
Abstract
Chronic venous insufficiency (CVI) causes severe symptoms and complications in the general population, but the prevalence, related risk factors, and treatment of CVI are unknown among nurses. The demographics and occupational factors of nurses from a university hospital were collected by questionnaires, and the presentation of CVI was confirmed by the specialist vascular surgeons. A total of 1606 participants were enrolled, and the prevalence of CVI was 7.5%. After multivariate adjustment, CVI was positively related to deep venous thrombosis history (OR 6.44, 95% CI 2.73-15.22), increased standing time (OR 2.21, 95% CI 1.20-4.10), and increased time in night shift rotation (OR 2.01, 95% CI 1.29-3.14). CVI was negatively related to oral contraceptives (OR .43, 95% CI .21-.87). Of the participants, 72.5% with CVI received compression therapy. For them, wearing compression stockings with a pressure of >20 mmHg or for >4 h/day significantly increased the rate of symptom relief, while the length of compression stockings made no difference. Thus, it was beneficial for nurses to spend less time standing and shorten their time in night shift rotation. Wearing compression stockings with sufficient pressure and for enough time was recommended for CVI symptom relief.
Background
Chronic venous insufficiency (CVI) indicates the more advanced forms of chronic venous disease (CVD), including edema, skin changes, or venous ulcers, corresponding with C3 to C6 of the Clinical, Etiological, Anatomical, Pathophysiological (CEAP) classification. 1 A recent study reported that CVI affected 13.4% of the global population. 2 If not treated, CVI will cause severe symptoms and complications which can lead to decreased quality of life, loss of working days, and health care costs. 3 It is also a strong predictor of all-cause death independent of the concomitant clinical profile and medication. 4
Recent studies found that age, female sex, overweight, prolonged standing, and family history are risk factors for CVD in the general population.5-8 Thus, nurses who are mostly female and spend a long time standing during work are at high risk of CVD. The prevalence of CVD in the nurse population was reported to be 34-69.1%,9-11 but there is no study investigating the prevalence and risk factors of CVI in the nurse population, which affects their work and life more seriously. Besides, compression therapy is recommended for patients with CVI, 12 but how it is applied in the nurse population with CVI is unknown. Given these gaps in knowledge, we conduct a survey in a university hospital with the aim to investigate the prevalence, risk factors, and compression therapy of CVI in this selected nurse population.
Methods
Study Participants
The investigation was conducted from September 2021 to April 2022 in West China Hospital and was approved by the ethical committee. Nurses from different clinical workstations were invited to participate, and those who answered the questionnaires were included in the study. Written consent was obtained from each participant prior to the questionnaire. Anyone who was currently pregnant or began nursing practice <1 year before was excluded from the study.
Data Collection
The data were collected by electronic questionnaires, which consisted of demographics and occupational factors. Specifically, the demographics included age, gender, height, weight, smoking status, bowel habit, marital status, parity, family history of CVD, and medical histories such as hypertension, oral contraceptive medication, lower limb fracture, and deep venous thrombosis (DVT). Occupational factors were composed of the work experience (years), working hours in standing posture, education level, job type, and night shift status. The job type was classified into clinical or management posts. The time in standing posture during work was reported by each individual according to their average standing hours in the last 6 months. For the participants with CVI, compression therapy was further investigated. The use of compression therapy was defined as regular wearing of compression stockings ≥3 times/week during work. The information about pressure at the ankle, wearing time, and length of stockings were collected, as well as the symptom relief after using compression stockings.
Outcome
The outcome was CVI, which was defined as clinical classes C3 to C6. During the investigation, several specialist vascular surgeons clinically examined the participants and confirmed the clinical classification for each individual based on the CEAP classification. 13 Due to the huge number of participants, ultrasound examinations were not possible to perform to further assess etiology, anatomy, and pathophysiology.
