
Abstract
Objectives:
Dyskeratosis congenita (DC) is a progressive congenital disorder that predisposes patients to squamous cell cancers (SCC) of the head and neck. We report a case of a patient who underwent primary osteocutaneous free flap for mandibular SCC followed by additional treatments for positive margins and discuss a systematic review on therapeutic management for this patient population.
Methods:
Case report of a 39-year-old male with DC who underwent resection and reconstruction with a fibular free flap for mandible SCC, followed by revision surgery and adjuvant radiotherapy for positive margins. A systematic review was completed afterward with the following terms: “dyskeratosis congenita” AND “oral cancer” OR “head and neck” OR “otolaryngology” on Medline and Web of Science for articles between 1980 and 2021. In total, 12 articles were included that reported on DC and SCC in the head and neck.
Results:
Of the case reports that were included in this review, half the patients had recurrence within 1 year of primary treatments. Only 2 patients did not require revision surgery, adjuvant, or salvage therapy. Half of patients that received radiation therapy had severe side effects.
Conclusions:
This is the largest review of DC and SCC in the head and neck. Based off our case report and review, these patients have aggressive disease that often requires multi-modality treatment. Consideration should be taken in regards to reports of side effects with radiation therapy.
Introduction
Dyskeratosis congenita (DC) is an inherited bone marrow failure syndrome originally described in 1906. 1 Classically, this condition is characterized by nail dystrophy, abnormal skin pigmentation, and oral leukoplakia. 2 Inheritance is most often x-linked recessive and DC results from gene mutations that impair telomerase function. 3 Thus, patients have shorter telomeres than expected. DC is more commonly seen in males, but in total only 552 cases were recorded over the span of 30 years. 4 There is heterogeneity at both the genetic and clinical presentation levels, and other syndromes in this family of bone marrow failure syndromes includes Fanconi anemia and aplastic anemia. Patients with DC are at higher risk of developing hematological disorders and solid malignancies, the most common of the solid tumors being squamous cell carcinomas (SCCs) of the head and neck, followed by skin and anorectal cancers. 4 The rate of malignancy amongst these patients has been estimated at around 10%. 4
