can also have significant standing care needs including wound care, tracheotomy management, and care of a gastrostomy tube. Multiple adverse consequences have been identified for the caregiver role including psychological, social, and economic distress. Additionally, caregivers may forsake their own health to care for the patient during the treatment and recovery periods. 8
It is important to identify the physical and psychological conditions faced by HNC caregivers and to understand the extent to which caregivers utilize healthcare resources for management of their own needs. Our goal is to summarize the current understanding of HNC caregiver physical and mental health in order to develop strategies in the future to better support caregivers, and, ultimately, improve clinical outcomes of our HNC patients.
Methods
Eligibility Criteria
This review was designed and performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Protocol. 9 We identified articles published between January 2000 and December 2020. Primary outcomes included assessments of physical health, psychological diagnoses, and use of healthcare resources, among HNC caregivers. Secondary outcomes included unmet needs, coping strategies, and illness perceptions as they relate to caregiver physical and mental health. Studies assessing these caregiver variables during any timeframe of the HNC diagnostic, treatment, and recovery periods were included in the review. Case reports and commentaries were excluded from the screening process. Additional exclusion criteria were non-English language studies and studies that were published outside the specified timeframe. Studies were excluded if they did not specifically address the state of caregiver physical health or psychological diagnoses including anxiety, depression, and PTSD.
Search Strategy and Study Selection
Independent searches of MED-LINE, Web of Science, Cochrane Library, and PsycINFO were conducted to identify articles published from 2000 to 2020. Reviews of reference lists, conference abstracts, and internet searches were conducted to ensure inclusion of unpublished or ongoing trials. The components of the search strategy included head and neck cancer, caregiver, physical health, mental health, and healthcare access. These components were used to identify corresponding MeSH terms and combined to develop search strings for PubMed. The terms included related terms for “head and neck cancer,” “caregiver,” “psychological stress,” “anxiety,” “depression,” “mental health service,” and “delivery of healthcare.” Search terms were modified based on keyword availability through other databases to ensure a broad scope of studies was included in the initial search (Supplemental Material 1). Search results were uploaded to an EndNote database. Duplicates were removed, and all titles and abstracts were screened with full papers reviewed for eligibility.
Data Collection
Two independent authors participated in the review process. In screening titles and abstracts, any disagreement/incongruence between the 2 reviewers was resolved by a third reviewer. For full papers included in the final review, data regarding caregiver demographics, HNC location and staging, treatment modality, and study period were collected. Additionally, the level of evidence was assigned to each study based on the Oxford Levels of Evidence (http://www.cebm.net/index.aspx?o=5653).
Results
Database searches and manual cross-reference searches identified a total of 595 articles. After applying the PRISMA protocol criteria, a total of 21 studies were included in the literature review (Figure 1). There was heterogeneity in reporting of caregiver health and healthcare utilization, thus a qualitative synthesis of the studies was used to integrate study results by analyzing common themes present in the available literature. It was not possible to perform a meta-analysis on study results.