Statistical Analysis
Continuous variables were described as median with interquartile range (IQR), and they were compared with the Mann-Whitney U test. Categorical variables were analyzed using χ2 tests or Fisher’s exact tests, as appropriate. Logistic regression analysis was applied for univariate and multivariate analyses of risk factors for CVI. Variables with P < .05 in univariate analysis or considered to have clinical significance were included in the multivariate analysis using a stepwise method. All statistical analyses were performed using the RStudio (Boston, MA, USA). A two-sided P < .05 was considered significant.
Results
Characteristics of Participants
Distribution of Clinical Classification According to CEAP Classification 13 (n = 1606).
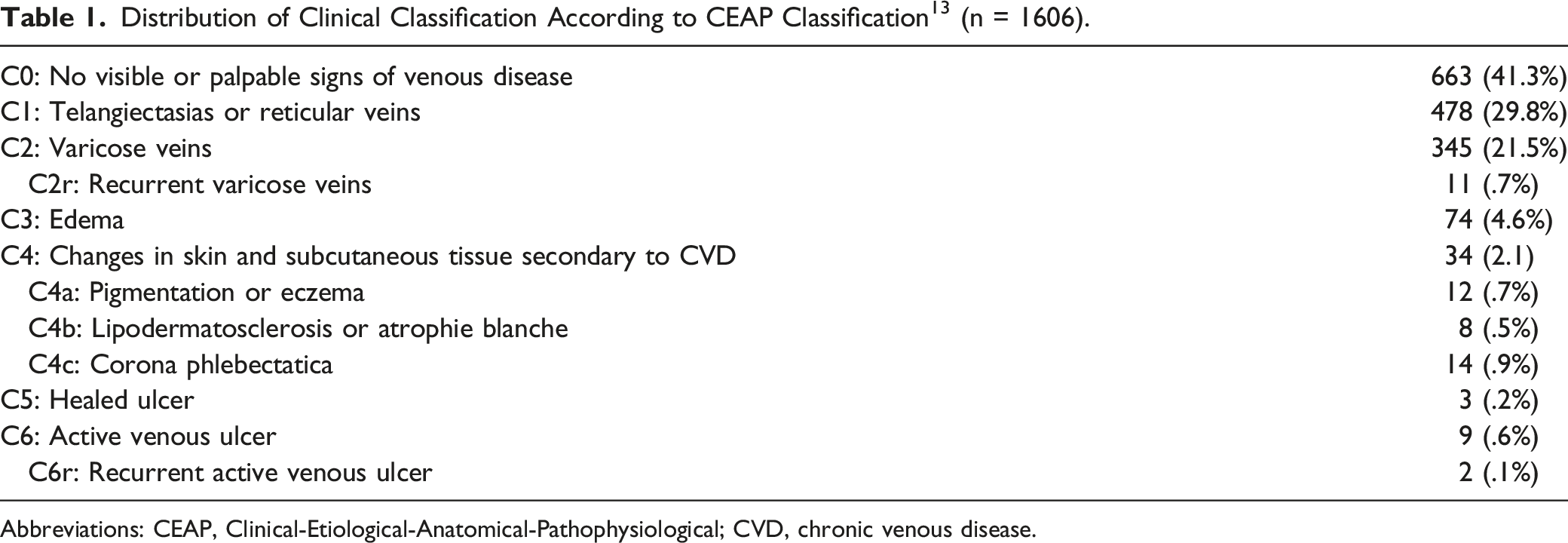
Abbreviations: CEAP, Clinical-Etiological-Anatomical-Pathophysiological; CVD, chronic venous disease.
The Characteristics of the Nurse Population.
