
Abstract
This study evaluated the role of the C-reactive protein (CRP)/albumin ratio (CAR) in estimating the probability of occurring contrast-induced nephropathy (CIN) after carotid artery angiography (CAAG). Patients (n = 410) who had CAAG for carotid artery stenosis (CAS) were included in this study. A spike in serum creatinine was used to define CIN within 72 h of the procedure (>.5 mg/dL or >25% above baseline). CAR was calculated by dividing the CRP by the albumin level. Patients with CIN had higher numbers of white blood cells (P = .002), numbers of neutrophils (P = .007), neutrophil–lymphocyte ratios (P = .026), high-sensitivity CRP levels (P < .001), and CAR levels (P < .001) than those without CIN. They were also older (P < .001) and more likely to have diabetes mellitus (P = .006) and hypertension (P = .016). According to receiver operator characteristic curve (ROC) analysis, the CAR value has a 75% sensitivity and a 68% specificity for identifying CIN at a cutoff of 1.8. Also, NLR and CRP predicted CIN with 71% sensitivity and 67% specificity, 71% sensitivity and 66% specificity at the best cutoff values of 1.96 and 7.91, respectively. According the present study, in patients with CAS, the development of CIN after CAAG is independently correlated with CAR at admission.
Keywords
Introduction
Symptomatic carotid atherosclerotic stenosis is among the most crucial risk factors for an ischemic stroke. 1 In recent years, the use of new inflammatory markers has become increasingly common in the diagnosis, treatment planning and prognosis of cardiovascular (carotid/coronary/peripheral artery) diseases.2-5
Although non-invasive diagnostic tests (such as ultrasound, computed tomography angiography (CTA)) are the first tests to be requested in the diagnosis of carotid artery stenosis (CAS), digital subtraction angiography (DSA) is still the gold standard diagnostic method. Additionally, stenting of the carotid artery, among endovascular CAS therapeutic alternatives, has gained favor globally and has become a less invasive technique in recent years.6-10
An unreliable and delayed indication of contrast-induced nephropathy (CIN) is the serum creatinine (sCr) level. 11 Therefore, efforts to find biomarkers that perform better are ongoing, both for the prompt delivery of essential medication and for the early and reliable identification of CIN. 11 About 10% of acute renal failure (ARF) that develops in hospitals is caused by CIN, which is typically reversible acute renal damage. 12 Despite the success of percutaneous coronary and carotid procedures, the development of CIN increases mortality and morbidity, which drives up healthcare expenditures.13-15
Numerous factors, including renal vascular narrowing, reduced renal flow of blood, oxidative stress, and endothelial dysfunction, are involved in the pathogenesis of CIN. It is still unclear why some patients with comparable risk factors or contrast agent exposure developed CIN differently from those who did not.15,16
Previous research has shown that inflammation and various process of inflammation and their biomarkers are linked to CIN.17-22 The development of CIN after invasive vascular procedures is a significant complication; consequently, early risk assessment (eg, with new biomarkers) for CIN is crucial.
High-sensitivity C-reactive protein (hsCRP) is a positive acute phase reactant that significantly impacts atherosclerosis at all stages. 23 Decreased albumin levels, a negative acute phase reactant, are associated with increased cardiovascular diseases, independent of traditional risk factors. 24 The prognosis of patients with several inflammatory illnesses, that is, cardiovascular conditions, sepsis, cancer, acute pancreatitis, ulcerative colitis, and hepatitis B, is more accurately predicted by the CRP/albumin ratio (CAR), which has been introduced as a new parameter for inflammation.24-28 However, there is no evidence linking CAR levels to the emergence of CIN following carotid operations. Therefore, the present study evaluated the role CAR in determining the likelihood that CIN will develop after carotid artery angiography (CAAG).