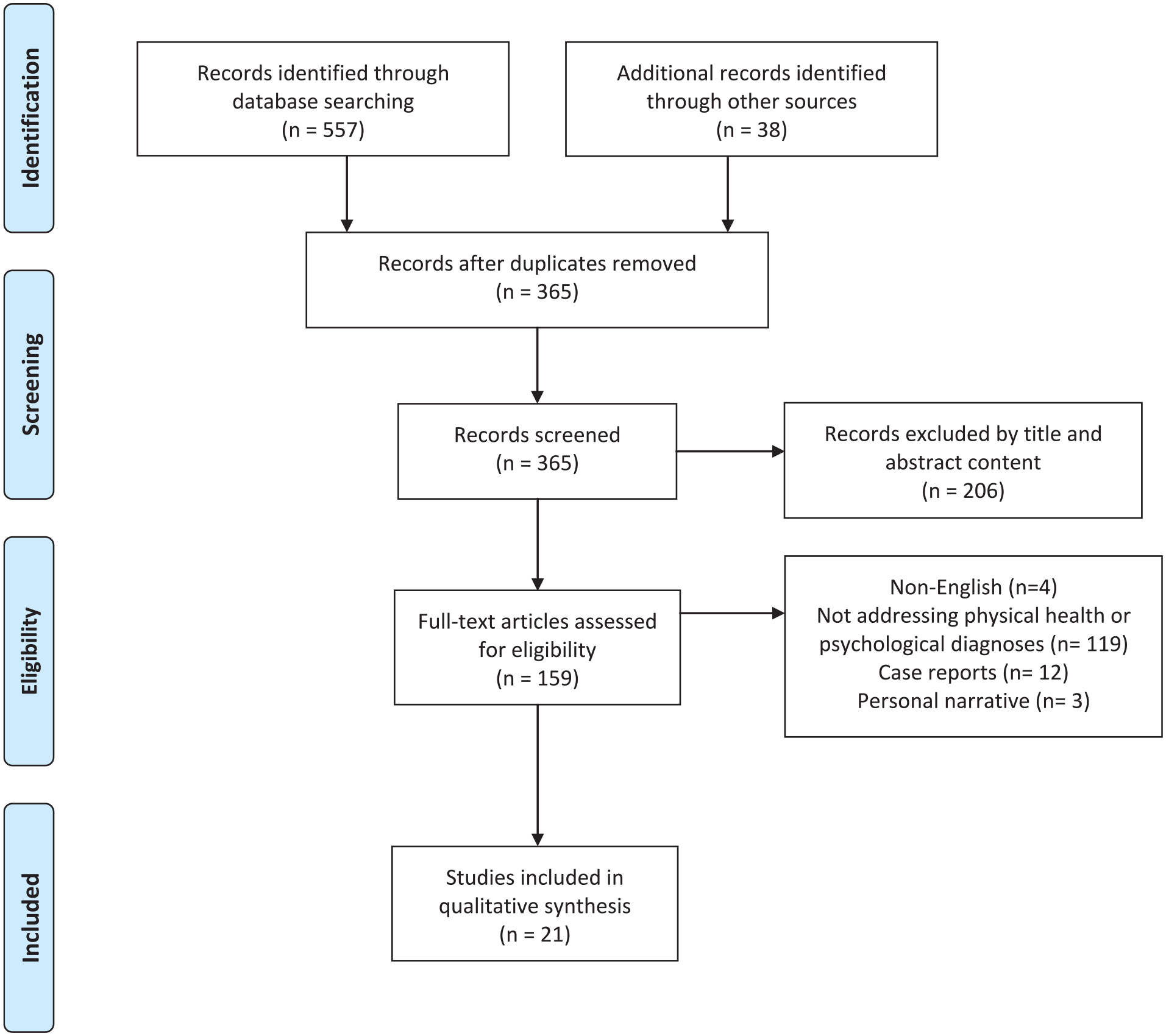
PRISMA Flow Diagram for systematic review article selection.
Demographics
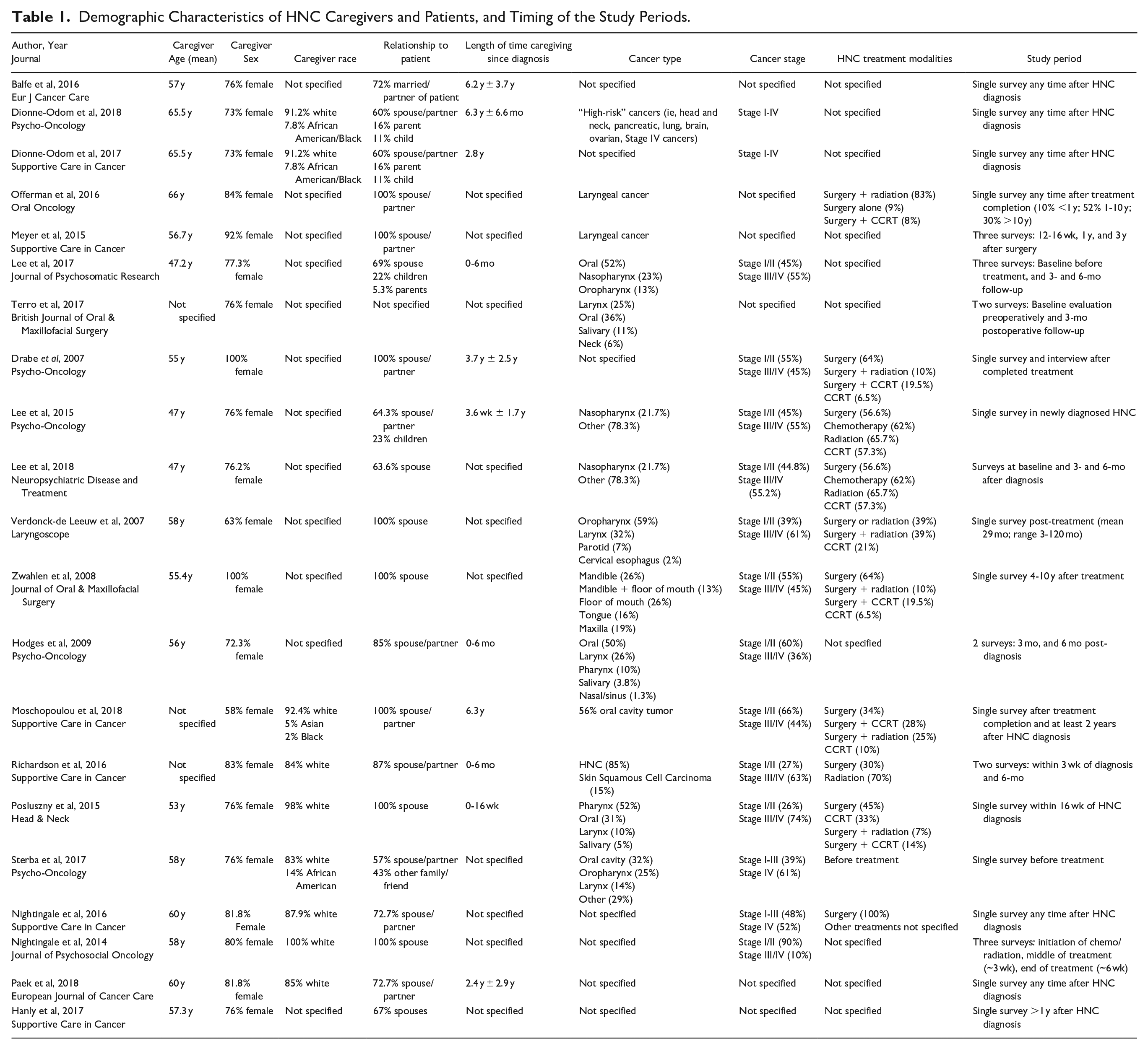
Among 21 studies, a total of 1745 caregivers were included. The average age was 57 years, the majority were female (58%-100%), and spouses/partners of the patients (77%). Studies were conducted anywhere from the time of diagnosis to years after treatment, and 9 studies did not specify length of caregiving since diagnosis (Table 1). There was a relatively even distribution of HNC patients with early stage (stage I/II, 49%) and late stage (stage III/IV, 51%) disease. There was significant variability in types of HNC (Table 1). A summary of the main findings from each study as they relate to the study objectives are included in Table 2.
Demographic Characteristics of HNC Caregivers and Patients, and Timing of the Study Periods.
Qualitative Article Summaries with Main Head and Neck Cancer Caregiver Health and Healthcare Access Findings with Levels of Evidence Based on Oxford Centre for Evidence-Based Medicine 2011.
