
Abstract
Objectives:
There are numerous well-described benefits to breastfeeding to both infant and mother. Even in healthy children with an uncomplicated perinatal course, there may be significant struggles maintaining a breastfeeding relationship. Infants with a complicated clinical course have been shown to benefit even more from the provision of breastmilk, however they are seldom encouraged to feed directly at the breast. There are no reports of successful direct breastfeeding in an infant with a tracheostomy.
Methods and Results:
We present the case of a breastfeeding dyad including a trach-dependent infant with congenital idiopathic bilateral vocal fold immobility who successfully initiated and maintained an inclusive breastfeeding relationship.
Conclusion:
This case illustrates that successful direct breastfeeding can be achieved in an infant with a tracheostomy. If a patient is felt to be capable of oral feeding via bottle, there is no reason that there should not be a trial of direct feeding at the breast, for the benefit of both members of the breastfeeding dyad.
Introduction
The benefits of breastfeeding are innumerable, and include provision of maternal antibodies, bonding between neonate and mother, and protection against illnesses including necrotizing enterocolitis.1,2 The World Health Organization recommends exclusive breastfeeding to the age of 6 months, with continued breastfeeding until 2 years of age. 2 Despite this, rates of exclusive or even inclusive breastfeeding in North America are very low, even in infants without medical comorbidities. 2
Complex and medically fragile babies may benefit even more from the protection conferred by breastmilk. 3 Often mothers of these fragile children are encouraged to provide breastmilk via expression, and do not always transition to successful feeding directly at the breast. This can be for a variety of reasons, including a perception that direct feeding precludes measurement of volumes, or perhaps that there is less ability to control flow rate to the child. However, exclusively pumping can be frustrating and increases risk of early cessation of breastfeeding. 4 Skin-to-skin contact, maternal-infant bonding, and milk supply are also improved with feeding directly at breast.
Patients with significant airway compromise have difficulty sustaining latch and would likely be unsafe and unsuccessful orally prior to tracheostomy. There are reports of supporting breastfeeding in surgical infants, and of supporting oral feeding in tracheostomy-dependent children.3,5 Patients with cleft lip and palate also frequently have feeding challenges, and literature suggests that those who are supported to direct breastfeed have better weight gain, similar wound outcomes, and improved parental relaxation and satisfaction compared to other methods of oral feeding. 6 However, there are no reports of direct breastfeeding in a tracheostomy-dependent neonate. Herein we present the case of a term neonate with idiopathic bilateral vocal fold paralysis who was successfully able to initiate and maintain breastfeeding after tracheostomy tube placement.
Case Report
Baby C is a female infant who was born at term following an uncomplicated pregnancy. At birth, she had increased work of breathing and required continuous positive airway pressure (CPAP). Baby was initially fed via expressed breastmilk via nasogastric tube. She was transferred to neonatal intensive care unit (NICU) for evaluation.
Stridor was noted early after birth resulting in otolaryngology consultation on day of life (DOL) 2. Flexible fiberoptic nasolaryngoscopy (FFL), revealed bilateral vocal fold paralysis (BVFP) with cords immobile in a median to paramedian position. Significant work of breathing was noted any time the patient was not on positive end-expiratory pressure (PEEP) of 10.
Evaluation, including a magnetic resonance image (MRI) of head, neck and chest, was normal. BVFP was confirmed to be persistent on 2 subsequent FFL examinations and nasal CPAP could not be weaned. In consultation with family, a decision was made to proceed with tracheostomy, performed in an uncomplicated fashion on DOL 17.
First tracheostomy change was performed on post-operative day-5 as is standard at our institution. A 3.0 Bivona flextend tracheostomy tube was placed. This is the typical choice for our neonatal patients to avoid pressure on the chin and chest from redundant tissue often present in this area, but is ideally suited to avoid occlusion by breast tissue. Until this point, nutrition of expressed breastmilk (EBM) from mother had been provided via nasogastric tube. Baby C’s mother was motivated to direct breastfeed rather than exclusively pump and bottle feed EBM.
A senior lactation consultant and feeding occupational therapist (OT) were consulted to observe breastfeeding for safety. Initial latch was trialed with breasts relatively empty, post-pump. Latch was safe, adequate, and no increased work of breathing or increased or milky tracheal secretions were noted. After 3 days of practice latching, breastfeeding was trialed with full breasts, and nasogastric feeding was weaned. Mom and baby both appeared to be comfortable, and mother expressed her happiness that she could provide milk directly at breast for her infant. (Figure 1). The Bivona flextend could be easily positioned to avoid occlusion while in close proximity to mother.