Materials and Methods
Sample
This is a retrospective study and includes 410 patients undergoing CAAG and had CAS identified on Doppler in ≥50% between January 2016 and March 2022. All of the patients were symptomatic regarding carotid artery disease: 169 (41.2%) patients had a transient ischemic attack, 26 (6.4%) had amaurosis fugax, 112 (27.3%) had a stroke without sequelae, and 103 (25.1%) had sequelae. Carotid endarterectomy (CEA) was decided for 23 of 410 patients with carotid stenosis because aortic anatomy was not suitable. While carotid stenting was applied to the remaining 371 patients, medical follow-up was decided for 16 patients. CAAG was performed by experienced invasive cardiologists using the classical Seldinger technique from the femoral or radial artery in all patients.
Starting 12 h before the procedures and continuing for 24 h afterward, isotonic saline (.9%) at a rate of 1 mL/kg/h was administered to all patients. Nonionic and reduced osmolar contrast material (Iohexol, Omnipaque 350 mg/mL; GE Healthcare, Cork, Ireland) was used in all procedures. The local hospital ethics committee approved the study (Ethical number; 2021/170).
The study comprised patients undergoing CAAG whose sCr levels were assessed before and 2 days after CAAG. Patients who had coronary artery disease history, anemia, active infection or systemic inflammatory disease history, autoimmune or chronic inflammatory disease history, heart failure (ejection fraction <40%), and patients who used chronic anti-inflammatory drugs, nephrotoxic agents, and who had liver enzyme abnormalities (alanine aminotransferase >60 IU/L), and glomerular filtration rate <30 mL/min/1.73 m2 were excluded from the study.
A diagnosis of hypertension (HT) that is known to be recurring with blood pressure measures >140/90 mmHg on repeated measurements (≥2) or pharmacological therapy as described by the recommendations was considered to have HT.29,30 Diabetes mellitus (DM) was diagnosed in patients treated with diet, oral medicines, and insulin who had a fasting blood glucose of 126 mg/dL, a blood glucose level of 200 mg/dL or above at any time, or a history of the condition. Patients with total cholesterol levels >200 mg/dL, low-density lipoprotein cholesterol levels >130 mg/dL, or those who had already been diagnosed with and treated for hypercholesterolemia were classified as having the condition. Smokers are those who have smoked regularly for at least 6 months.
The North American Symptomatic Carotid Endarterectomy Study (NASCET) criteria were used to determine the degree of CAS angiographically. 31 Critical CAS were defined as symptomatic patients with a carotid DSA stenosis of 50% or more or asymptomatic patients with a carotid DSA stenosis of 70% or more, and these patients’ simultaneous carotid stenting was carried out.
Laboratory Assessments
All patients had venous blood samples drawn when admitted. sCr levels were assessed at baseline (before CAAG) and 48–72 h following the administration of a contrast agent. All standard biochemical assays, including glucose, serum albumin, CRP, lipid profile, and sCr, were conducted using an autoanalyzer (Roche Diagnostic Modular Systems, Tokyo, Japan). Automated hematology analyzer equipment (Sysmex K-1000 Hematology Analyzer, Guangdong, China) was used to test hematological parameters, including hemoglobin (Hb), platelet, white blood cell (WBC) counts, neutrophils, and lymphocytes. To conduct the analyses, we used absolute cell counts. The platelet/lymphocyte ratio (PLR) was calculated by dividing the platelet count by the lymphocyte count. The neutrophil/lymphocyte ratio (NLR) was calculated by dividing the neutrophil count by the lymphocyte count. By dividing the CRP level by the albumin level, CAR was calculated. Our hospital serum albumin and CRP reference ranges are 3.5–5.5 g/dL and 0–6 mg/L, respectively.
Within 48 h of being admitted to the hospital, two-dimensional echocardiographic tests were performed on each patient (Vivid S6; GE Medical System, Horten, Norway). Following universal norms, the Simpson method was used to calculate the Left Ventricular Ejection Fraction (LVEF). 32
Diagnosis of CIN
Within 48–72 h of all patients receiving the contrast agent, daily sCr concentrations were assessed in all individuals. A .5 mg/dL or 25% increase in sCr levels 48–72 h following exposure to a radiocontrast agent was used to define CIN. 33 Depending on whether the patients developed CIN or not, we categorized them as CIN (−) and CIN (+).
