
Abstract
Although coronary revascularization procedures are widely performed in patients with coronary artery disease (CAD), angina is often reported, even after such procedures. This study evaluated the antianginal efficacy and effect of ivabradine treatment on quality of life (QOL) in patients with CAD and history of coronary revascularization. This is a post hoc analysis (926 post-revascularization patients) of a prospective, noninterventional study, which included 2403 patients with CAD and stable angina. The data were recorded at baseline, at 1 month and 4 months after inclusion. After ivabradine administration, mean number of anginal events decreased from 2.2 ± 2.3 (median: 2.0, minimum: 0.0, maximum: 21.0, range: 21.0) to 0.3 ± 0.6 (median: 0.0, minimum: 0.0, maximum: 7.0, range: 7.0) times/week (P < .001), while nitroglycerin consumption decreased from 1.5 ± 2.2 (median: 1.0, minimum: 0.0, maximum: 20.0, range: 20.0) to 0.1 ± 0.4 times/week (median: 0.0, minimum: 0.0, maximum: 5.0, range: 5.0; P < .001). Quality of life improved at study completion compared to baseline (P < .001). Ivabradine addition on top of optimal individualized dose of β-blockers is associated with decreased anginal events and improvement in QOL in patients with stable angina and history of coronary revascularization.
Introduction
Angina pectoris is the most common disabling symptom in patients with coronary artery disease (CAD). Despite the wide use and improvement in revascularization procedures and techniques, a substantial percentage of patients remain symptomatic or will present angina pectoris in the future. 1 Data from a national chart review which assessed approximately 2000 patients with chronic angina revealed that from the patients who underwent revascularization in the prior year (57% of the total sample, 28% underwent coronary artery bypass surgery [CABG], and 39% percutaneous coronary intervention [PCI]), 92% presented at least 1 anginal event 6 months after the procedure, while 34% presented at least 1 episode per week. 2 In this population, angina is mainly attributed to disease progression, and hence pharmacological treatment represents the main clinical strategy for controlling ischemia and anginal symptoms. 3
Ivabradine is a heart rate (HR) lowering agent indicated in patients with chronic stable angina, 3 as well as in patients with chronic heart failure. 4 Several studies have demonstrated that the addition of ivabradine in patients with chronic stable angina significantly decreased the number of anginal events, nitroglycerin consumption, and time to angina onset, while improving angina, as well as quality of life (QOL), since a level of satisfactory usual activity was restored. 5 –8
Objectives
Our aim in this study was to evaluate the antianginal efficacy of ivabradine coadministered as individualized treatment with a β-blocker, during 4 months of treatment, in patients with CAD and history of coronary revascularization (CABG or PCI), as well as to evaluate the effect of this treatment on their QOL. The study objectives were to record the effect of ivabradine on resting HR, anginal events and nitroglycerin consumption, as well as on angina classification (on the basis of the Canadian Cardiology Society) 9 and on QOL, 1 and 4 months after the administration.
Study Design
Patients and Methods
This study was designed in line with the recommendations of the updated Helsinki declaration, Good Pharmacoepidemiology Practice Guidelines, and rules of Good Clinical Practice and was approved by the appropriate ethics committees (Scientific Councils) of participating hospital departments. Copyright permission to use the Euro quality 5 dimensions (EQ-5D) QOL questionnaire 10 was received. All patients were informed and gave their consent to participate, prior to their inclusion in the study.
Patients
Inclusion criteria were male or female ambulatory patients >18 years old, diagnosed with CAD and stable angina, with resting HR >60 bpm, despite treatment with β-blockers at the optimal individualized dose, and a need for coadministration of ivabradine. The optimal individualized dose was assessed by the treating physician. The decision for administrating ivabradine was made regardless of the patient’s perspective to be included in the study, and ivabradine treatment was started at maximum 5 days before the inclusion in the study. Treating physician was responsible for the dosage of ivabradine, taking into consideration the summary of product characteristics and HR.