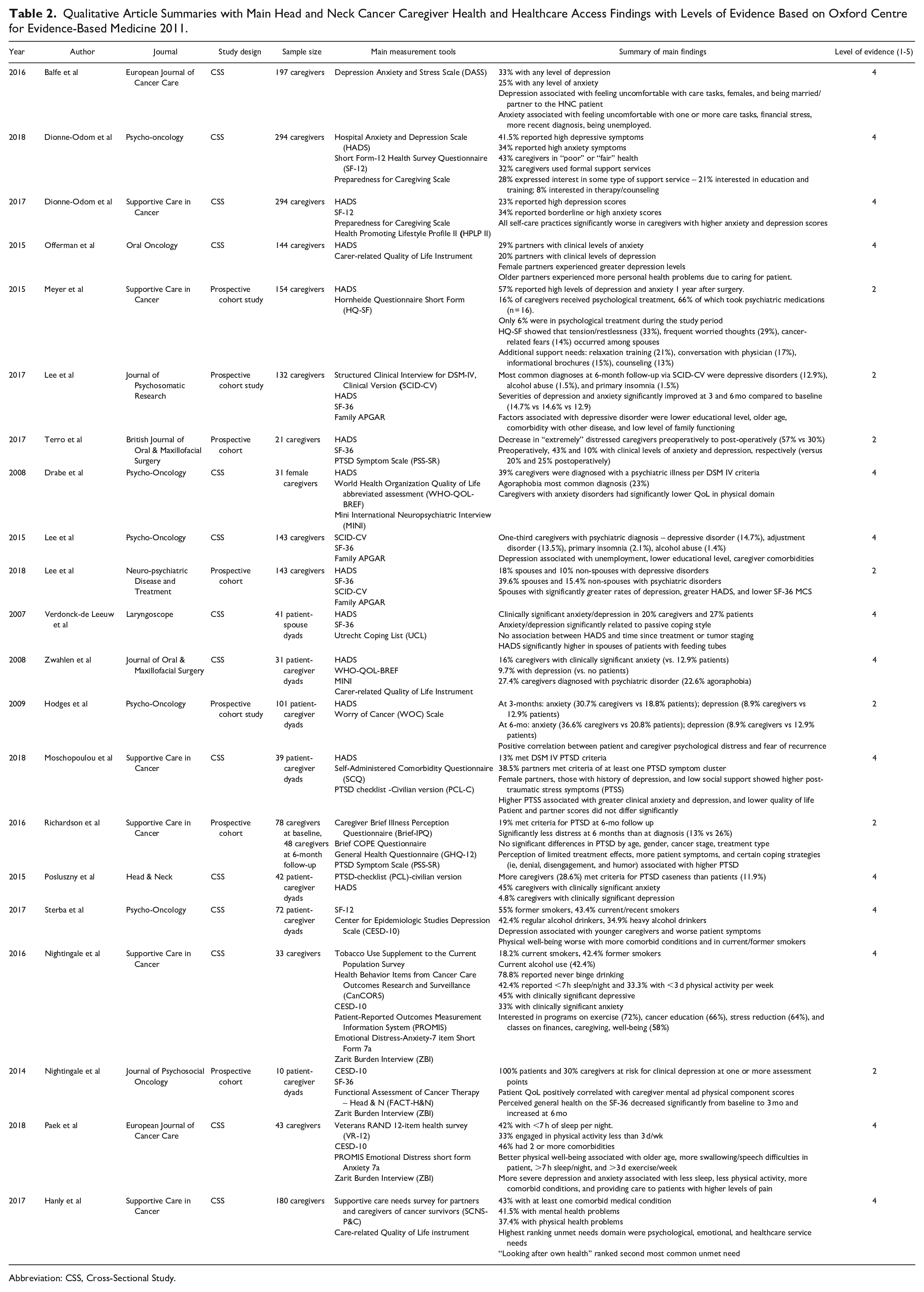
Abbreviation: CSS, Cross-Sectional Study.