We present a unique case of a patient with DC who underwent mandibulectomy and free tissue transfer for SCC. This patient unfortunately had positive margins and required revision surgery and radiation therapy. A systematic review focusing on therapeutic management and outcomes was completed for patients with SCC of the head and neck region to highlight treatment options.
Methods
Our institution’s Clinical Ethics Review Board provided a routine exemption for this case report.
Case Presentation
A 39-year-old male, diagnosed with dyskeratosis congenita a decade prior, originally presented to his dentist with right facial swelling. Computed tomography showed extensive bony destruction of the right mandible (Figure 1). The patient underwent bony debridement, removal of teeth 44 to 48 (FDI notation), and sampling of the gingiva and tongue by Oromaxillofacial Surgery.
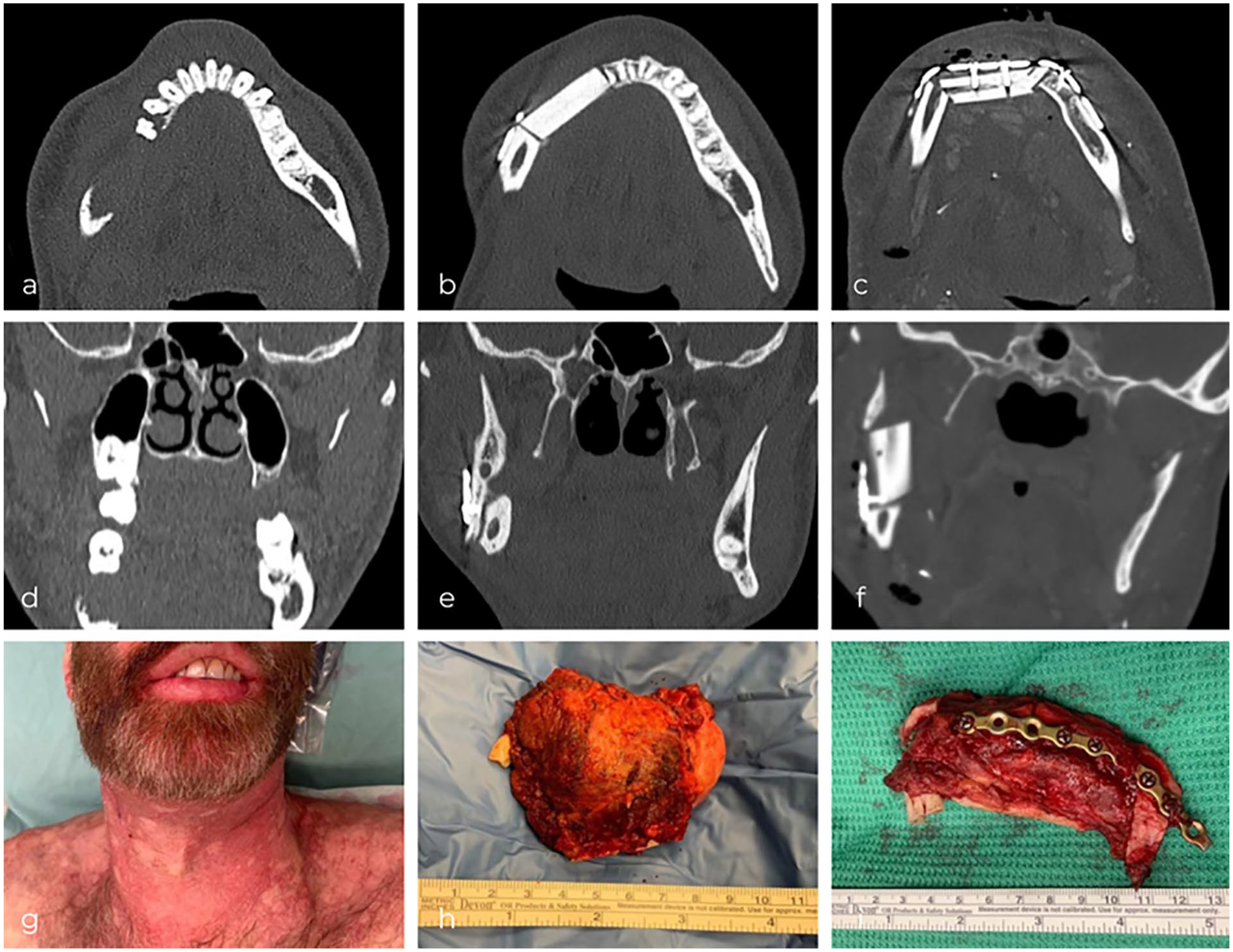
Axial and coronal CTs of the patient’s mandible at: (a and d) diagnosis, (b and e) initial post-operative, and (c and f) revision post-operative. (g) Mandibular asymmetry before initial resection with characteristic skin pigmentation. (h) Primary mandibulectomy. (i) Revision mandibulectomy.
His biopsy results demonstrated moderately-differentiated invasive SCC of the mandible and moderate dysplasia of the right anterior tongue. The patient was referred to Otolaryngology. In consultation, the patient had the typical triad associated with DC. His history and physical examination were otherwise insignificant, with no significant alcohol use or smoking history. The patient was counseled regarding management options for a cT4aN0 oral cavity SCC. Radiation oncology reviewed his case, and all involved reached consensus that surgery would be pursued as first-line treatment. Concerns from our radiation oncologists included worsening acute skin toxicity, long term fibrosis, and esophageal strictures or fistulas.
The patient underwent a right mandibulectomy, selective right neck dissection, and reconstruction with a left osteocutaneous fibular free flap (Figure 1). Pre-planned surgical cutting guides were used, as is standard at our institution (Figure 2). Intraoperative frozen soft tissue margins were not taken as it was felt that the margins were adequate. The fibula was crafted into a 2-segment reconstruction. The patient did well on the ward and was discharged with no complications.