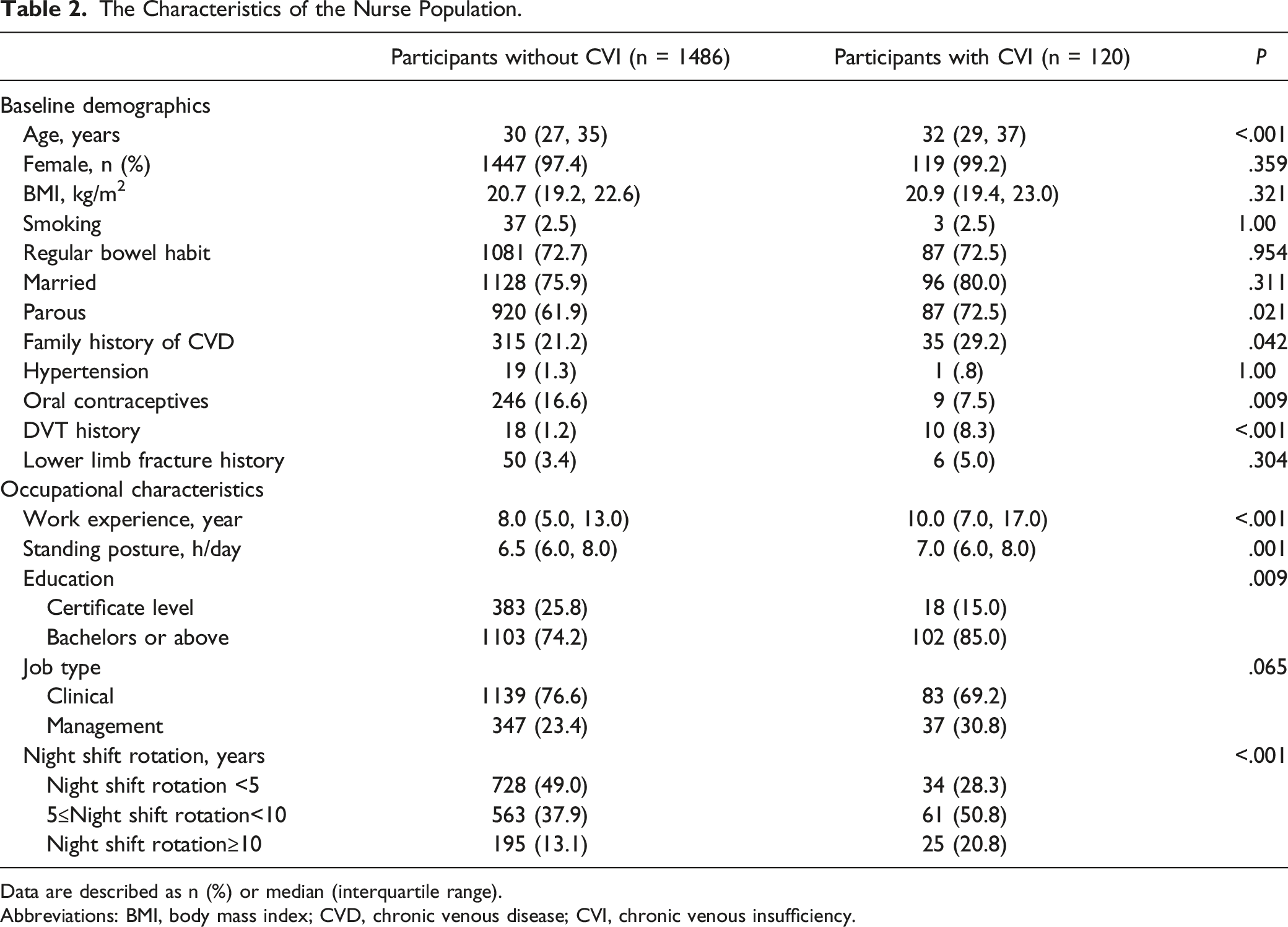
Data are described as n (%) or median (interquartile range).
Abbreviations: BMI, body mass index; CVD, chronic venous disease; CVI, chronic venous insufficiency.
As shown in Table 2, the participants also reported their occupational characteristics. For all the participants with CVD, the median years of work experience were 8.0, and the median hours of working in standing posture/day were 6.5. They were both significantly longer in the CVI group (10.0 vs 8.0 years, P < .001 and 7.0 vs 6.5, P = .001 h, respectively). Besides, more participants had higher education levels in the CVI group (85.0 vs 74.2%, P = .009). The night shift rotation was reported as 3 types, <5 years, 5 to 10 years, and >10 years; 49.0% of the participants without CVI worked in the night shift rotation for <5 years, however, it was only 28.3% in the CVI group.
