
Abstract
We investigated factors that affected perioperative, postoperative, and long-term outcomes of patients who underwent open emergency surgical repair of ruptured abdominal aortic aneurysms (RAAA). All patients who underwent open emergency surgical repair from 1990 to 2011 were included (463 patients; 374 [81%] male; mean age 74.7 ± 8.7years). Logistic and Cox regression analyses were performed to explore the association of variables with outcomes. Preoperatively, median (interquartile range) hemoglobin was 11.2 (9.5-12.8) g/dL, and median creatinine level was 140 (112-177) µmol/L. Intraoperatively, the median operative time was 2.25 (2-3) hours, and median estimated blood loss was 1.5 (0.5-3) L; 250 (54%) patients required intraoperative inotropes, and a median of 6 (4-8) units of blood was transfused. Median length of hospital stay was 11 (7-20) days. In-hospital mortality rate was 35.6%, and 5-year mortality was 48%. Age, distance traveled, operation duration, postoperative myocardial infarction (MI), and multi-organ failure (MOF) were predictors of in-hospital mortality and long-term outcome. Additionally, postoperative acute renal failure predicted in-hospital mortality. In patients with RAAA undergoing open surgical repair, the strongest predictors of in-hospital mortality and long-term outcome were postoperative MOF and MI and operative duration.
Introduction
The last 2 decades witnessed an increase followed by a sharp decrease in mortality resulting from ruptured abdominal aortic aneurysms (RAAA); the proportion of those patients offered and surviving emergency repair, probably, remains the same. 1,2 Undoubtedly, RAAA will always be the main contributor to mortality from AAAs, and emergency open repair of RAAA is still the gold standard, as randomized and long-term data showed no significant advantage for the endovascular option. 3 –9 Emergency open repair of RAAA has been associated with poor operative outcomes, with reported early mortality rates ranging from 13% to 53%. 5,10 –15
Several factors were found to have an effect on the morbidity, mortality, and survival following emergency open repair for RAAA. These include patient-related factors (eg, age, gender, comorbidities, level of consciousness, and preoperative biochemical profile), operative factors (blood loss, operating time, urine output, and technical issues), and the presence of postoperative complications. 10,13,16 –20
The treatment goal is to reduce the morbidity and mortality following repair of an RAAA. Therefore, it is useful to review the main predictors of outcomes after such an intervention to improve our care plan for patients admitted with an RAAA. The present study adds to the literature evaluating the perioperative variables that play a role in short- and long-term outcomes for patients who undergo emergency open surgical RAAA repair. It is based on a 20-year experience at a regional vascular surgical center in North-East Yorkshire (United Kingdom).
Methods
We identified all patients who underwent open surgical repair of RAAA during the last 20 years at the Hull Royal Infirmary in North East Yorkshire, United Kingdom. We retrieved records of patients admitted for RAAA from July 1990 to November 2011, using a locally developed, prospectively maintained database. Patients with symptomatic but intact aneurysms and those who underwent endovascular aneurysm repair (EVAR) of their RAAA were excluded.
Examination of the data was done thoroughly with reference to electronic data resources and patient case notes to verify the background clinical information retrieved. Basic preoperative, operative, and postoperative details were documented and current status checked (alive or dead).
Patient-specific variables analyzed were age, gender, hypertension (defined as an arterial pressure of ≥160/95 mm Hg or if the patient is on antihypertensive medications), smoking (current), diabetes (on oral hypoglycemic drugs or insulin), coronary artery disease (previously documented myocardial infarction [MI] and/or ongoing angina pectoris, ischemic changes on electrocardiogram and/or previous myocardial revascularization), chronic obstructive pulmonary disease (COPD) as documented in medical records and if the patient is on bronchodilators or steroids, cerebrovascular events (all grades of stroke, including transient ischemic attack), kidney disease (defined as a history of chronic or acute renal failure (ARF), or a serum creatinine level > 150 μmol/L), and drug history. Preoperative variables analyzed were presence of shock (defined as systolic blood pressure <80 mm Hg or hemodynamic instability), American Society of Anesthesiologists (ASA) score, and preoperative values of hemoglobin (Hb), white blood cell count, platelet count, urea, creatinine, and electrolytes. Preoperative blood pressure was measured on presentation and continuously monitored. Intraoperative variables analyzed were duration of operation, volume of blood loss (as documented in medical records and anesthetic charts), type of graft used, and intravenous fluid and blood volumes administrated (as documented in medical records and anesthetic charts). The outcome measures were immediate operative death, in-hospital, 1-year, and 5-year mortality as well as all morbidity data documented during hospital stay.