Statistical Analysis
Statistical analysis was carried out using SPSS 21.0 for Windows (SPSS Inc, Armonk, NY, USA). Using the Shapiro–Wilk test, we evaluated the distribution normality of the results. Depending on the distribution’s normality, descriptive data were presented as a mean with a standard deviation or a median (interquartile range, IQR). The Mann–Whitney U test compared quantitative variables with non-normal distributions, and the independent samples t-test was used to compare variables with normal distributions. The chi-square test compared the categorical variables (percentages and numbers). Using univariate analysis, the influences of numerous factors on the emergence of CIN were identified. Parameters with P < .10 in univariate analysis were added to multivariate regression analysis. Using a Receiver Operating Characteristic Curve (ROC) Analysis, we determined the threshold values for CAR, CRP, and NLR in predicting the development of CIN. As the ideal cutoff value, we decided on the value that the ROC analysis determined to have the maximum sensitivity and specificity values. A 2-sided P < .05 was considered significant.
Results
Demographic Characteristics of the Study Populations.
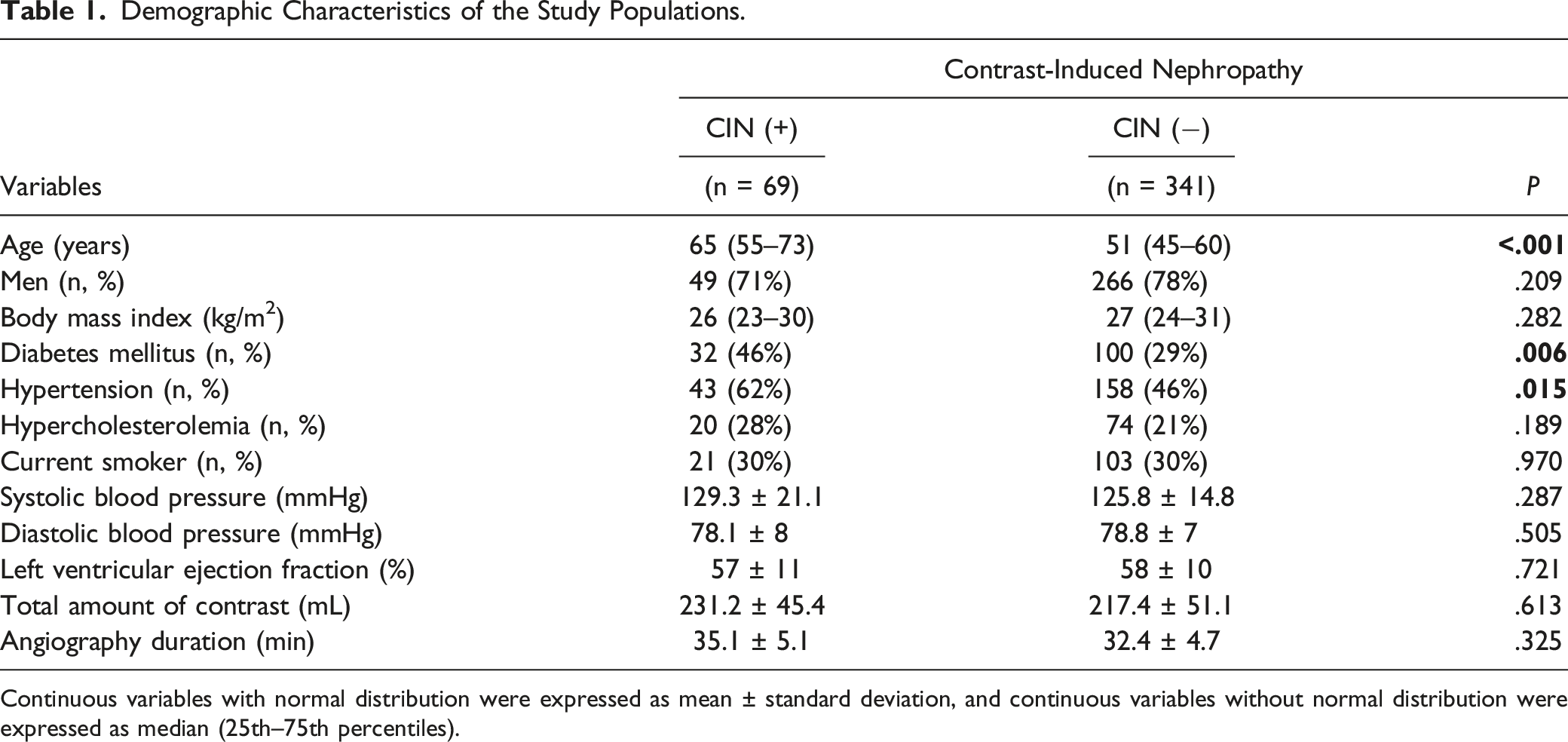
Continuous variables with normal distribution were expressed as mean ± standard deviation, and continuous variables without normal distribution were expressed as median (25th–75th percentiles).
Baseline Laboratory Findings of the Study Populations.
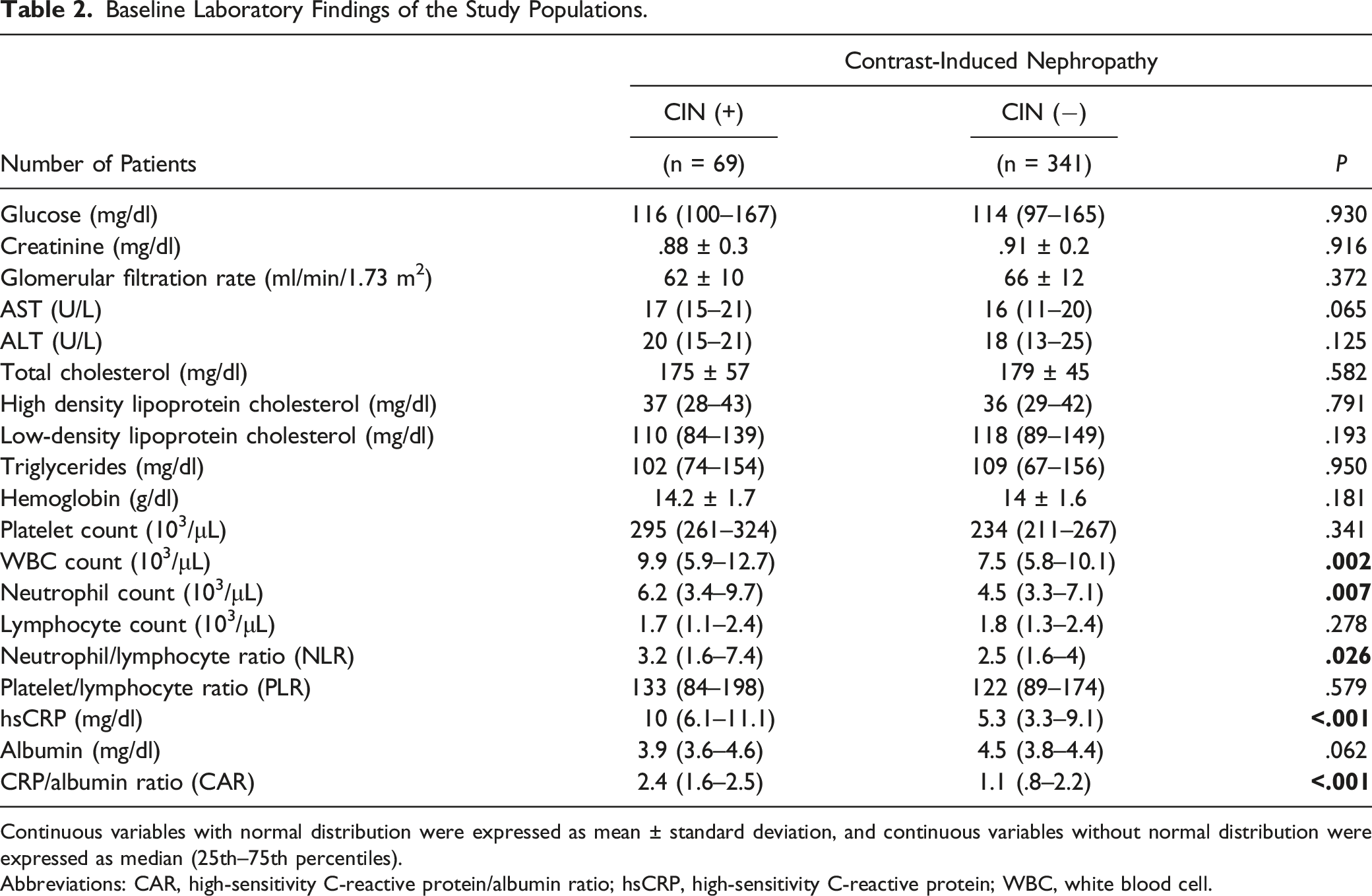
Continuous variables with normal distribution were expressed as mean ± standard deviation, and continuous variables without normal distribution were expressed as median (25th–75th percentiles).
Abbreviations: CAR, high-sensitivity C-reactive protein/albumin ratio; hsCRP, high-sensitivity C-reactive protein; WBC, white blood cell.
