
Abstract
The HAT2CH2 score [Hypertension (1 point), Age > 75 years (1 point), Stroke/Transient ischemic attack (2 points), Chronic obstructive pulmonary disease (1 point), and Heart failure (2 points)] was originally developed to predict the occurrence of new-onset atrial fibrillation. The aim of the present study was to examine whether this score could predict the development of no-reflow phenomenon (NR) in ST-segment elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (pPCI). Patients (n = 1552) with STEMI were consecutively enrolled in this single-center retrospective study. The SYNTAX score (SXscore) and HAT2CH2 score were calculated. The presence of thrombolysis in myocardial infarction (TIMI) score ≤2, without significant residual stenosis and mechanical obstruction, indicated the presence of NR. The HAT2CH2 score was significantly higher in the NR (+) group compared with the NR (−) group [2.29 ± 1.43 vs 1.46 ± 1.24, p < .001]. In multivariable logistic regression analysis, the HAT2CH2 score [OR = 1.585, p < .001] and SXscore [OR = 1.028, p = .017] were found to be independent predictors of NR. Receiver operating characteristic curve analysis showed that the HAT2CH2 score with a cutoff value of >2 determined NR, with 50.2% sensitivity and 79.4% specificity (AUC = .669, p < .001). In conclusion, the HAT2CH2 score may facilitate risk stratification in estimating NR in STEMI patients undergoing pPCI.
Keywords
Introduction
ST-segment elevation myocardial infarction (STEMI) is a life-threatening emergency with a high rate of morbidity and mortality, in which primary percutaneous coronary intervention (pPCI) has become the preferred treatment strategy. 1 The pathophysiology of acute myocardial infarction (MI) is a complex and dynamic process that is primarily triggered by platelet hyperactivation and thus can result in a sudden interruption in blood flow to myocardial tissue by narrowing the coronary lumen due to atherosclerotic plaque destabilization by various factors. 2 Rapid restoration of the infarct-related artery with pPCI is associated with improved ventricular performance and lower mortality outcomes in patients with STEMI. 3 No-reflow phenomenon (NR), which affects 10–30% of patients, is characterized as the persistence of inadequate myocardial perfusion despite the mechanical re-opening of an occluded infarct-related artery following PCI.4,5 The primary pathophysiological mechanisms causing NR include distal thrombus embolization, microvascular obstruction, and spasm. 6 Furthermore, NR is linked to the development of heart failure (HF), stroke, a significant proportion of damaged myocardium, malignant arrhythmias, and in-hospital mortality.7–9
The HAT2CH2 [Hypertension (1 point), Age > 75 years (1 point), Stroke/Transient ischemic attack (2 points), Chronic obstructive pulmonary disease (1 point), and Heart failure (2 points)] score is intended to identify individuals who are likely to develop forms of sustained atrial fibrillation (AF) based on age, presence of hypertension (HT), stroke/transient ischemic attack (TIA), chronic obstructive pulmonary disease (COPD), and heart failure (HF). 10 All aspects of the score are connected to pathophysiological mechanisms that increase the possibility of developing NR, such as atherosclerosis, vascular spasm, and microvascular dysfunction. However, while various risk variables have been demonstrated to influence the development of NR, no universally recognized simple and effective risk stratification approach for predicting exists. Therefore, the aim of the present study is to investigate the effect of the HAT2CH2 score on the development of NR for STEMI patients undergoing pPCI.
Methods
Study Population
This retrospective, single-center study consisted of 1552 patients with the diagnosis of STEMI who were admitted to the emergency department of Adana City Training and Research Hospital (Adana, Turkey), the regional pPCI center, within 12 h of the onset of symptoms between January 1, 2020, and January 1, 2021. With the exception of leads V2 and V3, where the cutoff values were .2 mV or higher in men 40 years of age or older, .25 mV or higher in men younger than 40 years, or .15 mV or higher in women, ST elevation consistent with MI was defined as new ST elevation at the J point in at least 2 contiguous leads with the cutoff value of .1 mV or higher in all leads, together with an elevation of cardiac troponin values with at least one value above the 99th percentile upper reference limit. Epidemiological, demographic, clinical, laboratory, procedural, and mortality data were obtained from patient medical records using a hospital registry system specific to each patient. Those were excluded from further analysis if they fulfilled the following criteria; aged 18 years or younger, severe liver disease, hereditary coagulation disorders, active cancer or on chemotherapy-radiotherapy treatment, fibrinolytic therapy, infarct-related artery diameter <2.5 mm, which is not suitable for stent placement, autoimmune connective tissue disease, or a high rate of missing values (Figure 1). Laboratory analysis of venous blood samples from all patients at the time of admission to the emergency department was performed using an automated chemistry analyzer (Roche Diagnostic Modular Systems, Tokyo, Japan). The estimated glomerular filtration rate (eGFR) was calculated according to the Modification of Diet in Renal Disease formula.