Direct breastfeeding in cradle position. Bivona Flextend with heat-moisture exchanger can easily be moved so it is not occluded, despite proximity to mother.
Weights initially declined slightly with exclusive breastfeeding, and a decision was made to feed with both EBM fortified to 24 kcal/oz in bottles and directly at breast, alternating roughly q3h. Weight fluctuations during initial hospital admission are charted in Figure 2a. At the time of hospital discharge at 6 weeks, her weight was 4395 g (from a birth weight of 4110 g). On FFL at 14 weeks of age, she had significant improvement in vocal cord mobility. Subsequently, Baby C underwent successful decannulation at 17 weeks of age. Post-cannulation, she did great with breast and bottle feeds, requiring fortification of her formula to maintain weight gain. At last follow-up visit, Baby C was thriving, with nice loud voice and gaining weight appropriately (Figure 2b).
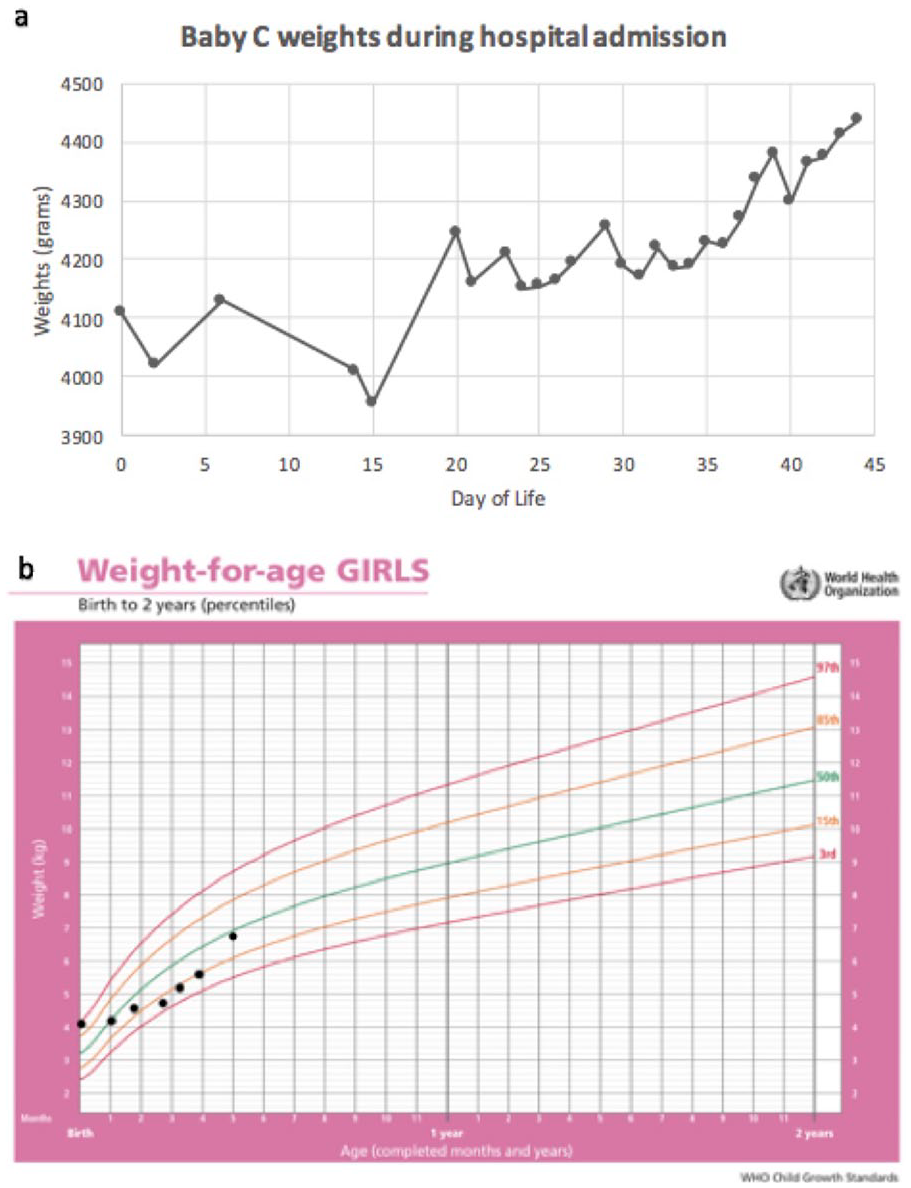
(a) Chart of infant weights. Note dip following switch to exclusive direct feeding at DOL 6, but still within normal limits of newborn weight fluctuation following birth. (b) WHO growth chart of Baby C’s weights.