Mental Health Findings
Multiple studies addressed the impact of HNC caregiving on mental health, with emphasis on clinically significant anxiety, depression, and post-traumatic stress disorder (PTSD). Several questionnaires have been developed to evaluate self-reported anxiety, depression, and stress levels (Supplemental Material 2). Table 2 displays the questionnaires used in each study. Thirteen studies utilizing the Hospital Anxiety and Depression Scale (HADS) demonstrated that anywhere from 9% to 57% of HNC caregivers suffer from clinically significant anxiety and/or depression.10-22 Using the Depression Anxiety and Stress Scale (DASS), Balfe et al reported anxiety and depression among 33% and 34% of caregivers, respectively. 23 In a cross-sectional study of healthy female spouse caregivers of HNC patients, 23% had anxiety disorders after completion of their spouses’ treatment, all of whom were also diagnosed with agoraphobia. 10 Zwahlen et al also reported an agoraphobia rate of 23% in caregivers anywhere from 4 to 10 years after treatment. 20
Lee et al compared caregiver HADS scores before treatment, and at 3- and 6-month follow-up, demonstrating significantly decreased anxiety and depression across this time trajectory (baseline 14.7%; 3 months 14.6%; 6 months 12.9%). 17 Terro et al also demonstrated a decline in depression (43%-25%) but increase in anxiety (10%-20%) preoperatively to the postoperative period. 18 Hodges et al found increased anxiety and similar depression rates with HADS at 3 months (anxiety 30.7%; depression 8.9%) compared to 6 months post-diagnosis (anxiety 26.6%; depression 8.9%). 21 Two studies highlighted other mental health disorders among caregivers and found similar rates of primary insomnia and alcohol use disorder at the time of HNC diagnosis and 3- and 6-month follow up (Table 2).17,24
As HADS score increased, overall caregiver health status declined, 11 which was a consensus among studies.10,17,25 Self-care practices (ie, stress management, physical activity) were significantly worse for caregivers with higher anxiety and depression. 13 Increasing levels of depression were associated with discomfort toward HNC care tasks, especially providing care to patients with higher pain levels or feeding tubes.11,23,25 Additionally, female caregivers demonstrated higher rates of depressive disorders compared to males.10,12,22,23 Spouses, lower educational level, and low level of social support were associated with more severe depression and anxiety.17,19,22,23 While Sterba et al concluded that depression is associated with younger caregivers, 26 Lee et al highlights older age as a risk factor for depression and anxiety. 17
The prevalence of PTSD was also investigated among HNC caregivers, with 13% to 29% of caregivers meeting diagnostic criteria for PTSD.22,27,28 Thirty-nine percent of HNC caregivers met criteria for at least one PTSD symptom cluster. 22 More patient symptoms, female-gender, higher HADS scores, low social support, and denial, behavioral disengagement, or humor coping strategies, were associated with greater PTSD symptomology.22,27,28 Caregiver perceptions of limited treatment effects and more patient symptoms were also associated with higher PTSD. No significant differences in PTSD by age, cancer stage, and treatment type were observed. 28
Six studies surveyed patients and their caregivers as dyads. Self-reported depression and anxiety and quality of life between caregivers and patients were shown to be significantly associated.11,20,21,26,27,29 Posluszny et al reported that over half of caregivers met criteria for anxiety/depression, compared to one-quarter of patients within 16-weeks after diagnosis. 27 Nightingale et al examined depression throughout the radiation treatment period and found 100% of patients to be at risk for depression at one or more time points compared to just 30% of caregivers. 29
Physical Health Findings
Physical health findings refer to the physical health effects of caregiving on the HNC caregiver. Eight questionnaire tools to assess physical health were included in the review: Short Form (SF) 12, SF-36, Health Promoting Lifestyle Profile II (HPLP-II), General Health Questionnaire (GHQ-12), VR-12 physical component score (PCS), Health Behavior Items from Cancer Care Outcomes Research and Surveillance (CanCORS), Self-Administered Comorbidity Questionnaire (SCQ), and CarerQoL-7D (Supplemental Material 2).
Lee et al and Hanly et al both reported that 43% of their caregiver populations had at least one comorbid condition,17,30 while Paek et al found 46% had 2 or more comorbidities. 25 Forty-three percent of caregivers reported being in “poor” or “fair” health, 15 and 7% expressed decline in health while caring for the patient. 12 Nightingale et al reported a decline in caregiver-perceived general health during radiation therapy, and subsequent improvement after the conclusion of treatment. 29 Additionally, Nightingale et al reported that caregivers get less than 7 hours of sleep per night (42%) and less than 3 days of physical activity per week (33%) due to time allotted to caregiving, 14 with Paek et al reporting similar results. 25 Offerman et al concluded that older partners experienced more physical health problems, 12 while Paek et al found that better physical caregiver well-being was associated with older age, more sleep per night and exercise per week, and patients with more swallowing/speech difficulties. 25
Two studies assessed smoking behaviors of caregivers, with 18% to 42% identifying as current smokers and 42% to 55% as former smokers.14,26 Both studies reported a regular alcohol use rate of 42%. Sterba et al found that 35% of caregivers are heavy drinkers and Nightingale et al reported that 22% of caregivers engage in binge drinking behaviors.14,26