11
Flowchart of inclusion in the study.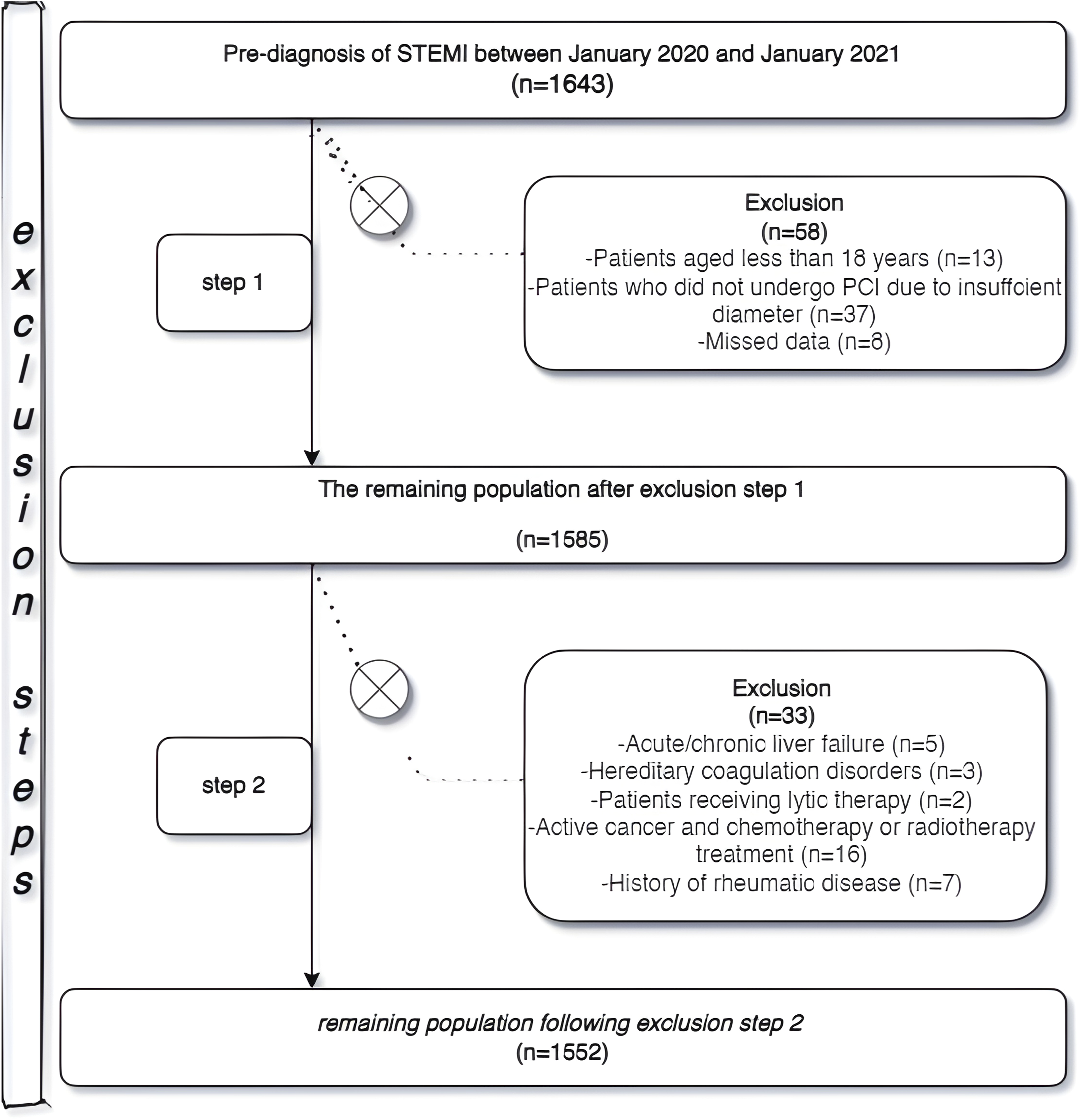
Previous Medical History Definition
Each patient’s medical history and co-morbidity data were retrospectively acquired from the national health registry systems and health files. HT was defined as office systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg or taking antihypertensive medication. In the presence of signs and symptoms, diabetes mellitus (DM) was diagnosed in those who met ≥1 of the following criteria: fasting blood glucose of ≥126 mg/dL, 2-h post-load plasma glucose of ≥200 mg/dl, HbA1c ≥ 6.5%, or random blood glucose of ≥200 mg/dL. Coronary artery disease was defined as the existence of a known MI, stent, or history of coronary artery bypass grafting. Stroke/TIA was defined as the presence of cerebrovascular events in which experienced neurologists had previously diagnosed based on clinical symptoms and brain imaging. COPD was described as the documented history of COPD in the medical registry or receiving COPD-specific pharmacological therapy (inhaled steroids, inhaled anticholinergics, inhaled β2-agonists, or theophylline).