Statistical Analysis
Statistical Package for the Social Sciences Program (SPSS) version 19 for Windows (SPSS Inc, Chicago, Illinois) was used for statistical analysis. Continuous variables were expressed as mean ± standard deviation for parametric variables and median (interquartile range) for nonparametric variables. Categorical data were presented as the number of patients and percentage. Comparison between the groups was carried out using unpaired t test for parametric variables and Mann-Whitney U test for nonparametric variables. The χ2 test for trend and Fisher exact probability test were used for categorical variables as appropriate. Survival was calculated from the date of operation until the date of death or date of last follow-up. If patients did not attend for follow-up, the general practitioner was contacted to confirm survival status. Kaplan Meier survival function was used for survival analysis and the log-rank test was used for survival comparison between the 2 groups. Logistic regression was used to identify factors associated with in-hospital mortality. Only variables with P < .05 in the univariable analysis were included in the regression model. Cox proportional hazard regression model was used to identify factors associated with long-term outcome with inclusion of variables with P < .05 in univariable analysis. All statistical tests were 2 sided, and a P < .05 was considered significant.
Results
Between July 1990 and November 2011, a total of 463 patients underwent open repair of RAAA; mean age was 74.7 ± 8.7 years, 138 (30%) patients were aged ≥80 years, and 375 (81%) patients were males. The median ASA score was 4 (3-4). Intraoperatively, the median amount of transfused blood was 6 (4-8) units, and the supervising vascular consultant was present in theater for 460 (99.4%) operations. A polytetrafluoroethylene graft was used in 7.7%. The remainder preoperative, operative, and postoperative patient characteristics are presented in Table 1.
Preoperative, Operative, and Postoperative Patient Characteristics.
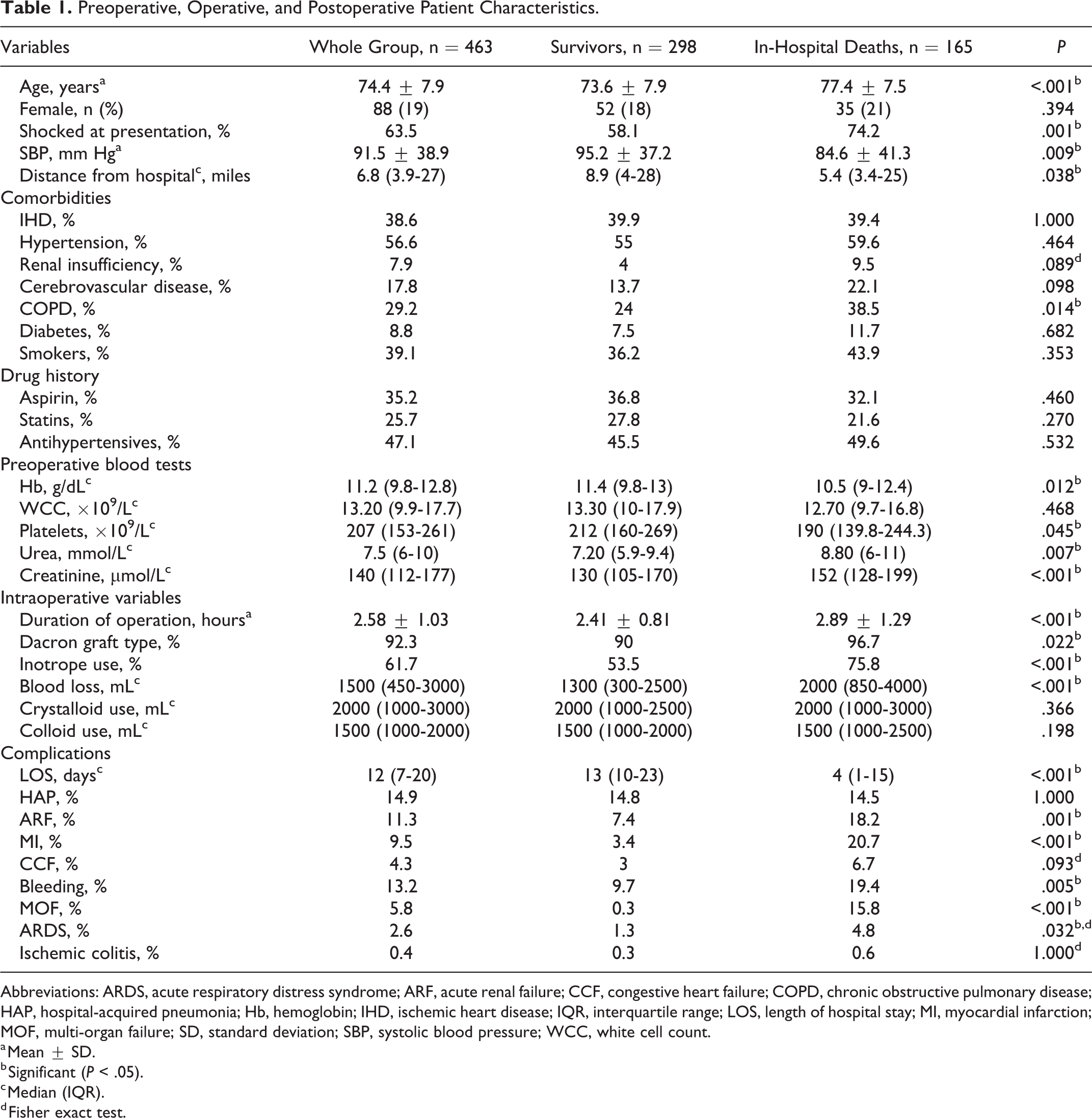
Abbreviations: ARDS, acute respiratory distress syndrome; ARF, acute renal failure; CCF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HAP, hospital-acquired pneumonia; Hb, hemoglobin; IHD, ischemic heart disease; IQR, interquartile range; LOS, length of hospital stay; MI, myocardial infarction; MOF, multi-organ failure; SD, standard deviation; SBP, systolic blood pressure; WCC, white cell count.