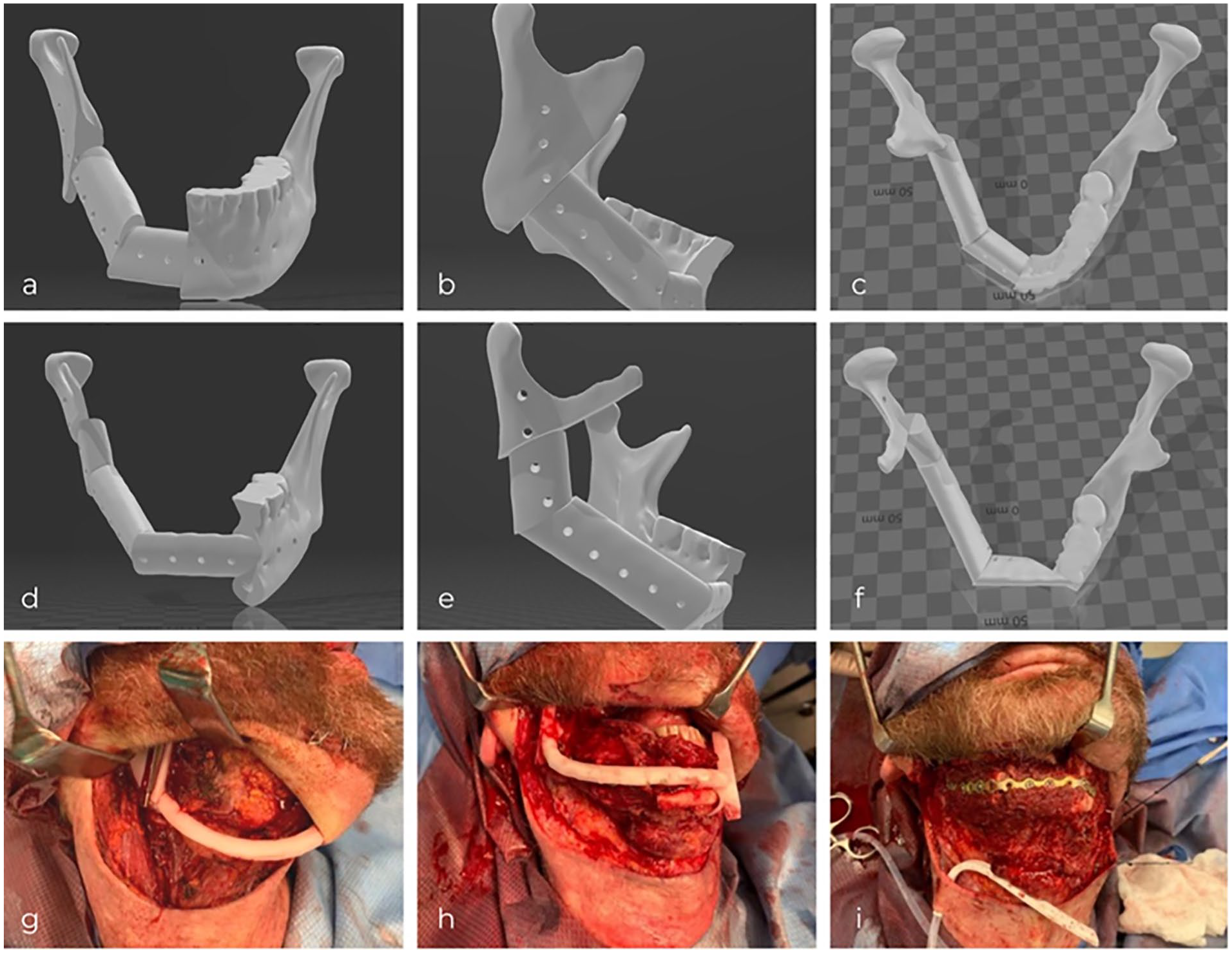
3D-images of patient’s planned fibular reconstruction prior to primary resection (a-c) and revision (d-f). 3D-printed cutting guides during primary resection (g) and revision (h). Revision fibular graft plated to remaining mandible (i).
The patient was subsequently seen in follow-up where he was informed that his anterior soft tissue and bony margin, as well as posterior bony margin, were extensively positive for SCC. This was after bone decalcification was done by pathology, as the bony margins had originally been reported as negative. The patient elected to proceed with a revision mandibulectomy and reconstruction. Margins were extended by an additional 3.5 cm anteriorly and 2.0 cm posteriorly. A 3-segment fibula reconstruction, with the contralateral right fibula as the donor, was performed.
The revision mandibulectomy osteotomy margins were negative for carcinoma and the scant amounts of soft tissue were also negative. However, after discussion with the patient, radiation therapy was added as an additional treatment for the positive soft tissue margins seen with his original mandibulectomy as only small amounts of additional soft tissue were resected with the revision. The patient has since completed his course and does not have recurrence at 6 months from surgery.
Systematic Review
The keywords “dyskeratosis congenita” AND “head and neck” OR “otolaryngology” OR “oral cancer” were used to search Medline and Web of Science for case reports between 1980 and 2021. Articles were included that discussed site of primary malignancy, treatment modality, and potential long-term side effects. Exclusion criteria included studies in languages other than English, retracted articles, articles lacking sufficient details, or those that only reported on skin cancers. Bibliographies of included papers were screened for additional studies.