HAT2CH2 Score and Parameters
The HAT2CH2 score was calculated by two independent cardiologists blinded to patient data as previously described. 10 Risk factors were coded as HT (1 point), age > 75 years (1 point), stroke/TIA (2 points), COPD (1 point), and HF (2 points). The HAT2CH2 score ranges from 0 to 7.
Coronary Angiography
All patients underwent coronary angiography (SIEMENS AXIOM Artis zee 2011; Siemens Healthcare, Erlangen, Germany) using a 6–7 French catheter via femoral route, guided by current recommendations. Acetylsalicylic acid (300 mg) and a P2Y12 inhibitor [prasugrel (60 mg loading), ticagrelor (180 mg loading), and clopidogrel (600 mg loading)] were given to the patients in accordance with current guidelines. 1 Unfractionated heparin (70–100 IU/kg bolus, 30–50 IU/kg maintenance in prolonged procedures) was administered after the decision for coronary intervention was decided. The use of various types of catheters, stent diameter or length, the decision of pre- and post-dilatation, and tirofiban infusion were all left to the operator’s discretion. Following coronary angiography, all patients were admitted to the coronary intensive care unit and began on routine antiplatelet medication (100 mg aspirin with 75 mg clopidogrel, or 10 mg prasugrel, or 90 mg ticagrelor twice a day). The presence of thrombolysis in myocardial infarction (TIMI) score ≤2, without significant residual stenosis and mechanical obstruction, indicated the presence of NR. 12 Angiography images were evaluated by two separate cardiologists who were unaware of the patient’s data. SYNTAX score (SXscore) was calculated as previously defined. 13 All coronary lesions with vessel diameter ≥ 1.5 mm and stenosis rate ≥ 50% were scored by two cardiologists blinded to patient data using the SXscore algorithm available at http://www.syntaxscore.com. The study population was separated into two groups based on NR status: NR (+) group (n = 239) and NR (−) (n = 1313).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 22.0 software (IBM Corp., Armonk, NY, USA). Continuous variables with normal distribution were expressed as mean ± standard deviation, while those with abnormal distribution were presented as median and interquartile range (IQR). An analytical method (Kolmogorov–Smirnov test) and visual methods (histograms and probability plots) were used to evaluate the normality distribution of continuous variables. Categorical variables were expressed as numbers (n) and percentages (%). The independent sample t-test or Mann–Whitney U test was used to assess continuous variables as appropriate. The chi-square test or Fisher’s exact test was used to compare categorical variables. Multivariable logistic regression analysis was performed to identify independent predictors of NR. The odds ratio (OR) and 95% confidence interval (CI) for each independent variable in univariable and multivariable regression analyses were calculated. Confounding factors were determined using the binary logistic regression model with elimination, including only parameters of the highest univariable significance. That is, variables with a p < .05 in univariable analysis were included in the multivariable analysis. Internal correlation analysis (multicollinearity) was carried out by determining whether the variance inflation factor <3, condition index <15, and variance proportions <.6 could be obtained using numerical expressions of individual parameters. In the regression analysis, the Hosmer–Lemeshow test was used to assess the goodness-of-fit. Receiver operating characteristic (ROC) curves and areas under the curve (AUC) analyses were performed to estimate the predictive accuracy and performance of the HAT2CH2 score in predicting NR. The Youden index was used to estimate the appropriate cutoff value for the HAT2CH2 score. Statistical significance was determined as 2-sided p < .05.
Results
Demographic, Admission Clinical, and Laboratory Parameters of the Overall Population.