Exclusion criteria were patients who had been hospitalized for cardiovascular disease during the last 3 months (including revascularization) or had a scheduled revascularization. In addition, patients with other conditions such as serious end-stage diseases (cancer, serious liver, respiratory and heart or renal insufficiency), severe neuropsychiatric diseases and cerebrovascular events with serious residual lesions and cases of pregnancy, lactation, or willingness to become pregnant were excluded.
This is a post hoc analysis, describing patients with history of coronary revascularization (CABG or PCI). The primary study was a multicenter, prospective, noninterventional study of 2403 patients with CAD and stable angina, which assessed data from 245 private cardiology offices and was coordinated by 2 cardiology departments of Greek hospitals. 11 This sample of patients included 926 patients who had previously undergone coronary revascularization. The total forecasted duration of follow-up observation for the needs of the study was 4 months, while the evaluations were performed at 3 intervals: at inclusion and at 1 and 4 months after inclusion. Quality of life was assessed by means of the EQ-5D questionnaire (EQ-5D index and visual analogue scale [VAS]; recorded at baseline and study completion). The EQ-5D questionnaire includes 5 dimensions: mobility, autonomy in self-care, usual activities, pain/discomfort, and stress/distress stratified in 3 levels, leading to 243 health conditions in total, and each health condition is stratified according to individual preference among several health conditions. 10 –14
Patient adherence to treatment with ivabradine was evaluated using a 5-level scale (recorded at the second and third visit): The patient had taken the treatment daily, during the interval from previous visit. The patient had taken the treatment very often (the patient might have forgotten it once or twice, during the interval from previous visit). The patient had taken the treatment half of the days, during the interval from previous visit. The patient had not taken the treatment for most of the days, during the interval from previous visit. The patient had never taken the treatment, during the interval from previous visit.
The tolerability of the treatment was evaluated by recording the time and reason for study treatment discontinuation. Patients’ visit schedule, study assessments, and patients recorded on each study visit are shown in Table 1.
Study Design: Visit Schedule, Study Assessments, and Patients Recorded During Each Visit.
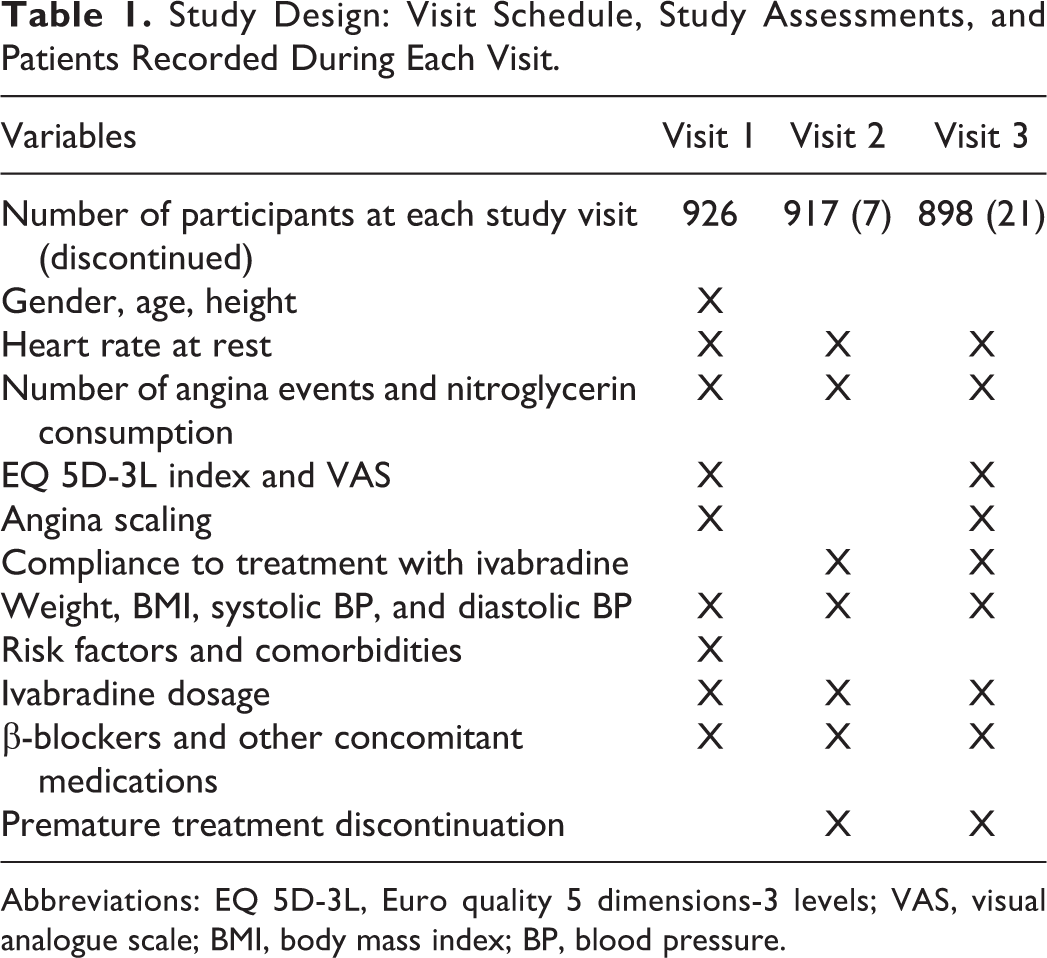
Abbreviations: EQ 5D-3L, Euro quality 5 dimensions-3 levels; VAS, visual analogue scale; BMI, body mass index; BP, blood pressure.
β-Blocker Dosage