In total, 40 articles were identified in the initial search and 10 others identified through bibliographic screening. Two independent reviewers (AQL, ECD) reviewed abstracts and any discrepancies were resolved by the senior author (JSD). After review, 12 articles satisfied the inclusion criteria. Please refer to Figure 3 for a flow diagram of articles included.
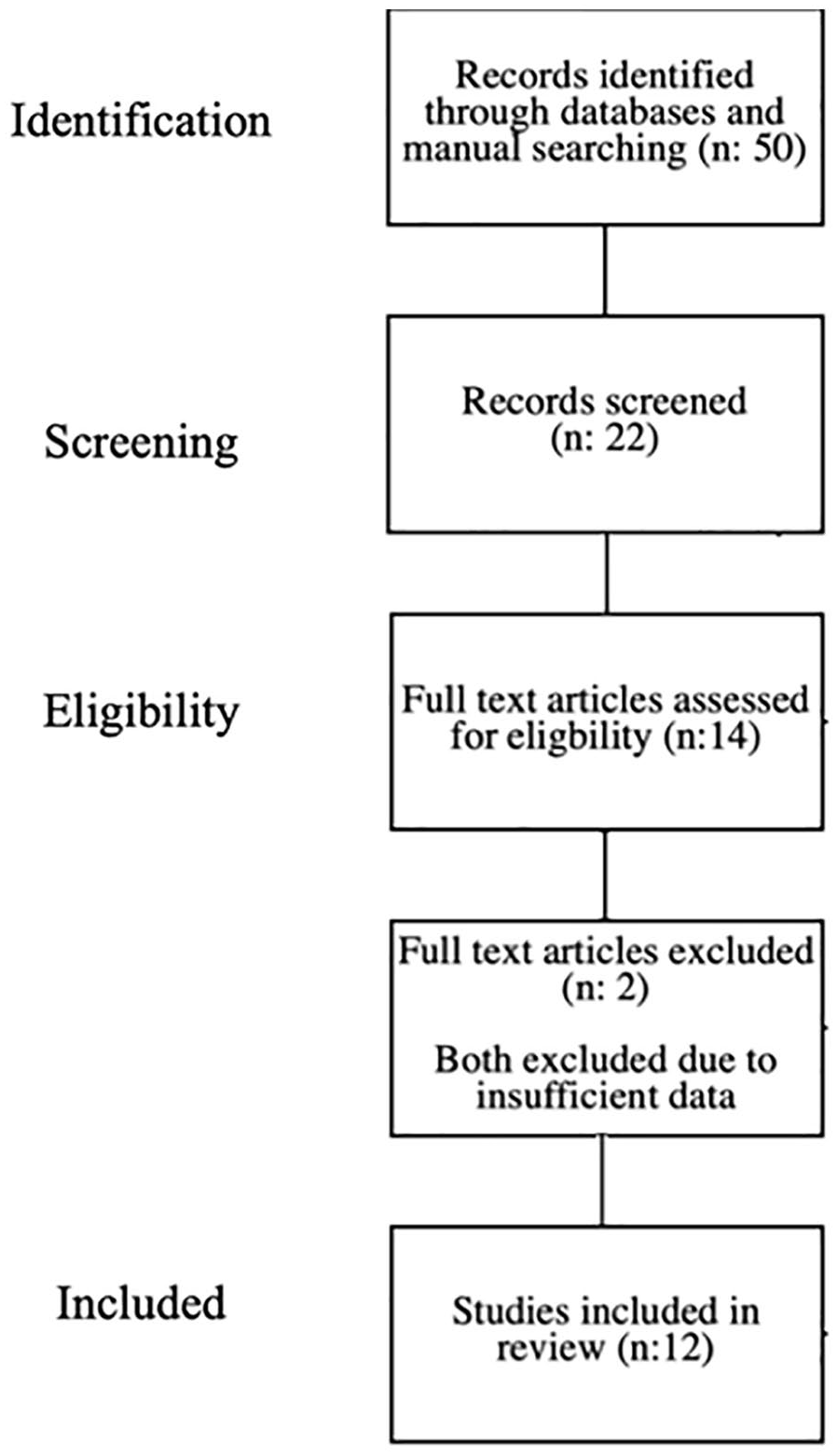
Systematic review study flow chart on case reports of solid squamous cell carcinomas in the head and neck for patients with dyskeratosis congenita.