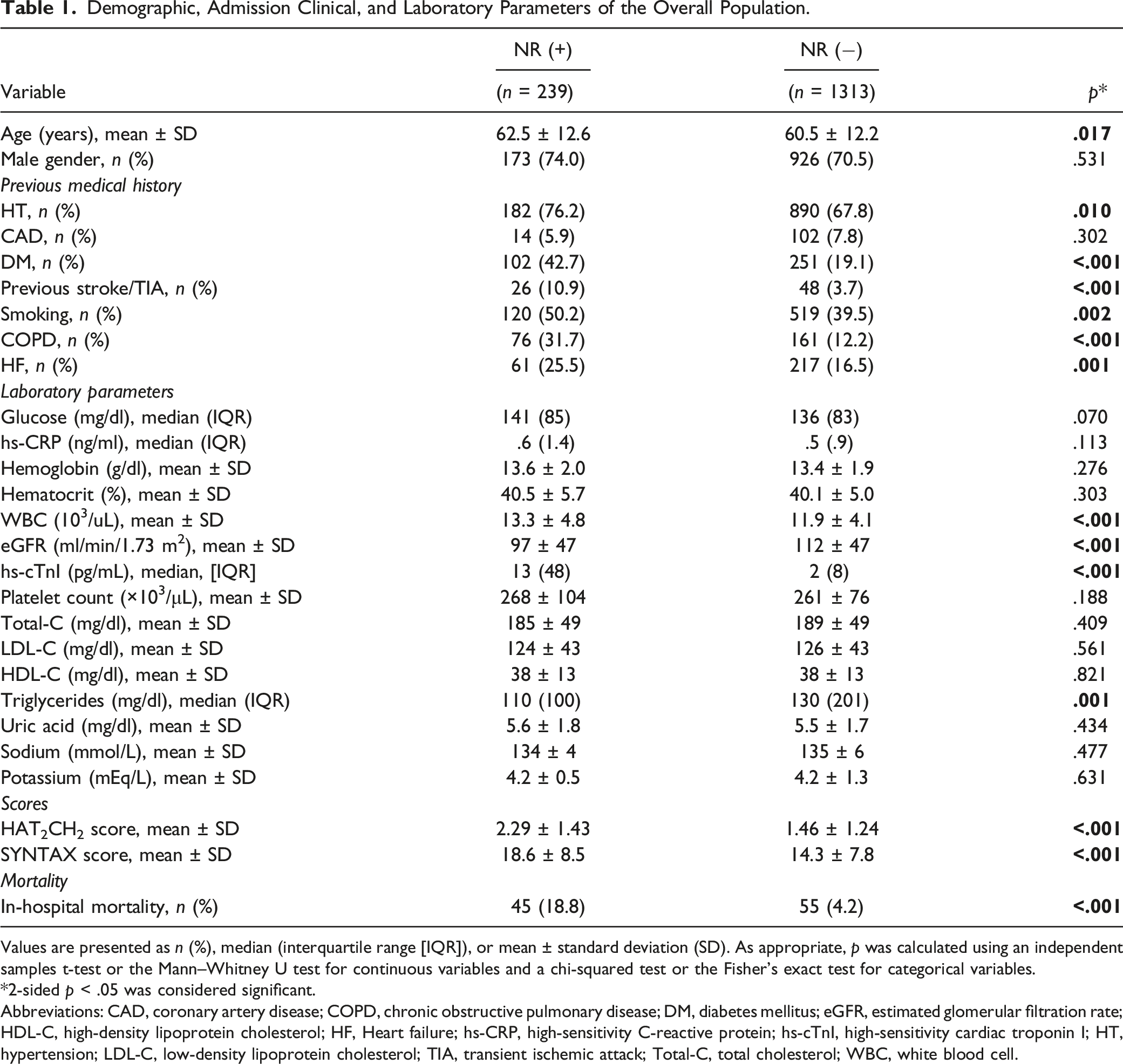
Values are presented as n (%), median (interquartile range [IQR]), or mean ± standard deviation (SD). As appropriate, p was calculated using an independent samples t-test or the Mann–Whitney U test for continuous variables and a chi-squared test or the Fisher’s exact test for categorical variables.
*2-sided p < .05 was considered significant.
Abbreviations: CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; HF, Heart failure; hs-CRP, high-sensitivity C-reactive protein; hs-cTnI, high-sensitivity cardiac troponin I; HT, hypertension; LDL-C, low-density lipoprotein cholesterol; TIA, transient ischemic attack; Total-C, total cholesterol; WBC, white blood cell.
Angiographic and Procedural Features.