Risk Factors of Chronic Venous Insufficiency
The correlation between variables and CVI was investigated by Logistic analysis. The univariate Logistic analysis revealed that with the increase in age, work experience, standing hours, and time in night shift rotation, the odds ratios (ORs) of having CVI increased. The prevalence of CVI also increased with these variables above (Figure 1). DVT history greatly increased the risk of CVI, with an OR of 7.41 (95% CI 3.34-16.45). Other variables like family history of CVD, parity, and higher education level were also positively associated with the increased risk of CVI. However, taking oral contraceptives was associated with a decreased risk of CVI, with an OR of .41 (95% CI .20-.82) (Table 3). The prevalence of chronic venous insufficiency increased with age (A), work experience (B), standing hours (C), and time in night shift rotation (D). Logistic Analyses of Potential Risk Factors Associated with Chronic Venous Insufficiency. Abbreviations: CVI, chronic venous insufficiency; OR, odds ratio; CI, confidence interval; DVT, deep venous thrombosis; Ref, reference.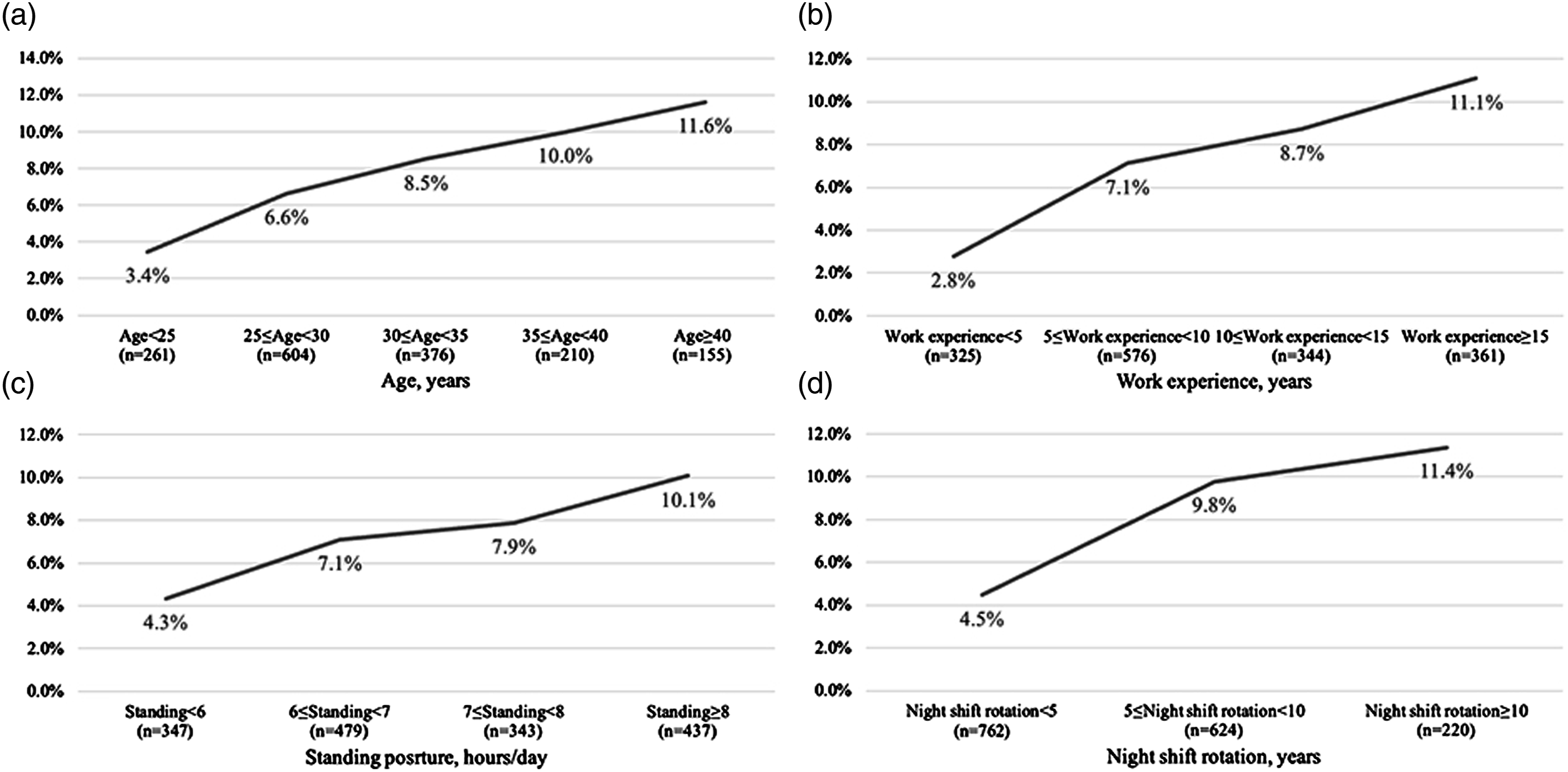
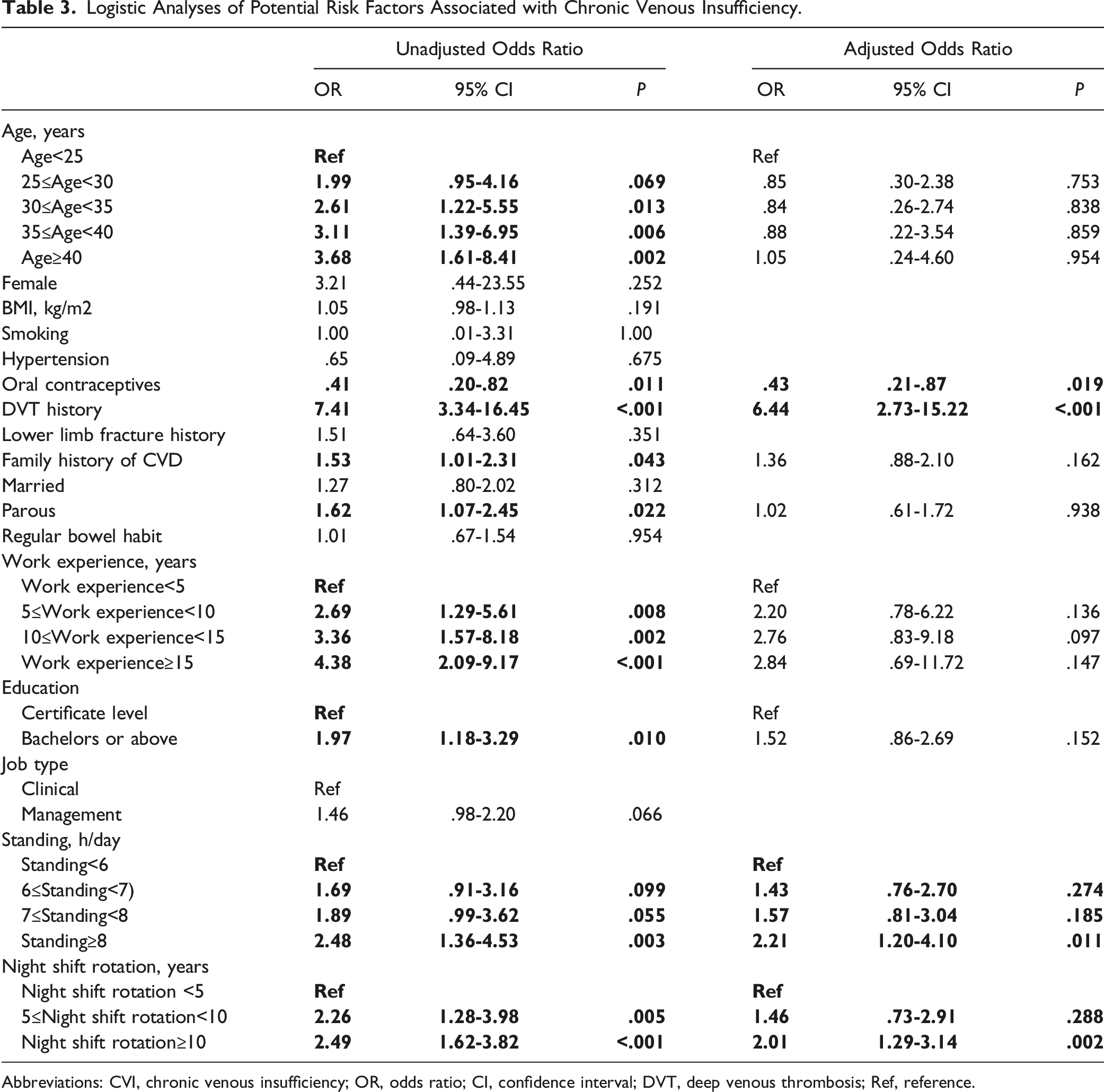
In the multivariate Logistic analysis, the effect of age, family history, parity, work experience, and education level on CVI were adjusted. History of DVT still greatly increased the odds of having CVI, with an adjusted OR of 6.44 (95% CI 2.73-15.22). When compared with those who stood for <6 h/day, there was a clear trend that the risk increased with the increase of standing time. When the standing time increased to >8 h, the difference was significant, with an adjusted OR of 2.21 (95% CI 1.20-4.10). Working