Results
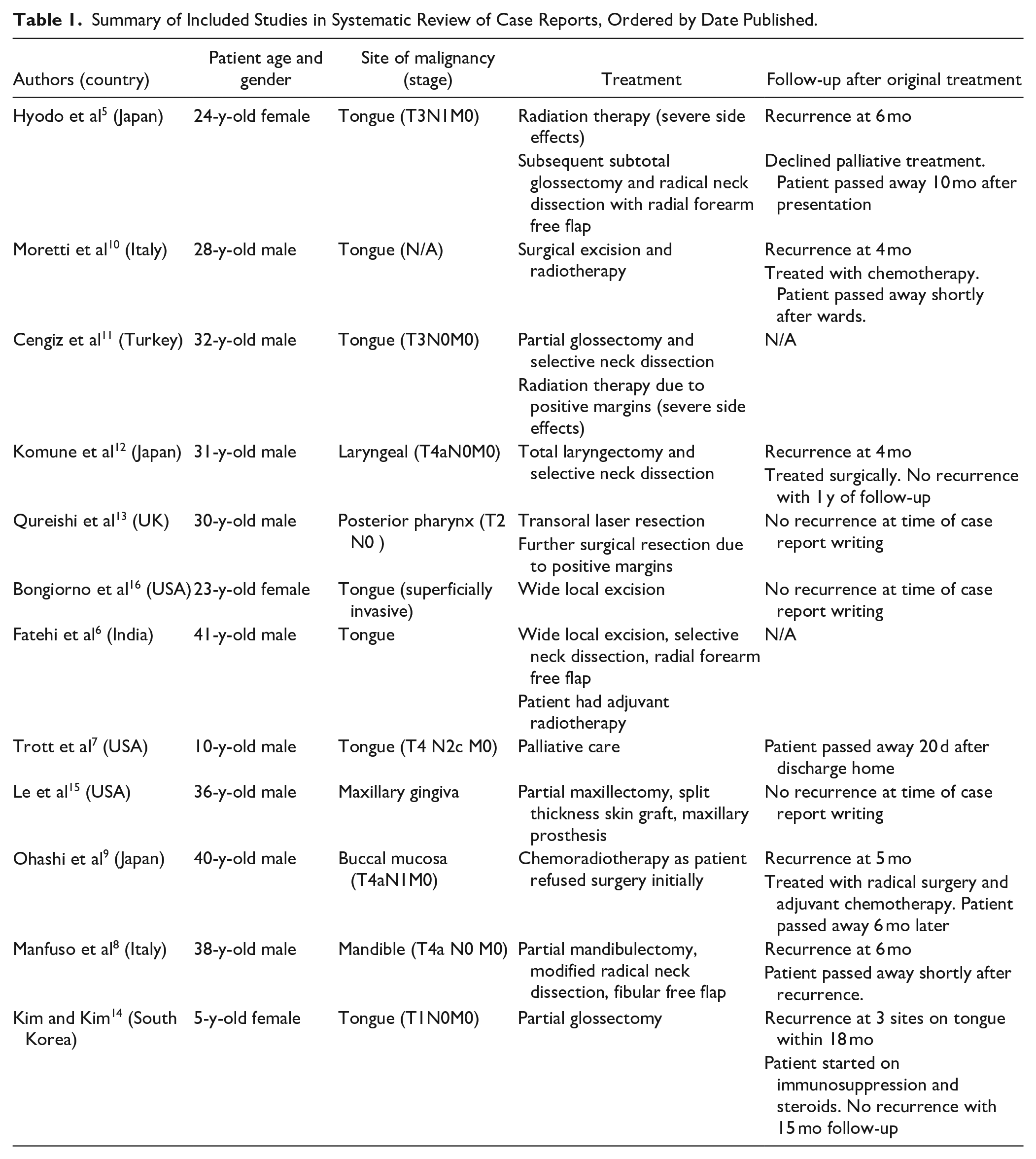
Included studies’ characteristics are summarized in Table 1. Of the 12 patients, 3 were female and 9 were male (ages 5-41). For initial treatment, 9 patients underwent surgical resection, 1 radiation therapy, 1 chemoradiotherapy, and 1 underwent palliative care. All but 2 patients required multi-modality therapy or revision surgery, and half of (6/12) the patients had recurrence within 1 year of treatment. Follow-up periods varied amongst the cases included, with the longest reported period being 15 months. Examination of those that passed away (5/12) after initial treatment showed a mean survival time of 5.4 months (1-10 months).