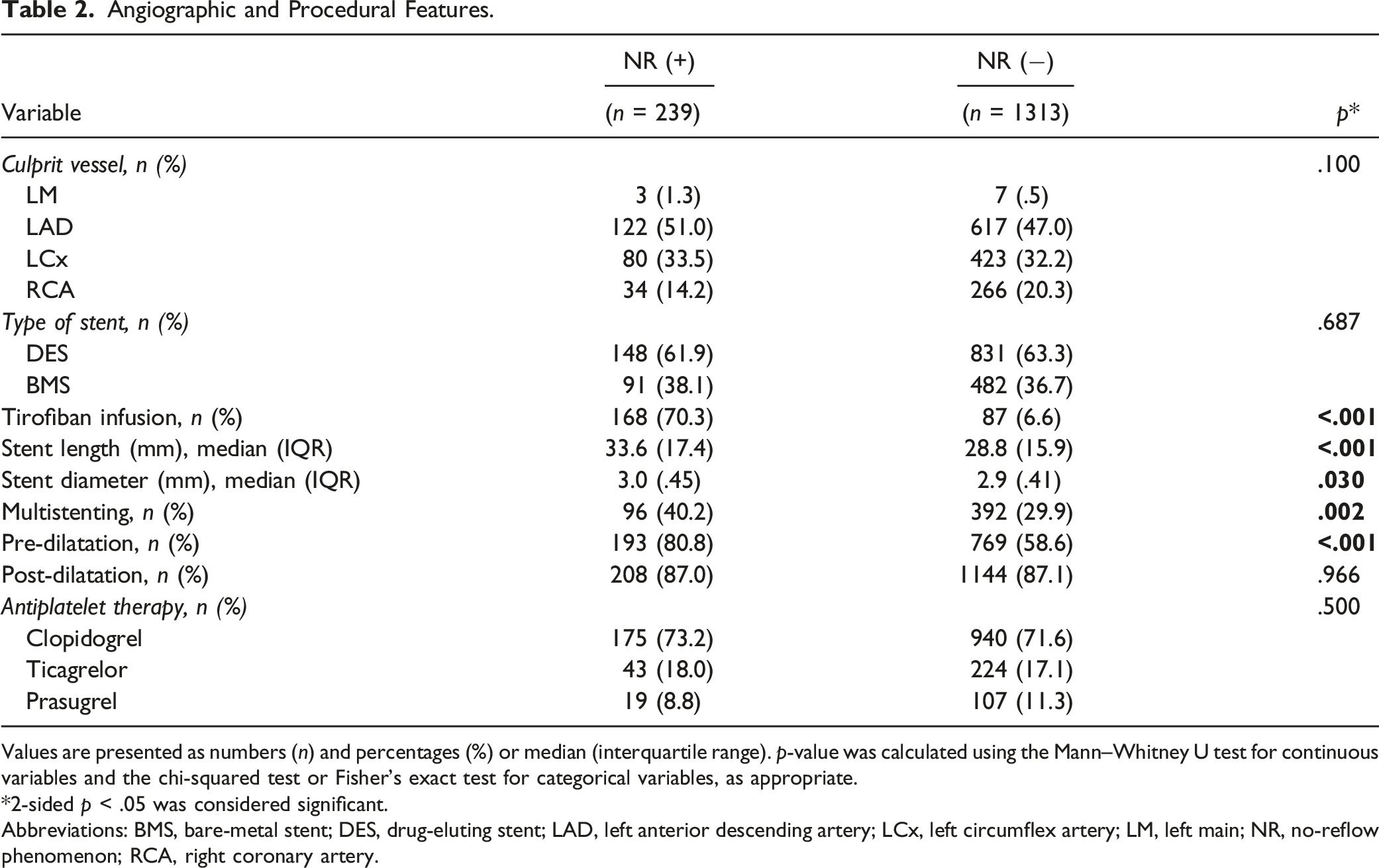
Values are presented as numbers (n) and percentages (%) or median (interquartile range). p-value was calculated using the Mann–Whitney U test for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables, as appropriate.
*2-sided p < .05 was considered significant.
Abbreviations: BMS, bare-metal stent; DES, drug-eluting stent; LAD, left anterior descending artery; LCx, left circumflex artery; LM, left main; NR, no-reflow phenomenon; RCA, right coronary artery.
Univariable and Multivariable Analysis of the No-Reflow Phenomenon in STEMI Patients Undergoing pPCI.