In addition, NLR, CRP levels, and CAR were all greater in CIN (+) patients compared with CIN (−) patients: 3.2 (1.6–7.4) vs 2.5 (1.6–4), P = .026, 10 (6.1–11.1) vs 5.3 (3.3–9.1) mg/L, P < .001, and 2.4 (1.6–2.5) vs 1.1 (.8–2.2), P < .001, respectively. Other laboratory results, however, did not reveal any statistically significant variations between the groups. Finally, there was no significant difference in the amounts of contrast agent used during the angiographic technique between the groups (P = .613; 231.2 ± 45.4 vs 217.4 ± 51.1).
Univariate and Multivariate Predictors of Contrast-Induced Nephropathy in Patients With Carotid Artery Stenosis.
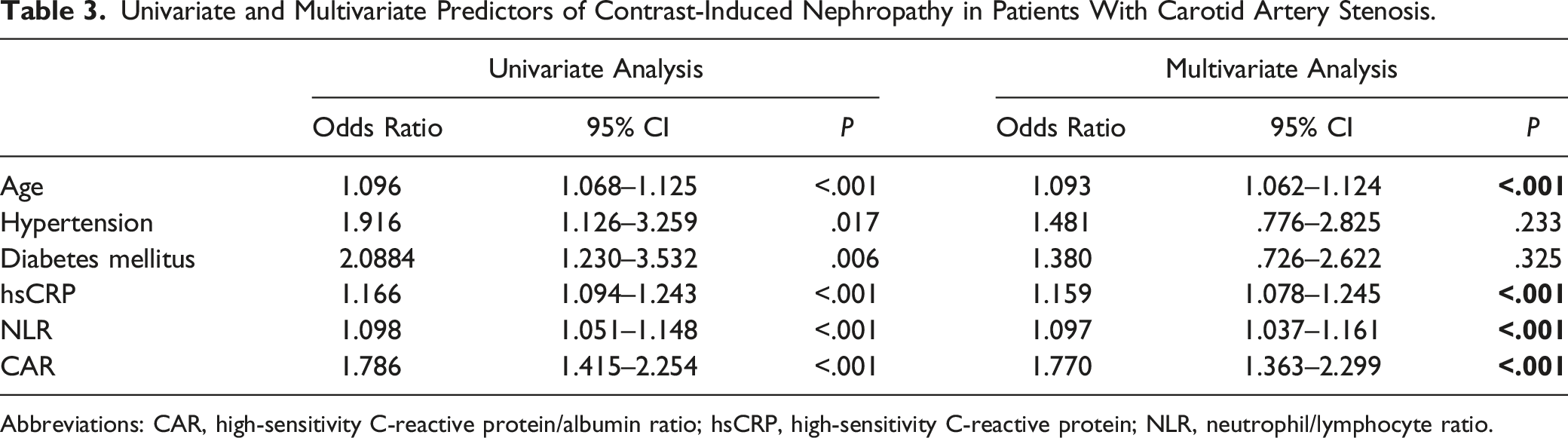
Abbreviations: CAR, high-sensitivity C-reactive protein/albumin ratio; hsCRP, high-sensitivity C-reactive protein; NLR, neutrophil/lymphocyte ratio.