a Mean ± SD.
b Significant (P < .05).
c Median (IQR).
d Fisher exact test.
Effect of Gender on Preoperative, Intraoperative, and Postoperative Variables
Female patients were significantly older (78.7 ± 6.1 vs 74 ± 8.1 years; P < .001), lived closer to hospital (4.9 [3.3-18.7] vs 8.1 [4.1-27.7] miles; P = .030), had lower preoperative Hb level (10.4 [9.3-11.7] vs 11.6 [9.5-13] g/dL; P = .005), higher preoperative platelet count (230 [161-292] vs 200 [148.7-251.5] 109 L−1; P = .034), and received less crystalloids (1500 [1000-2000] vs 2000 [1000-3000] mL; P = .034) than male patients. The other variables (Table 1) showed no significant difference between genders.
In-Hospital Morbidity and Mortality
Hospital-acquired pneumonia (14.9%) was the most common postoperative complication followed by bleeding (13.2%) and ARF (11.3%; Table 1). Overall, a total of 394 (85%) patients survived the first 24 hours after the surgical operation. A univariable comparison between patients who survived and patients who died in hospital is presented in Table 1. Patients differed significantly in terms of age (P < .001), preoperative shock presentation (P = .001), preoperative systolic blood pressure (P = .009), distance from hospital (P = .038), percentage having COPD (P = .014), preoperative Hb level (P = .012), platelet count (P = .045), and serum urea (P = .007) and creatinine levels (P < .001). Intraoperatively, they differed in terms of duration of operation (P < .001), graft type (P = .022), inotropes used (P < .001), and the amount of blood loss (P < .001). Postoperatively, patients differed in terms of length of hospital stay (LOS, P < .001) and higher occurrence of MI (20.6%), ARF (18.2%), bleeding (19.4%) and multi-organ failure (MOF, 15.8%) in the in-hospital deaths group. The in-hospital mortality rate was 35.6%.
Predictors of In-Hospital Mortality
Variables with P < .05 in univariable analysis (19 variables) were entered into logistic regression model with in-hospital mortality as the dependent variable (Table 2). Predictors of in-hospital mortality included age (odds ratio [OR]: 1.21, 95% confidence interval [CI]: 1.08-1.34, P < .001), duration of operation (OR: 3.42, 95% CI: 1.41-8.25, P = .006), postoperative ARF (OR: 5.08, 95% CI: 1.09-23.69, P = .038), and LOS (OR: 0.91, 95% CI: 0.87-0.96, P < .001). The strongest predictors of in-hospital mortality were postoperative MI (OR: 15.11, 95% CI: 1.91-119.45, P = .010) and MOF (OR 138.37, 95% CI 2.53-7551.98, P = .016). Interestingly, an increase in distance from hospital by 1 mile decreased mortality by 0.91, 95% CI: 0.85-0.98.
Multivariable Analysis of Factors Affecting In-Hospital Mortality.