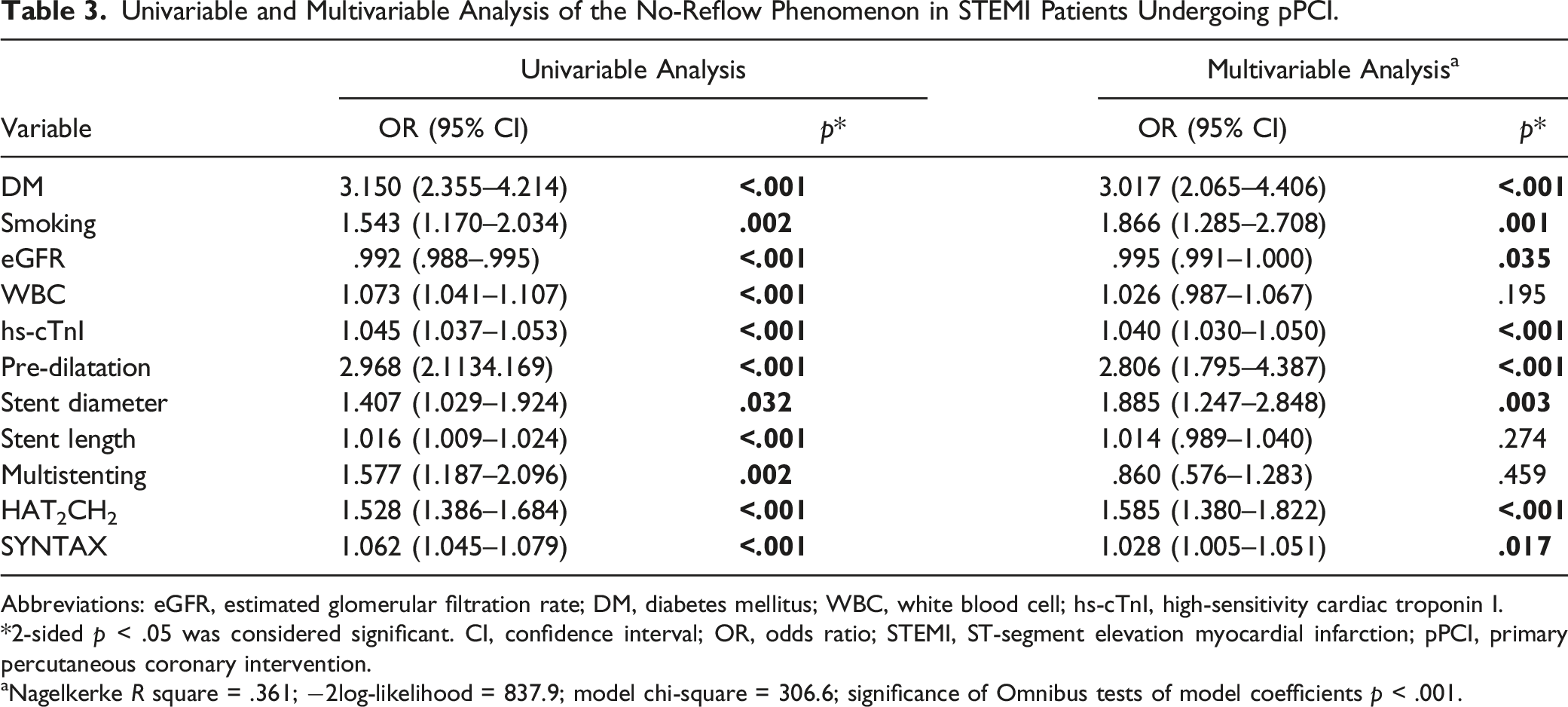
Abbreviations: eGFR, estimated glomerular filtration rate; DM, diabetes mellitus; WBC, white blood cell; hs-cTnI, high-sensitivity cardiac troponin I.
*2-sided p < .05 was considered significant. CI, confidence interval; OR, odds ratio; STEMI, ST-segment elevation myocardial infarction; pPCI, primary percutaneous coronary intervention.
aNagelkerke R square = .361; −2log-likelihood = 837.9; model chi-square = 306.6; significance of Omnibus tests of model coefficients p < .001.
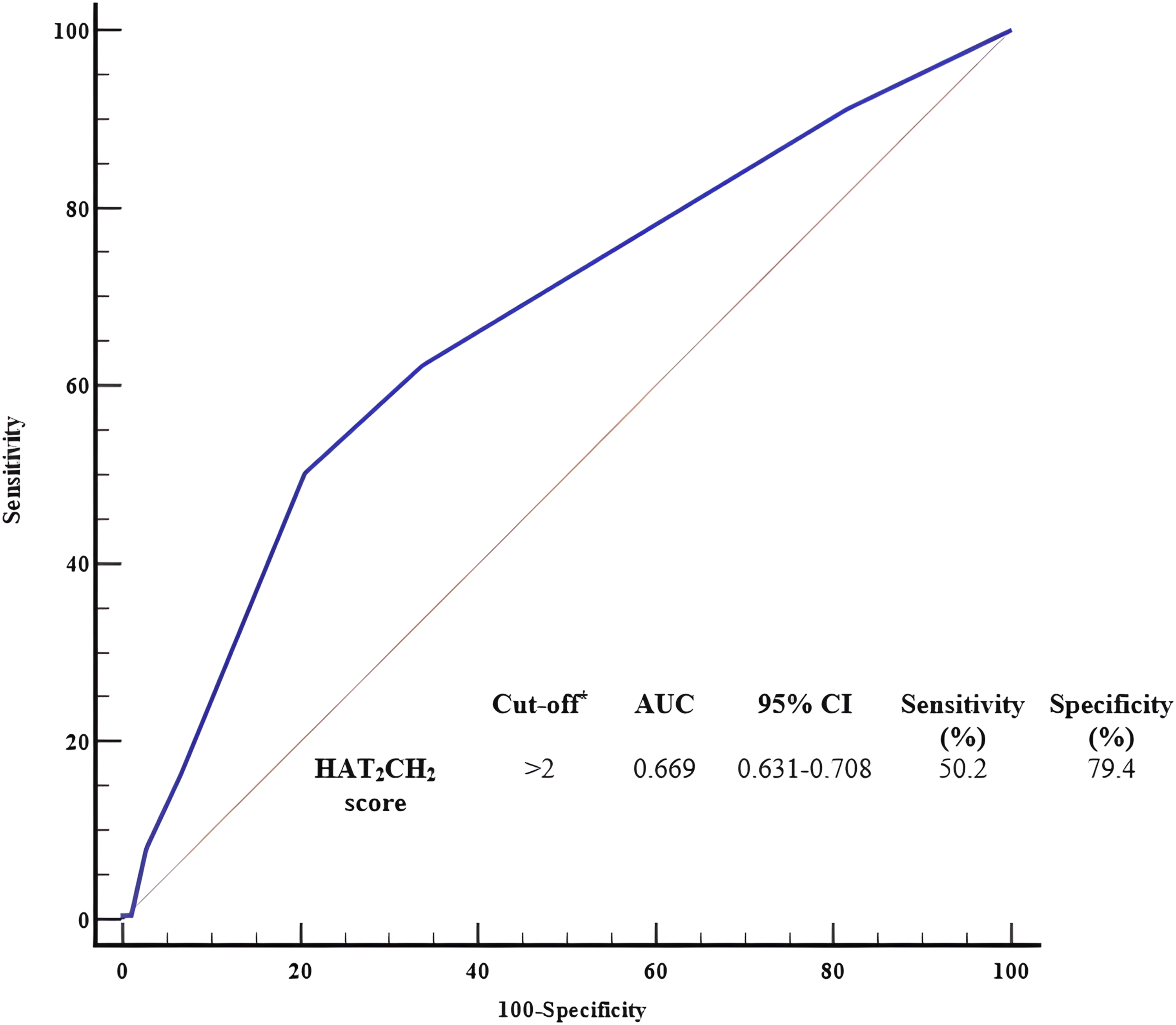
Receiver operating characteristic curve analysis of the HAT2CH2 score for determining the coronary no-reflow phenomenon in patients with STEMI undergoing pPCI. * The Youden index was used to identify the cutoff value. Abbreviations: AUC, area under the curve; CI, confidence interval.
Discussion
The main findings of the present study were as follows: (i) NR was observed in 15.4% of STEMI patients who underwent pPCI, (ii) The participants were predominantly elderly and male, (iii) HAT2CH2 score, SXscore, hs-cTnI, DM, smoking, eGFR, stent diameter, and pre-dilatation were independent predictors of NR in STEMI patients undergoing pPCI, and, (iv) The HAT2CH2 score with a cutoff >2 may be used as a determinant of NR with 50.2% sensitivity and 79.4% specificity.
Primary PCI is the main approach to revascularization for STEMI patients. The immediate decrease in distal blood flow following the procedure, despite stenting of the infarct-related artery, could, on the other hand, result in unfavorable consequences known as NR. 14 Although there are several proposals based on experimental methodologies and expert opinions to address this issue, no established therapy protocol has yet to be defined.15,16 Despite advancements in percutaneous treatment devices, procedures, and related medical practices, 11–41% of STEMI patients treated with pPCI may develop NR with large infarct size, HF, severe clinical events, and death.17,18 NR has been demonstrated to be a powerful independent predictor of in-hospital death in STEMI patients. 19 NR occurred at a rate of 6.4% in the present study, similar to previous studies. Furthermore, mortality rates (18 vs 4%, p < .001) were found to be higher in patients who developed NR. It should be noted, nonetheless, that a wide variety of demographic, laboratory, and procedural factors have been proven to influence the development of NR.20–24
Several studies have shown a link between AF-related stroke risk scoring systems, which are often used in cardiology, and NR in acute MI patients. Independent of AF and stroke risks, the impact of stroke risk scoring system components on coronary artery events was also examined. 