Access of Healthcare Resources
Caregiver access of healthcare resources refers to how HNC caregivers engage with the healthcare system for their own health and caregiving concerns. Two studies examined caregiver use of formal support services. Thirty-two percent (n = 294) reported use of support services such as therapy/counseling, and caregivers with higher depression and anxiety used services at slightly higher rates (8% and 9%, respectively). Other services included education and training (19.7%), and assistance from outside organizations (11.2%). 15 Assessment of psychological treatment of spouses of HNC patients demonstrated that 16% received psychological treatment, 66% of whom took psychiatric medications. However, there was no significant change in use of psychological services over the caregiving period, with 5% of spouses actively receiving psychological treatment/counseling at the 3-year mark after surgery. 16 The reasons for non-usage of psychological services included lack of information, insufficient motivation, and inconvenient location. 16
HNC caregiver interest in healthcare services was explored across multiple studies. Richardson et al reported 40% of caregivers wanted psychological support at the time of diagnosis; however, this declined to 33% at 6-month follow up. Timing of psychological support was important to caregivers, with interest in resources early after diagnosis and before treatment. 28 Caregivers expressed preferences for support via face-to-face meetings and home visits, as well as delivery through the mail, computer/internet, or clinic visits. 14 Caregivers expressed interest in many types of support or wellness services, with education and training being most common.14,15 Meyer et al reported that relaxation training, conversation with the patient’s physician, and conversation with a psychologist or social worker were the 3 most desired services. 16 Caregivers were also interested in classes for exercise, stress and financial management, cancer education, and smoking cessation. 14 Interest in healthcare services was associated with higher depressive and anxious symptoms, younger age of caregiver, minority status, being less prepared for caregiving, and experiencing more care demands.14,15
Unmet Needs
Despite caring for a cancer patient with complex needs, caregivers still have their own significant needs that may go unmet, leading to negative impacts on health status and capability of caregiving. Hanly et al used the Supportive Care Needs Survey for Partners and Caregivers of Cancer Survivors (SCNS-P&C; Supplemental Material 2) to assess needs in the informational, emotional, health services, work, and social domains. They found that “psychological and emotional needs” were the highest-ranking unmet need domain, followed by access to healthcare services. 30
Discussion
The health and well-being of HNC caregivers are profoundly affected by the often complex and prolonged treatment and recovery of their loved ones. Survival rates for HNC have increased in recent years,31,32 and with greater survivorship comes more caregivers impacted by HNC. Rates of clinically significant anxiety and depression among HNC caregivers are greater than rates among caregivers of other cancer types (20%-57% vs 13%), 33 and caregivers often experience increased psychological diagnoses compared to patients themselves.20,27 This review collectively examines the physical and psychological health of HNC caregivers and their use of healthcare services to better understand how the healthcare system can serve the needs of this population.
In the present review, the majority of caregivers were female, which limits our ability to compare male versus female caregiver health status. This gender prevalence disparity may influence the observed psychological findings as females consistently report higher rates of anxiety and depression in the general population.34,35 In addition, there was heterogeneity in the screening tools for anxiety and depression, which may account for differing rates of anxiety and depression across studies.
The existing literature indicates that advanced disease is associated with higher caregiver burden, including more negative mental health implications 36 ; however, this review had limited examination of the impact of cancer type and stage on caregiver psychological health, thus requiring further investigation. There was also significant variability in when caregivers were evaluated during a patient’s treatment course. The evidence suggests that the immediate post-diagnosis period and 6-month interval after treatment are times of significant psychological distress,17,21,28 as caregivers must endure the burdens of bad news, extensive cancer-related information, and demands of treatment. In a study of cancer survivor spouses’ engagement with mental healthcare, greater care demands were associated with less utilization of mental health resources, 37 which could present a major barrier in HNC due to the many challenging caregiving tasks. In addition, the evidence demonstrates significantly fewer health care encounters (ie, physician office visits, hospitalizations, and emergency room visits) among cancer caregivers in the 12-month post-diagnosis period compared to controls. 38 Acquired communication impairments in the HNC patient have been shown to contribute to social withdrawal and loneliness, 39 which may also contribute to caregiver isolation and restricted healthcare access. Therefore, understanding how the caregiving role in HNC impacts the capacity to access support services is warranted.