According to ROC analysis, the optimal cutoff value for CAR to predict the onset of CIN was 1.8, with a 75% sensitivity and 68% specificity (area under the ROC curve = .726 (95% CI: .667–.786), P = .001). The optimal cutoff value for NLR was 1.96, which had a sensitivity of 71% and a specificity of 67% in predicting the development of CIN (area under the ROC curve = .585 (95% CI: .504–.665; P = .001). With a sensitivity of 71% and a specificity of 66%, the optimal cutoff value of 7.91 for CRP predicted the emergence of CIN (area under ROC curve = .716 (95% CI: .656–.777; P = .001)) (Fig. 1). Receiver operating characteristic curves for the CRP to albumin ratio, C-reactive protein, and neutrophil to lymphocyte ratio for predicting contrast-induced nephropathy.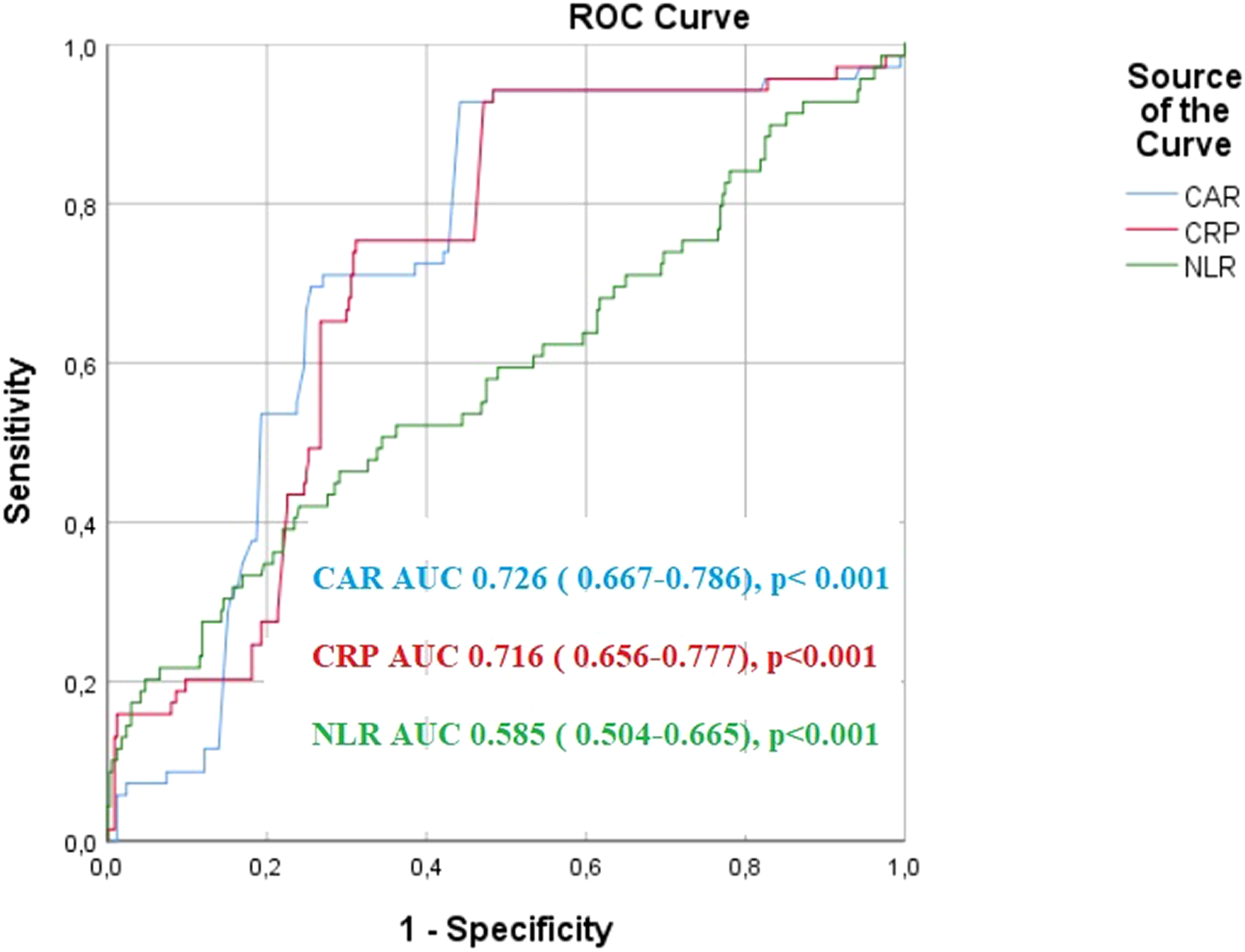
Discussion
The study’s most striking finding is that an increase in CAR (recently introduced as a marker of inflammation) in patients receiving angiography for CAS is a robust independent predictor of the development of CIN. To our knowledge, this is the first study showing a connection between CIN and CAR in patients undergoing CAAG.
The third most common factor contributing to ARF in hospitalized patients is CIN. 17 The use of contrast agents has increased due to the rise in diagnostic angiography and interventional procedures, which has increased the frequency of CIN in hospitalized patients. Consequently, CIN has received greater attention from clinicians and has become a more prevalent issue in daily practice. Patients at an elevated risk of having CIN have a 90% chance of developing ARF. This rate is <2% in patients with a low risk of developing