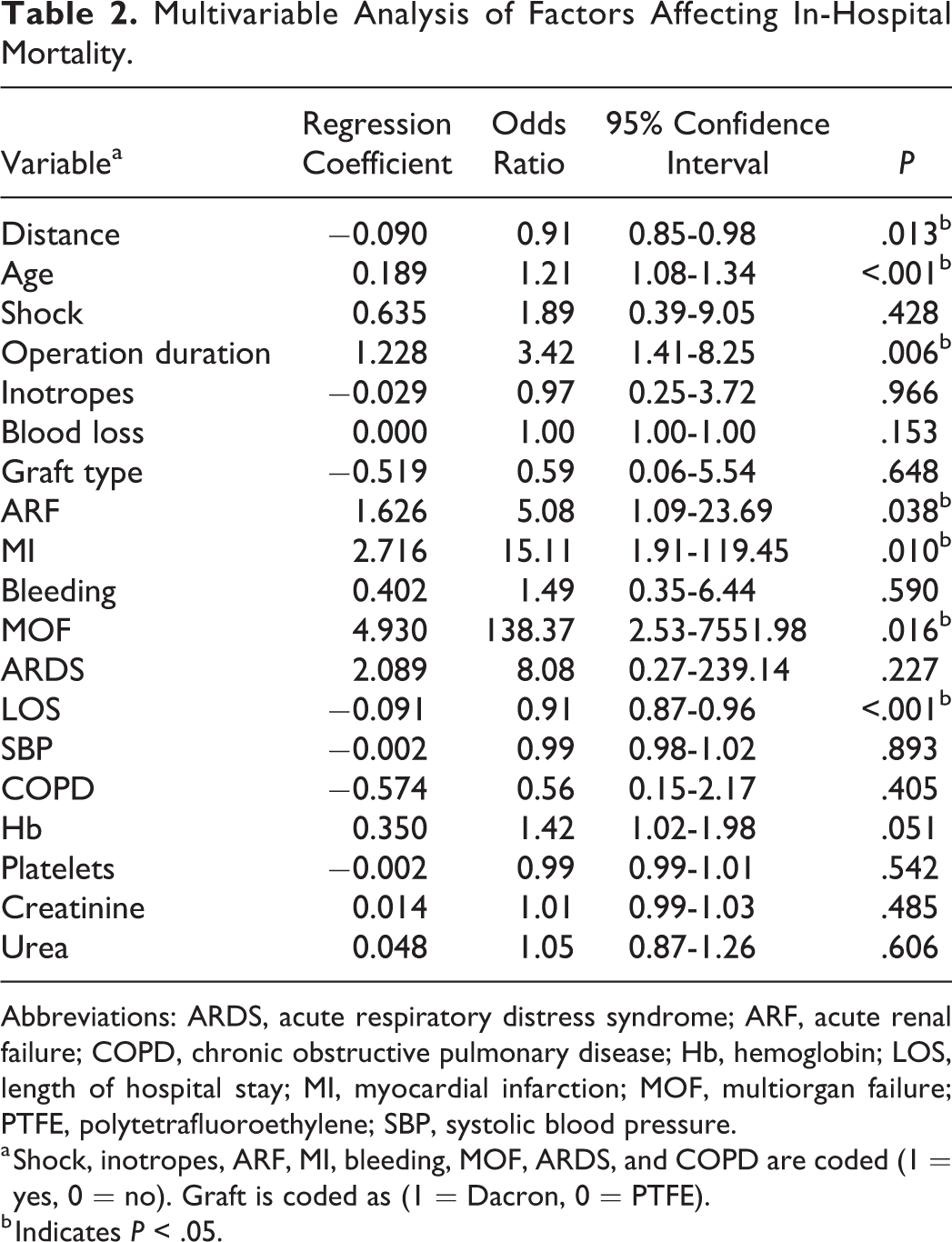
Abbreviations: ARDS, acute respiratory distress syndrome; ARF, acute renal failure; COPD, chronic obstructive pulmonary disease; Hb, hemoglobin; LOS, length of hospital stay; MI, myocardial infarction; MOF, multiorgan failure; PTFE, polytetrafluoroethylene; SBP, systolic blood pressure.
a Shock, inotropes, ARF, MI, bleeding, MOF, ARDS, and COPD are coded (1 = yes, 0 = no). Graft is coded as (1 = Dacron, 0 = PTFE).
b Indicates P < .05.
Long-Term Outcome
The 1-year mortality rate was 40%, and 5-year mortality rate was 48%. Median survival for the whole group was 5.08 years (Figure 1). Median survival for female patients was significantly lower than male patients (809 vs 2355 days, P = .024; Figure 2).