25 Similarly, the relationship of CHA2DS2-VASc (congestive heart failure, HT, age [≥65 = 1 point, ≥75 = 2 points], DM, stroke/transient ischemic attack [TIA] [2 points], and vascular disease [peripheral arterial disease, previous MI, and aortic atheroma], sex category [female sex = 1 point]) and its modified forms with NR in MI patients has been established.26–28 Previous research has also demonstrated the NR connection of another risk score, ATRIA (the Anticoagulation and Risk Factors in Atrial Fibrillation), and its modified versions. 29 The HAT2CH2 score, based on the patient’s age and the presence of HT, stroke or transient ischemic attack, COPD, and HF, was developed in 2010 to identify patients likely to progress to sustained forms of AF. 10 The HAT2CH2 score, in other words, is a scoring system that intends to demonstrate the development of chronic disease and advanced age-related risk factors to new AF without relying on laboratory results. In our analysis, a high HAT2CH2 score was found to be highly related to NR. Moreover, all of the components of the score are risk factors having prognostic significance in STEMI. In light of the similarities between the main risk variables and the underlying mechanisms of NR, it might be claimed that our study provided the first evidence in the literature that the HAT2CH2 score had predictive significance for NR. Likewise, DM, smoking, and troponin, which have demonstrated impacts on the NR with the potential to impair microvascular coronary flow, were predictors of NR development in our investigation, similar to prior studies.30–34
It has been revealed that procedural features in coronary angiography may have a role in the pathogenesis of NR. For example, in one study, direct stent implantation without pre-dilatation significantly decreased the risk of NR development (12 vs 5%, p = .008). 35 Likewise, we showed that pre-dilatation has been an independent predictor of NR. In addition, as in the literature, stent diameter and high SXscore score were found to be associated with NR.13,36,37
SXscore is an anatomical scoring system that indicates the severity of coronary artery disease. This scoring system has been linked to short- and long-term morbidity and mortality in acute MI patients.38–41 Various mechanisms have been proposed for the association between SXscore and NR. Severe coronary artery disease is an indication of impaired microcirculation. 42 On the other hand, as lesion complexity increases, so does oxidative stress, and vasodilator response becomes insufficient. 43 This may impede epicardial coronary flow due to reduced microcirculation and poor vasodilator response. Furthermore, if the donor artery, which may supply insufficient blood flow to the infarct-related artery through the ipsilateral and contralateral retrograde route, is dysfunctional, reflow and associated consequences will be absent because collateral circulation to the microvascular bed is limited. Briefly, NR continues to be a significant issue and an indicator of poor outcome in MI patients.