in the night shift rotation also increased the risk of CVI. For the participants who worked 5-10 years in the night shift rotation, the adjusted OR was 1.46 (95% CI .73-2.91), and the risk was significant with the time increased, with an adjusted OR of 2.01 (95% CI 1.29-3.14). Taking oral contraceptives was the only protective factor for CVI, with an adjusted OR of .43 (95% CI .21-.87)
Compression Therapy of Chronic Venous Insufficiency
Among the participants with CVI, 87 (72.5%) of them claimed that they were using compression stockings during work; 48 (55.2%) of the CVI participants use compression stockings with a pressure >20 mmHg, and 53 (60.9%) of them wore compression stockings for >4 h during work. Additionally, 53 (60.9%) of them used knee-length compression stockings. For the 87 participants with CVI who used compression stockings, 65 (74.7%) of them suggested symptom relief after the use of compression stockings. The rate of symptoms relief was higher for the participants who used compression stockings with a pressure >20 mmHg (85.4 vs 61.5%, P = .011) or wore compression stockings for >4 h/day (84.9 vs 58.8%, P = .006), but it was not associated with the length of compression stockings (Figure 2). The rate of symptoms relief with compression stockings for participants with chronic venous insufficiency.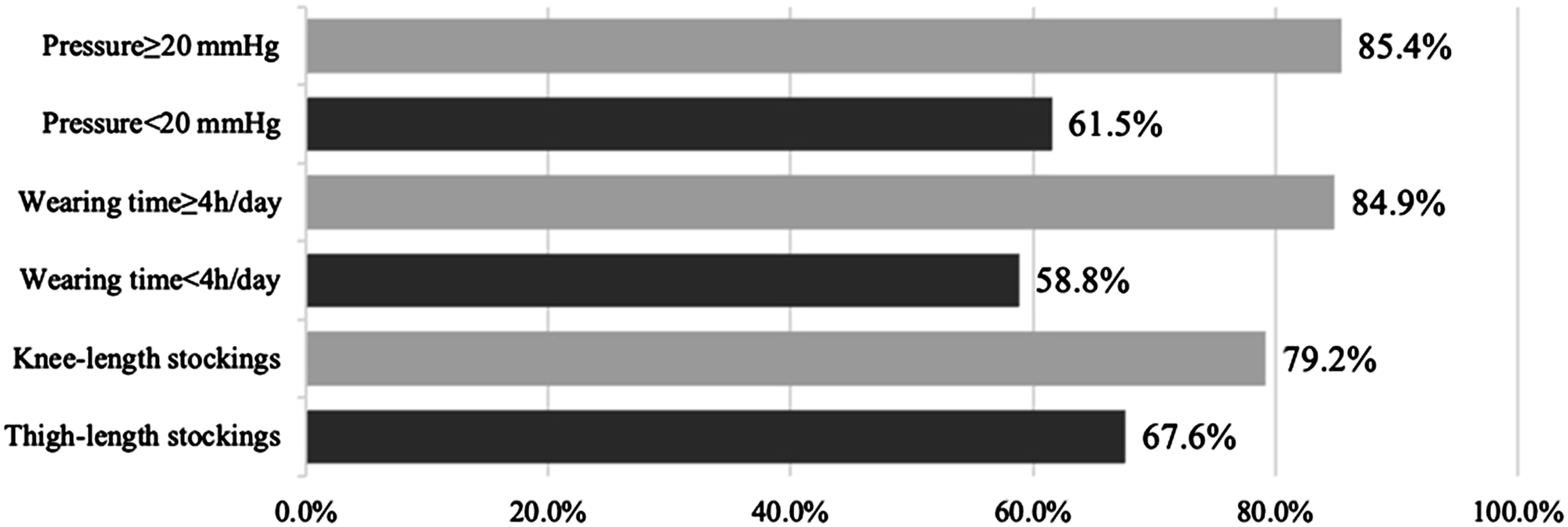
Discussion
In the present study is a cross-sectional investigation of the nurse population in a comprehensive university hospital. Unlike previous studies that only reported the prevalence of varicose veins or CVD in the nurse population,8,9,11 the present study firstly focused on the CVI which greatly affected their work and life. The