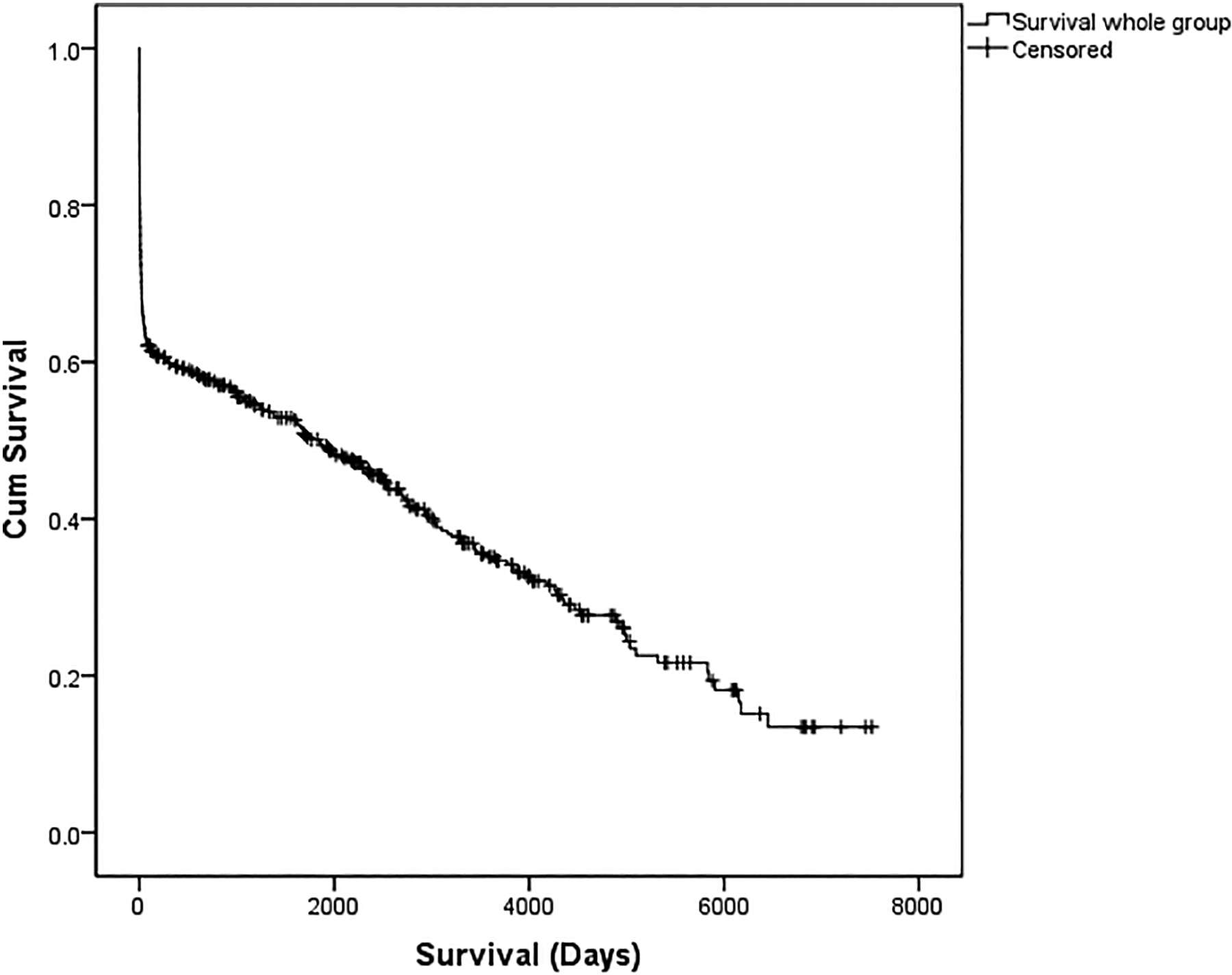
Median survival of the whole cohort.
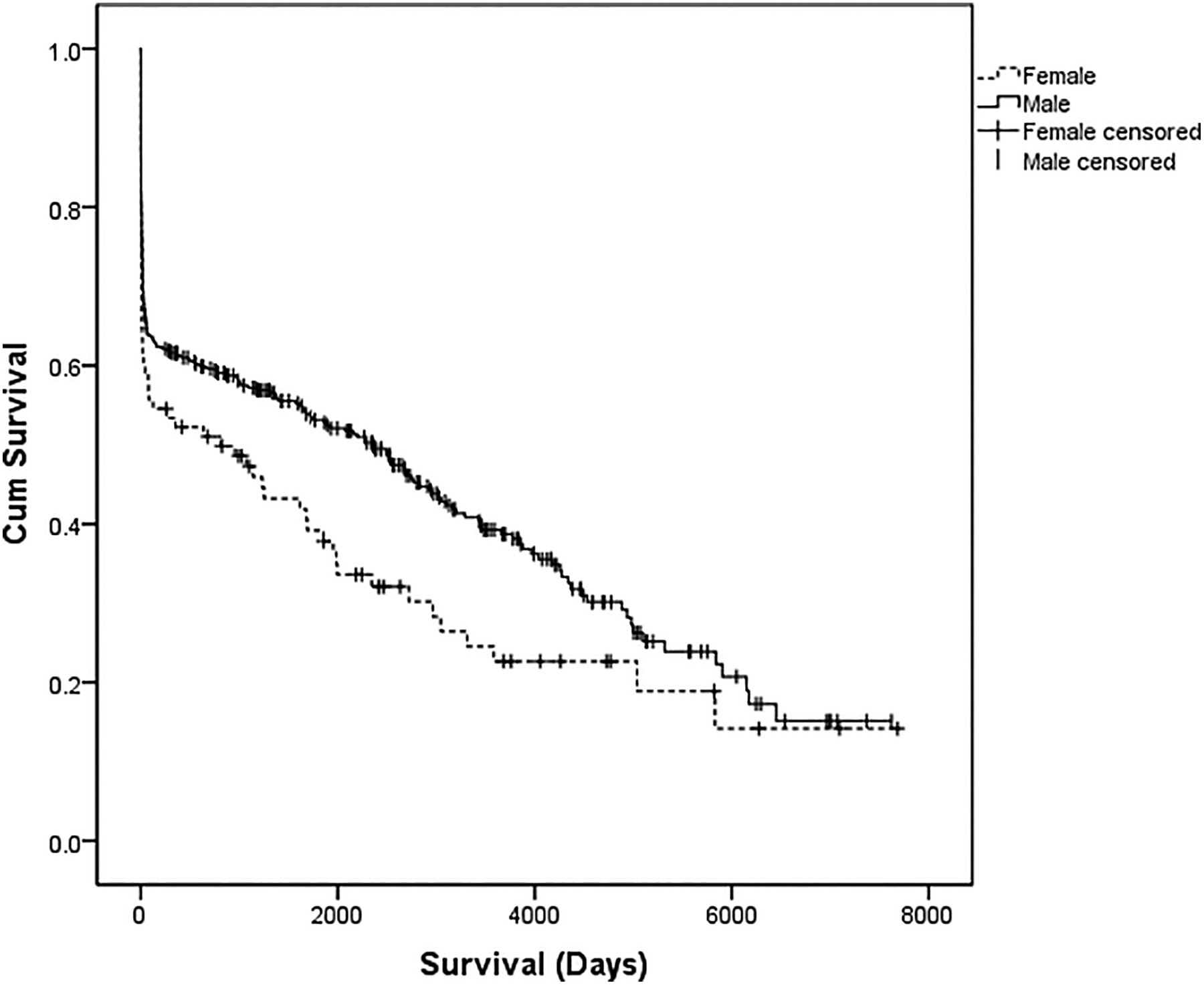
Median survival based on gender.
Predictors of Long-Term Outcome
Variables with P < .05 in univariable analysis were also entered in a Cox regression model to determine their effect on long-term survival. Although gender distribution was found to be insignificant in the univariable analysis, a significant difference in long-term survival was illustrated in the Kaplan-Meier survival analysis. Therefore, we included gender as a factor in the Cox regression model in addition to the same 19 variables that were entered into logistic regression model. Predictors of long-term outcome (Table 3) included age (hazard ratio [HR]: 1.11, 95% CI: 1.06-1.15), duration of operation (HR: 1.49, 95% CI: 1.11-2.01), and preoperative creatinine levels (HR: 1.00, 95% CI: 1.00-1.01). However, the strongest predictors of long-term outcome were postoperative MI (HR: 2.51, 95% CI: 1.05-5.96) and MOF (HR 9.05, 95% CI: 3.19-25.60). Interestingly, an increase in distance from hospital by 1 mile decreased the risk of death by a factor of 0.96, 95% CI: 0.94-0.98.
Multivariable Analysis of Factors Affecting Long-Term Outcome.