Before PCI, it may be helpful to identify patients who are likely to develop NR. Although the HAT2CH2 score has been recently developed to determine the risk of AF, it may also estimate the development of NR. In individuals who have higher HAT2CH2 scores, the likelihood of coronary microvascular dysfunction and NR should be kept in mind, and treatments to increase coronary flow in the perioperative period should be adopted if coronary complications arise. In addition, efficient management of comorbid diseases that impair concomitant microvascular flow in patients with high HAT2CH2 scores becomes increasingly important in the postoperative phase. Eventually, the score can serve as a simplified tool for rapid risk assessment on admission, contributing to the identification of patients at high risk of developing NR as well as guiding early treatment and close follow-up since it allows documentation of the presence of cardiovascular, cerebrovascular, and pulmonary system diseases with a concise scoring system and includes risk factors similar to atherosclerosis and microvascular dysfunction.
Limitations
The retrospective and single-center study design was the most notable limitation of the study. Therefore, caution should be exercised about the generalizability of the results. We were unable to include other confounding factors such as intraprocedural hemodynamics, medications administered, and extended laboratory findings in our data. Furthermore, factors that may provide information regarding the cause-effect relationship, such as thrombus aspiration, intra-aortic balloon pump, intravenous ultrasonography, or fractional flow reserve analysis, could not be presented. Finally, we could not compare the HAT2CH2 score to other scores to examine its association with NR and discriminative ability. This issue could be an attractive area for further research.
Conclusion
We demonstrated that the HAT2CH2 score, which is used to identify new-onset AF in a variety of clinical settings, has strong evidence for predicting the occurrence of NR, a vital and prevalent consequence of MI. Therefore, the HAT2CH2 score, which is simple and practical to use, may facilitate prognostic stratification at the first medical contact without the need for further laboratory tests.
Footnotes
Author Contributions
HARBALLIOĞLU H, ALICI G, YILDIRIM A, and GENÇ Ö carried out the studies, participated in collecting data, and drafted the manuscript. QUISI A, ALICI G, and GENÇ Ö performed the statistical analysis and participated in its design. GENÇ Ö, HARBALIOĞLU H, QUISI A, ALICI G, and YILDIRIM A participated in the acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was carried out according to the recommendations set forth by the Declaration of Helsinki on biomedical research involving human subjects. The study was approved by the ethics committee of Adana City Training and Research Hospital (21.04.2022, decision No: 1897). Due to the retrospective design, informed consent was not required according to the ethics committee rules.
Data Availability
The analyzed datasets are available from the corresponding author upon reasonable request.