main findings of this study were that: 7.5% of the nurse population was affected by CVI; DVT history, prolonged standing time, and night shift rotation were positively related to CVI in the nurse population while taking oral contraceptives was negatively related to CVI; compression therapy was applied for the majority of nurses with CVI during work, and using compression stockings with pressure >20 mmHg or wearing compression stockings for >4 h/day can more effectively relieve their symptoms.
The prevalence of CVI over the past few decades had been difficult to estimate due to varying and inconsistent standards of evaluation and diagnosis. In the Edinburgh Vein Study of venous disorders in the general population, CVI was defined as corona phlebectatica, distribution of hyper- or hypopigmented areas, and active or healed ulcer cruris, corresponding with C4 to C6 of CEAP classification. 14 The prevalence of CVI in that study was 9.4% in men and 6.6% in women. However, another study defined CVI as C1 to C6, resulting in a CVI prevalence of 69.1% in the health care workers in the United States. 9 Due to these conflicting standards, the current study defined CVI according to the most recent guidelines on the management of chronic venous disease, 1 and it presented a prevalence of 7.5% in the nurse population.
The Edinburgh Vein Study found the incidence of CVI rose significantly with age in the general population (21% in men >50 years, and 12% in women >50 years), 14 the Gutenberg Health Study also identified age as a clinical determinant of CVI. 4 The incidence of CVI rose with age greatly in our nurse population, from 3.45 to 11.61%. However, we interestingly found the association