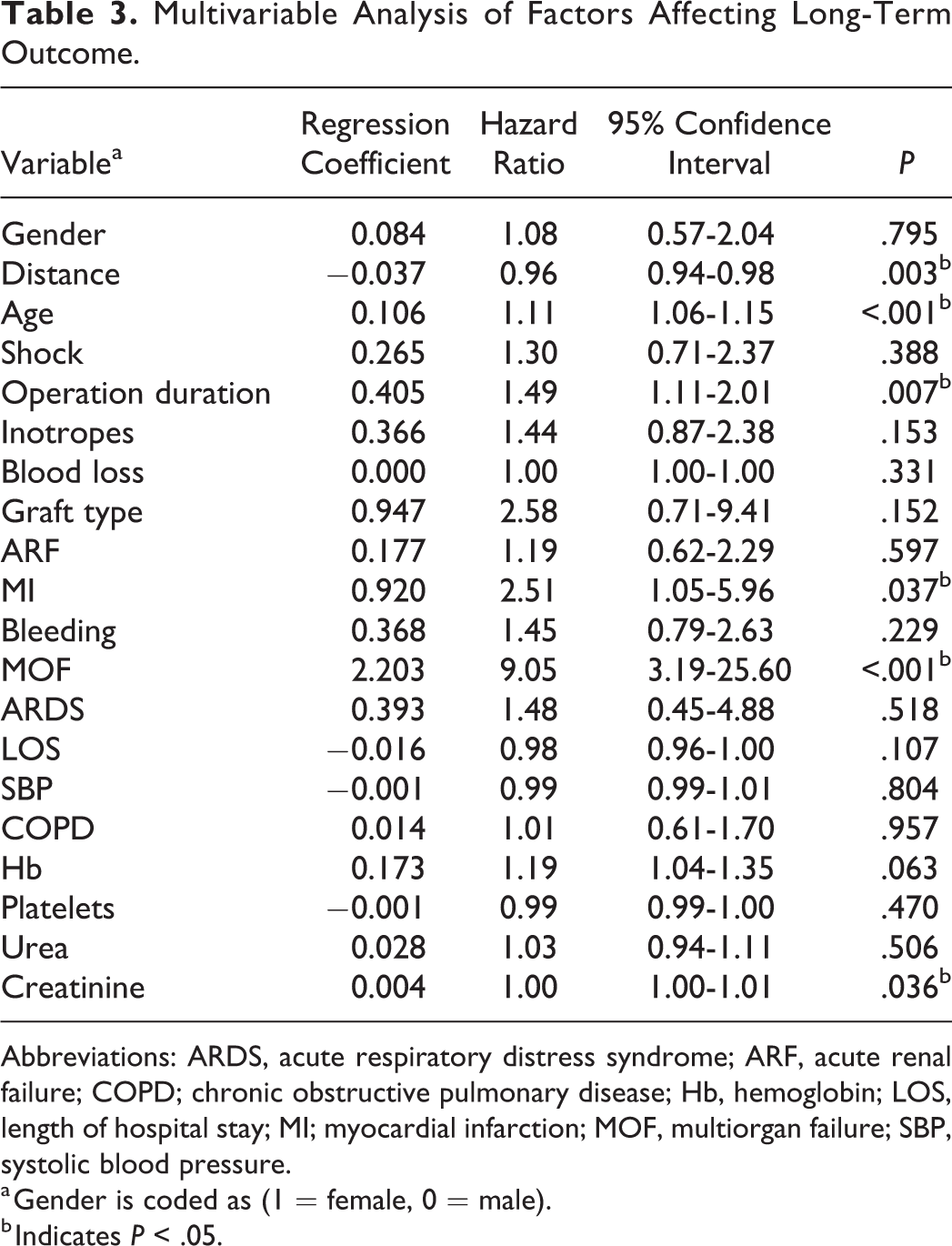
Abbreviations: ARDS, acute respiratory distress syndrome; ARF, acute renal failure; COPD; chronic obstructive pulmonary disease; Hb, hemoglobin; LOS, length of hospital stay; MI; myocardial infarction; MOF, multiorgan failure; SBP, systolic blood pressure.
a Gender is coded as (1 = female, 0 = male).
b Indicates P < .05.
Discussion
The present study is one of the largest cohorts to examine the effect of such a number of relevant variables on outcomes following open repair of RAAA. Several observational studies similarly explored the role of different preoperative, operative, and postoperative factors in defining a high-risk profile. 17 –20,21 –26 This presents clinicians involved in the care of these patients with valuable information.
We report an in-hospital mortality rate of 35.6%; this, in accordance with the more recently reported figures, is an improvement, since this intervention was first described in the 1950s. 10 However, the common agreement is that this procedure remains associated with a higher morbidity and mortality than acceptable.
The assessment of patient fitness for emergency interventions is usually made on an individual basis and starts at the first encounter in the emergency department. Our analysis identified advanced age as a predictor of inferior early and late outcomes. This is no surprise, as it agrees with most reports in literature. 13,14,17 –20,27 Hardman et al identified advanced age as 1 of 5 risk factors that can be used to assist in early risk stratification (age >76 years, loss of consciousness, ischemic features on electrocardiography, initial serum creatinine >0.19 mmol/L, and Hb <9 g%). 17 Age is now integral to most risk scoring systems prior to major vascular surgical interventions. 27,28 It should be clarified, however, that physiological age is actually the more relevant and that the general approach to the elderly patient with this surgical emergency should be carefully considered. More recent studies advocate a more confident surgical approach in the elderly individuals, as satisfactory early and late survival rates are observed in octogenarians surviving the initial insults of rupture and surgery. 21 –23 This is confirmed in the present study where octogenarian patients had a 45.3% in-hospital mortality rate. Hope remains that the now popular screening programs and advancing endovascular technologies will improve the overall outcomes in the elderly population further.