Barriers to accessing support services may contribute to discrepancies between psychological health problems among caregivers and use of supportive resources observed in the current review. Meyer et al reported that 57% of spouses experienced significant psychological distress 1 year after surgery, yet only 16% sought psychological treatment. 16 This is less than reported in a previous study of psychiatric disorders among caregivers of advanced cancer patients, where 29% utilized professional mental health services after diagnosis. 33 A study assessing the use of an app-based mental health intervention targeted toward breast cancer patients and caregivers demonstrated improvements in anxiety, depression, and overall distress. 40 Similarly accessible interventions in the HNC population may assist in reducing the incongruity between distress and mental health service utilization, but this requires further exploration. This review identified preferred resources among caregivers including relaxation training, stress management, and smoking cessation,14,16 which could represent avenues for targeted interventions. Support strategies could be aimed toward high-risk caregivers, as identified in this review, such as spouses, those with lower educational level or social support, as well as coping and illness perceptions associated with poor mental health.17,19,22,28
Our review demonstrates limited evidence addressing the impact of caregiving on physical health. A study of the relationship between comorbidities and quality of life among advanced cancer patient-caregiver dyads showed that hypertension (30%), heart disease (26%), and depression (22%) were the 3 most common comorbidities among caregivers. As comorbidities increase, caregiver and patient mental health and quality of life significantly decrease, ultimately contributing to patient mortality.10,17,25,41 Therefore, future studies could assess comorbidities and management of chronic conditions, so we can better understand how the healthcare system can assist in increasing their engagement to serve their unmet needs.30,42
This data emphasizes the need for implementation of HNC caregiver support strategies. Richardson et al evaluated a supportive care intervention for caregivers of patients with lung cancer, consisting of a needs assessment and individualized 12-week support plan. At the end of the study period, caregivers had fewer unmet needs particularly in emotional support. 43 Sterba et al developed a survivorship needs assessment planning (SNAP) tool for post-treatment HNC survivors and their primary caregivers to generate tailored care plans. At 6-week follow-up, depression and unmet needs in caregivers significantly decreased, and the majority of caregivers felt prepared for the post-treatment period. 44 These studies highlight the impacts of individualized caregiver assessments and interventions on psychological well-being; however, it remains crucial to continue research aimed to assess HNC caregiver comorbidities and access to healthcare resources. Development of a standardized, validated assessment tool to quantify caregiver physical health problems could help guide future interventions and resource allocation.
There are limitations associated with this review. First, although the literature search was comprehensive, published studies may have been missed. Publication bias may also have influenced the studies identified. The lack of validated measurement tools for HNC caregivers presents another limitation. Nonetheless, the reviewed studies do demonstrate use of multiple questionnaires to assess mental and physical well-being that have been validated in general populations. Lastly, due to the heterogenous nature of the studies, we were unable to conduct a metanalysis of the data.
Conclusions
The literature demonstrates that there is clinically significant anxiety, depression, post-traumatic stress disorder (PTSD), and physical health decline among HNC caregivers. The available literature is limited regarding specific medical burdens faced by caregivers or validated instruments for measuring their well-being. Future research is needed to assess the physical and mental health of HNC caregivers to develop effective and accessible caregiver support models to address the healthcare needs of this unique population.
Supplemental Material
sj-docx-1-aor-10.1177_00034894221088180 – Supplemental material for Health and Well-Being Needs Among Head and Neck Cancer Caregivers – A Systematic Review
Supplemental material, sj-docx-1-aor-10.1177_00034894221088180 for Health and Well-Being Needs Among Head and Neck Cancer Caregivers – A Systematic Review by Sarah Benyo, Chandat Phan and Neerav Goyal in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-docx-2-aor-10.1177_00034894221088180 – Supplemental material for Health and Well-Being Needs Among Head and Neck Cancer Caregivers – A Systematic Review
Supplemental material, sj-docx-2-aor-10.1177_00034894221088180 for Health and Well-Being Needs Among Head and Neck Cancer Caregivers – A Systematic Review by Sarah Benyo, Chandat Phan and Neerav Goyal in Annals of Otology, Rhinology & Laryngology
Footnotes
Author Contributions
All authors contributed to concept design, data acquisition and analysis, drafting of manuscript, and critical manuscript revision
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.