between CVI and age was not significant after adjustment, which was inconsistent with previous studies. The reason might be the different cohort, the age of our nurse population was younger, while the mean age in the Edinburgh Vein Study was 45 years, and the age in the Gutenberg Health Study ranged from 40 to 80 years.
The most powerful risk factor after adjustment was a history of DVT. Dysfunction of the deep venous system is a consequence of damage from previous DVT, which leads to rapid refilling by pathologic retrograde venous flow and may even reduce the blood volume exiting the lower limbs. Thus, DVT plays an important role in the pathogenesis of CVI.15,16 Another expected risk factor was prolonged standing, causing veins to become distended as the vein fills via antegrade flow, allowing the valves to open and pressure to increase, gradually promoting venous insufficiency. Several studies worldwide reported that prolonged standing increased the risk of having varicose veins in the nurse population.8,17,18
Night shift rotation was identified as an independent risk factor for CVI in the present study. Recent studies reported that nurses working in the night shift rotation showed a higher prevalence of varicose veins.19,20 However, no study explored the relationship between night shift work and CVI except the current 1. Brum et al 21 found that night shift workers sleep fewer hours, and had higher body mass index (BMI) compared with day shift workers. Based on this result, a hypothesis is that fewer sleep hours for night nurses leads to prolonged upright posture, coupled with higher BMI, which will increase the pressure on the venous system and eventually promote the progress of CVI.