CIN. 17 Despite the low frequency of CIN (1.6–2.3%) in procedures requiring a contrast agent; this probability increases when the contrast agent is administered intraarterially.34,35 However, this rate has been reported as 15–57% after CAAG.14,15,35 In the present study, 16.8% of the participants had CIN, consistent with previous studies. But compared to the literature, the amount of contrast material used in our study seems to be higher. Most of the patients in our study group underwent simultaneous carotid stenting immediately after the diagnosis of CAS. Therefore, a higher than normal amount of contrast was applied compared to the patients who were only diagnosed.
Identifying the risk of CIN before the procedure and/or determining the measures to minimize it is crucial because a worse prognosis, a greater risk of complications, a more extended hospital stay, and higher mortality rates are all linked to CIN.15,36 Currently, the recommended most successful strategy to prevent CIN seems to be intravenous and/or oral hydration, which we routinely employed in the study. 37
Even though the pathophysiological processes generating CIN are not clearly and completely understood, female gender, advanced age, HT, DM, and the presence of underlying chronic renal failure are the best-known risk factors for the development of CIN. 38 In our study, we have shown that advanced age, DM, and HT are predictors of the development of CIN. Despite these known risk factors, it is still challenging to determine which patients will develop CIN. Therefore, new biomarkers are needed to predict the development of CIN in patients scheduled for angiographic procedures.