Summary of Included Studies in Systematic Review of Case Reports, Ordered by Date Published.
Discussion
This case illustrates an important clinical entity for those that provide care for head and neck cancers. We found a total of 12 other case reports of patients with DC and SCC of the head and neck, excluding cutaneous malignancies.5-16 To our knowledge, this is the largest systematic review of this patient population. Of note, most of the cases involved SCC of the tongue; this is the only case that reports on sequential osteocutaneous free tissue transfers.
Our patient did well after both surgical resections and free flap reconstructions with bone and soft tissue transfer, and had no complications. He did unfortunately have extensive positive margins after his first surgery with our team. This was thought to be due to the patient having aggressive disease that was uncharacteristic given his original presentation. We could not find osteocutaneous flaps used in other areas of the body for DC, and it is important to highlight that our patient had no complications with sequential fibular free flap transfers 1-month apart. At the time of follow-up, he was able to do activities of daily living and had minimal functional impact on his lower limbs.
At baseline, DC patients are at high risk for developing bone marrow failure, hence conventional DNA-damaging therapies may accelerate bone marrow failure or cause severe mucositis due to impaired mucosal lining repair. 13 Managing these patients should involve discussion with the patients about each treatment option and potential side effects. Patients with DC can have pancytopenia from bone marrow failure, which would also predispose them to complications when considering chemotherapy.5,11 Of the 4 reported patients who underwent radiation therapy, 2 did not tolerate the treatment modality (Refer to Table 1).5,11 One developed severe radiation mucositis after 26 Gy and had to discontinue radiation therapy for surgical resection. 5 The other case report details Grade IV mucositis developing after 20 Gy and continued severe mucositis after a treatment break. 11 We also do note that our institutions radiation oncologists were hesitant to begin therapy. The decision was made to proceed with radiation as an adjunct after the case was brought up at tumor boards and a long discussion about side effects was had with the patient. Other case reports have also highlighted that oncologists in multi-disciplinary discussions have recommended surgical treatment as first-line due to these concerns.13,15
If malignancy is present, we would also advocate for wide surgical margins for DC patients. It does appear that their cancers are more aggressive based off the other reported cases, as well as our own experience. Routine intraoperative frozen sections may be helpful as their disease seems to more aggressive than clinical presentation would suggest. Only 2 previously reported cases, at the time of writing this manuscript, had not required revision, adjuvant, or salvage treatment modalities.15,16 Furthermore, patients with DC can develop multiple primary malignancies.17,18 Trott et al highlighted the importance of prognosis for these patients, as their patient chose palliative care after diagnosis due to expected quality of life. The average life span for those with DC has been quoted at 23.6 to 42 years. 19
This case demonstrates a syndrome that otolaryngologists should be aware of due to patients’ high likelihood of developing malignancy; those with DC have 11-times the risk of being diagnosed with cancer compared to the general population. 4 Estimations of their mean malignant transformation rate of oral leukoplakia has been reported as around 30%. 20 Common oral features of DC include: loss of alveolar bone and buccal mucosa with leukoplakia, extensive dental caries, delayed dental eruption, and gingival inflammation and bleeding.21,22 Cannel has discussed that oral tumors in patients with DC often progress from white patches of necrotic epithelium or candida infections to recurrent ulceration and erythroplakia. He proposed that erosive leukoplakia and carcinoma developed at 20 to 30 years of age, which agrees with the ages of the case reports we found. 23
The authors agree that once patients are diagnosed with DC, they should have close follow-up of their upper aerodigestive tract for early detection of malignancies due to a high prevalence of leukoplakia. 24 While there are a small number of cases found in this review, true incidence is likely much higher. Recommendations for those with DC that have previously been discussed include monthly self-examinations of the oral cavity by patients and annual review with an otolaryngologist.4,25 At this time, there is no curative treatment for dyskeratosis congenita.
Conclusion
DC is a syndrome that places patients at higher risk for SCC of the head and neck. Our patient required aggressive revision surgery and adjuvant radiation. It is important for those that practice in the region to understand that recurrence is common and follow-up is needed for this patient population. We would advocate for first-line surgical treatment with wide margins, especially as radiation and chemotherapy may not be well tolerated in those with DC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Exemption
The University of British Columbia’s Clinical Ethics Review Board provided a routine exemption for this case report.