One of the objectives of this study was to report the main complications encountered during hospital stay and their effect on overall outcomes. In addition to advanced age, we identified 4 strong predictors of in-hospital mortality: operation duration, postoperative ARF, MI, and MOF. Hospital-acquired pneumonia was the most encountered postoperative complication during hospital stay. Review of this information adds to the clinical relevance of this study; these patients are known to spend an extended amount of time in hospital and especially in critical care units, and mortality increases in a cumulative fashion with each new systemic complication in the postoperative period, a common occurrence leading to MOF. Multi-organ failure is a diagnosis is associated with very poor prognosis 24 –26 and was the most common cause of delayed in-hospital deaths in the current series.
To date, the effect of operative duration on early mortality has not been highlighted in the literature. To our knowledge, this is the largest cohort to present this analysis showing that an increased operative time was independently associated with a higher in-hospital mortality rate. Wakefield et al similarly reported an increased postoperative mortality with operations exceeding 400 minutes in duration. 15 This relationship needs to be further investigated in relation to surgeon’s experience, aneurysm anatomy, preoperative hemodynamic status, and intraoperative factors such as fluid and blood product administration, clamp site, and graft description among other variables that can increase operative time and complexity.
Survival beyond hospital discharge for patients undergoing open repair of RAAA is generally good, 29 –31 and functional outcomes seem to be comparable to outcomes following elective repair. 32 In the current study, we found that advanced age was also independently associated with adverse long-term survival. However, MI and MOF in the postoperative period were more powerful predictors.
The comparison in survival patterns presented here show that in the long term, female survival is inferior to that of males. This difference may be partially explained by the fact that females were significantly older in our population (by about 4 years); however, in the literature, controversy exists regarding the role of female gender and its association with inferior outcomes. Evans and colleagues, 33 in contrast with others, 34,35 examined data from the Lothian surgical audit to show that there was no significant differences in perioperative mortality nor long-term survival between both genders in patients who underwent surgical AAA repair. Interestingly, it was difficult to explain the noted gender selection bias for intervention; a greater proportion of women were deemed more at risk and so denied open repair. This is unlikely to be solely attributed to age. But a review of administrative data failed to show a significant difference in preoperative comorbidities between the 2 genders which would offer an alternative explanation. 33 Mureebe et al, on the other hand, examined data from the Medicare database to show that females had higher early mortality rates and were less likely to leave hospitals following interventions for RAAA. 36 They also noted the difference in the proportion of females undergoing an intervention for RAAA. This is still poorly understood. The apparent discrepancy in management between genders raises some queries on the timing of intervention and the value of screening in women. Further research is needed to highlight this important matter.
Intriguingly, our analysis showed that a decrease in mortality is associated with increased distances traveled to hospital. Adam et al were the first to describe the regional management of RAAA with focus on the distance traveled, surgical intervention rates, and outcomes in the United Kingdom. 37 Using data from the Lothian surgical audit, they found no significant difference in distance travelled between survivors and non-survivors. Research later followed to further reinforce these findings. 16,38,39 A possible explanation for the aforementioned outcome in our study could be related to the fact that those deemed clinically suitable for transport across to Hull Royal Infirmary might have actually been in a better clinical condition to withstand open repair. Since no information is available on community deaths prior to transfers, it is difficult to verify this conclusion.
The outcome data for open repair of RAAA in the current study are acceptable given that the only reasons for nonoperative management were patient refusal, cardiac arrest, and known end-stage disease (eg, advanced dementia or metastatic carcinoma). For 15 years, the unit’s policy has been to use minimal fluid resuscitation (permissive hypotension), cell saver when possible, and consultants to be scrubbed always and as quick an operation as is feasible. Whether EVAR can equal or better these data in all patients with RAAA is yet to be proved.
Predicting mortality and outcomes following open repair of RAAA is a complex process. This procedure is still associated with high morbidity and mortality despite advances in anesthesia and service centralization. A variety of patient, surgeon, and hospital factors play a role, and widespread screening programs together with increasing elective repairs might show further improvements in the years to come. It must be appreciated that the key to reducing AAA mortality is early diagnosis with screening and elective intervention. 40 –42
This study has some limitations. This was a retrospective study of prospectively collected data of a nonrandomized design. Retrospective studies lack exposure control or the reporting on some variables and introduce selection and misclassification bias. However, the data in our study were collected in a prospective robust manner that reduces selection and information bias.
To conclude, in patients with RAAA undergoing open surgical repair, the strongest predictors of in-hospital mortality and long-term outcome were postoperative MOF and MI and operative duration and to a lesser degree advanced age and ARF.
Footnotes
Acknowledgments
The authors thank Mrs Barbara McCloy for performing the search using the vascular database and for helping us in retrieving case notes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.