Discussion
There are many indications for tracheostomy in infants. Some may have challenges that may preclude oral feeding completely, such as severe bronchopulmonary dysplasia, craniofacial anomalies, or certain cases of bilateral vocal cord immobility where cords are fixed in a more lateral position. Literature around oral feeding in patients with BVFI is limited. There is a small case series of 23 patients in which 61% required supplemental or exclusive tube feeding at presentation, with 70% orally feeding by follow-up. 7 Though the series is small, the authors note that those patients with idiopathic, non-neurologic BVFI were less likely to require a G-tube, with only 1 of 7 patients needing tube feeds in the study. Likewise, those without developmental delay also were more likely to avoid gastrostomy tube and successfully orally feed than those with developmental challenges.
Baby C had single level airway obstruction at the vocal folds with normal craniofacial anatomy and lung function. Vocal cords were in a paramedian position, her pathology was idiopathic, and she had no other neurological deficits. She was an ideal candidate for a trial of oral feeding and would typically be encouraged to bottle feed post-tracheostomy. However, in this or any patient that could theoretically tolerate a conventional bottle nipple, if the mother is motivated, breastfeeding should be encouraged, and the dyad empowered to try to feed at breast. Bottle trial can be reserved for cases when supplemental feeding is required or desired by mother, to avoid nipple confusion.
Feeding in a complex child is a multidisciplinary process. It is important to identify and anticipate feeding challenges early, so that lactating parents can be assisted with optimizing and maintaining milk supply during the initial workup and treatment of baby. This should include advocating for lactation consultant support immediately after birth, providing safe space and equipment to pump, and encouraging parents to continue pumping to maintain milk supply if direct breastfeeding or feeding expressed breastmilk is within parents’ feeding goals.
At our institution, feeding assessments are performed by trained OTs and speech-language pathologists (SLPs), and have been recognized in previous studies in tracheostomy-dependent infants as integral to safety and success. 5 Lactation consultants are required in this process to provide support to mother and guide latch correction. We propose an algorithm to follow utilizing the expertise of these critical allied-health professionals (Figure 3). Latch should be observed by an experienced lactation consultant, and ideally accurate pre- and post-feeding weights taken, as well as a close examination of tracheostomy secretions and signs of aspiration by the SLP or OT. We suggest using a Bivona Flextend if available as it can be positioned to avoid occlusion by breast tissue, but another option could include a Swedish nose heat moisture exchanger on a conventional non-flextend tracheostomy. Care should be taken to observe that the trach site is free of obstruction regardless of tracheostomy tube chosen.