Oral contraceptive medication was the only protective factor for CVI in the present study. However, the role of oral contraceptives in the venous system was uncertain. The studies by Fukaya et al 22 and Jukkola et al 23 reported the relationship between varicose veins and oral contraceptives. They found the use of oral contraceptives was a debated risk factor for varicose veins, which showed a small and not significant protective effect. It was worth noting that oral contraceptives confer a 2 to 4-fold increase in venous thrombosis risk, but because the baseline incidence of venous thrombosis is higher in older women, the absolute risk was lower in the younger oral contraceptive users. 24 Oral contraceptives that contain third-generation progestins even had a greater venous thromboembolic risk than those that contain levonorgestrel. 25 Based on these results, further well-planned investigations are warranted to find out if oral contraceptives are beneficial in preventing CVI.
Compression therapy was widely applied to the participants with CVI. Similar to the recent guidelines which recommended compression stockings exerting a pressure of 20-40 mmHg at the ankle to reduce edema and skin induration, 1 we found that compression stockings with a pressure >20 mmHg can significantly increase the rate of symptom relief. In addition, we found that wearing compression stockings for >4 h/day also increased the rate of symptom relief. Although the duration of compression therapy was not clearly defined in most of the guidelines, 26 it was reasonable that prolonged external compression can consistently oppose the hydrostatic forces of venous hypertension, which lead to symptom relief. In our investigation, more than half of the nurses with CVI did not wear compression stockings with qualified pressure or for enough time per day. Therefore, education on the better use of compression stockings should be emphasized in the nurse population. For the length of compression stockings, more nurses in the current study wear knee-length compression stockings, and there was no difference in symptom relief. This result was similar to the study of Lee et al, 27 that compared edema, pain, and satisfaction according to different lengths of compression stockings worn by female nursing students; no differences were found, but side effects appeared in participants wearing the thigh-length stockings. Besides, knee-length compression stockings were reported to be more comfortable, encouraging higher levels of adherence. 28 Thus, knee-length compression stockings might be suggested for nurses.
The present were study has some limitations. Firstly, due to the nature of the cross-sectional study, the reported risk factors were only related to CVI, but cause and effect cannot be determined. Well-planned case-control studies are warranted to determine the pathogenic factors of CVI. Secondly, the accuracy of data collected by electronic questionnaires may be affected, because they were self-reported by the participants, especially standing hours during work. The lack of ultrasound evaluation and quality of life assessment made us unable to verify the presence of venous insufficiency and the impact of CVI on nurses’ life. Finally, this investigation was conducted in a single center, where the nurses were young and almost all were women. Multicenter worldwide studies are needed.
Conclusion
CVI affected nearly one-tenth of the nurse population. Several risk factors for CVI were identified. It might be beneficial for the nurses to spend less time standing at work and try to shorten the time in night shift rotation. For the nurses already with CVI, wearing compression stockings with a pressure >20 mmHg and for >4 h/day is recommended for symptom relief.
Footnotes
Acknowledgments
We really appreciate the cooperation of the volunteered nurses in this investigation, and the help of vascular surgeons in the Department of Vascular Surgery, West China Hospital.
Author Contribution
All authors contributed to: (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and, (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Postdoctoral Science Foundation (2021M702352); 1•3•5 project for disciplines of excellence (ZYJC21078), West China Hospital, Sichuan University; Health Commission of Sichuan province program (21PJ044), and Sichuan International Science and Technology Innovation Cooperation Project (2021YFH0149).
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.