Some factors, including low Hb levels, a decline in glomerular filtration rate, and an increase in serum uric acid level, have been found to predict the development of CIN following coronary artery imaging and percutaneous intervention.39-42 In addition, studies generally suggest that inflammation, increased inflammatory response, and oxidative stress play an essential role in the development and progression of CIN. The secretion of inflammatory mediators causes a decrease in glomerular filtration pressure, leading to sustained vasoconstriction of the intrarenal vessels. 43 The combination of oxidative stress and inflammation induces ischemic damage at the cellular level in the kidney and hence apoptosis. 43 Many markers have been defined to determine the risk of CIN development (Cystatin C, Neutrophil Gelatinase Associated Lipocalin (NGAL), L-type fatty acid binding protein (L-FABP), Kidney Injury Molecule (KIM)-1, Interleukin (IL)-18 etc.) However, their use is limited, and they are expensive methods.44-46 This situation has led to the investigation of parameters that can be easily measured and does not require complex or costly technologies. For this purpose, we focused on markers that are often overlooked by clinicians, such as NLR, PLR, and CRP, after coronary imaging and/or interventional procedures. These parameters have entered the literature as predictors of CIN.18-20,47-51 In our study, we found a significant relationship between the increase in NLR and the development of CIN, in line with the results of previous studies. However, this relationship could not be demonstrated with PLR.
CRP, a positive acute phase reactant, is one of the best-known and most researched inflammatory markers. It is considered an independent predictor of cardiovascular diseases, and it has been shown many times that increased CRP levels are associated with adverse cardiovascular outcomes.52,53 As mentioned before, a significant relationship between the increase in CRP level and the development of CIN was also present in our study. CRP levels were significantly higher in our group of patients who developed CIN.
Inflammation has been associated with decreased albumin synthesis and increased catabolism, identifying albumin as a negative acute phase reactant. 30 Decreased albumin levels are associated with increased cardiovascular diseases, such as heart failure and acute coronary syndrome, independent of traditional risk factors. 54 In addition, serum albumin levels can be correlated with blood flow and has been shown to be a useful parameter for determining disease severity in various patient groups. 55 Also, albumin levels have been found to be associated with thrombotic vascular processes.55,56 However, Murat et al. 30 showed that a decrease in serum albumin levels could predict the development of CIN after acute coronary syndrome. Although we found lower albumin levels in the CIN (+) group in line with previous studies, this was not statistically significant.
Many studies have shown that CAR is superior to CRP and albumin levels alone in cardiovascular diseases. Kelesoglu et al 57 found that increased CAR levels were associated with decreased coronary collateral circulation. Yıldırım et al. 58 claimed that the increase in CAR could be considered a potential index of the severity of carotid artery disease and could be an independent risk factor for severe CAS. Another study showed the relationship between increased CAR and the extent of coronary artery in patients with non-ST elevation myocardial infarction (NSTEMI). 26 Satilmis et al. 45 claimed that a high CAR in patients with NSTEMI and Altiparmak et al. 59 in stable angina pectoris patients could predict CIN after coronary angiography.
Our study suggests that using a combination of biomarkers may be a more sensitive parameter in determining the risk of CIN. A pronounced inflammatory response will lead to a significant increase in CAR, which may more reliably predict the risk of acute kidney injury. According to ROC analysis results CAR is a more sensitive marker for determining the CIN development than NLR alone. But CAR was marginally, but not significantly different, than using CRP alone. Both elevated CRP and low albumin support a possible link between systemic inflammation burden and endothelial dysfunction, oxidative stress, and renal vasoconstriction, explaining CIN after contrast exposure. 43
Our results also partially support the investigation by Karabag et al, 60 claiming that CAR is a strong predictor of the development of CIN in patients with STEMI undergoing primary percutaneous coronary intervention. Larger studies are needed to show whether CAR really has a significant advantage over CRP alone in predicting CIN.
Study Limitations
The most important limitation of this study is that it is both a single-center and a retrospective study. In addition, relatively few patients were included. We only calculated CAR at the start of the study, so we do not know the CAR changes that may occur during patient follow-up and the effect on our results. In addition, because we did not have a follow-up, we may have overlooked CINs, which developed after 72 h. Although a high CAR is an effective predictor of CIN, we cannot make a claim as to whether this has an impact on guiding the treatment approach. Multicenter studies with a large number of patients are needed.
Footnotes
Author Contribution
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.