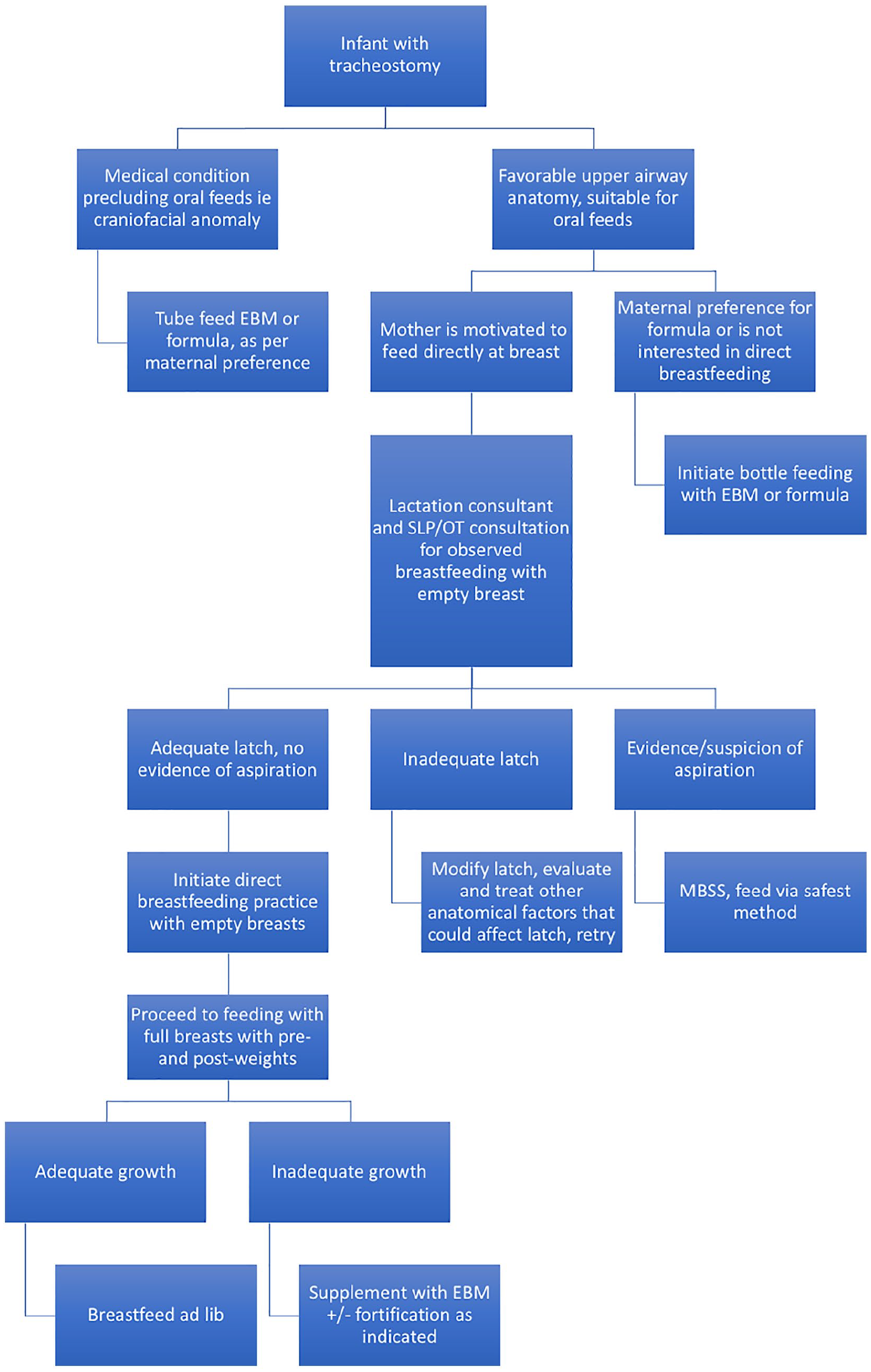
Direct breastfeeding algorithm. Note that this is specific to the infant after tracheostomy placement, but in these and other infants with a goal of direct breastfeeding or provision of expressed breastmilk, lactation support should be provided immediately after birth if a child cannot initially direct feed in order to establish milk supply.
As silent aspiration is a possibility in patients with vocal fold palsy, additional options could be considered for evaluation of swallowing safety depending on local resources and expertise. These would include fiber-optic evaluation of swallowing, dying the nipple during feeding and examining the tracheal secretions for discoloration, and modified barium swallow study, with the caveat that this does not accurately mimic breastfeeding as it usually uses bottled expressed milk or formula.
Conclusion
The guidance available about feeding in an infant with tracheostomy is inconsistent and not evidence based, as there is at present no literature describing direct breastfeeding in an infant with tracheostomy. 5 This case illustrates that successful direct breastfeeding can be achieved in an infant with a tracheostomy. As the airway specialist, it is the role of the pediatric otolaryngologist to advocate for a trial of direct feeding at breast if this fits with the goals of the patients’ mother. If a patient is felt to be capable of oral feeding via bottle, there is no reason that there should not be a trial of direct feeding at the breast, for the benefit of both members of the breastfeeding dyad.
Footnotes
Acknowledgements
We are grateful to Baby C and her mother for agreeing to be the subject of this case report. By doing so, they are assisting in potentially practice-changing feeding support for other complex newborns.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This case report was exempt from institutional ethics approval. Parents consented to the publication of this case and associated photographs.