During the study, β-blockers were prescribed at a dose considered by the treating physician to be optimal for each patient. The target dose of the most common β-blockers was defined as atenolol 100 mg/d, betaxolol 10 mg/d, bisoprolol 10 mg/d, carvedilol 100 mg/d, celiprolol 200 mg/d, metoprolol 200 mg/d, nebivolol 10 mg/d, propranolol 160 mg/d, and sotalol 160 mg/d.
Statistical Analysis
For the main parameters (HR at rest, number of angina events, nitroglycerin consumption, and EQ 5D and VAS questionnaire), a 97.5% confidence interval (CI) was given for the differences between the first and the third visit. The change in efficacy parameters over time was investigated using the Friedman test and the Wilcoxon test (for pairwise comparisons between visits). Multiple linear regression technique tested the relation of the differences in the main parameter between the first and the third visit with the following parameters: gender, age, angina scaling on the first visit, HR on the first visit, calcium channel blockers (CCBs; yes–no), long-acting nitrates administration (yes–no) for the total trial duration, and acute myocardial infarction (yes–no). The same technique was also applied in the case of QOL VAS to test the relation of VAS differences between the first and the third visit with the following parameters: VAS on the first visit, gender, age, angina scaling on the first visit, anginal events difference between the first and the third visit, nitroglycerin consumption difference between the first and the third visit, HR difference between the first and the third visit, CCBs (yes–no), long-acting nitrates administration (yes–no) for the total trial duration, and acute myocardial infarction (yes–no). Spearman correlation coefficients were computed for each pair of differences between the first and the third visit: HR at rest, number of angina events, and nitroglycerin consumption. Spearman correlation coefficients were computed between angina scaling differences and the following differences between the first and the third visit: HR at rest, number of angina events, and nitroglycerin consumption.
Results
Of the 926 patients with CAD with a history of coronary revascularization (CABG or PCI) who participated in the study, 28 (3%) prematurely discontinued treatment with ivabradine. Approximately 77% of the patients were male. Patients mean age was 66.9±10.5 years and mean body mass index was 28.4±4.0 kg/m2. The most frequent comorbidities were hypercholesterolemia (78.6%) and hypertension (71.9%). Patient baseline characteristics are shown in Table 2. All patients were receiving β-blockers at inclusion at the optimal individualized dose (Table 3), while 70 patients discontinued them during the trial due to intolerance (30 patients), hypotension (6 patients), or other reasons (38 patients).
Baseline Characteristics of Patients (n = 926).
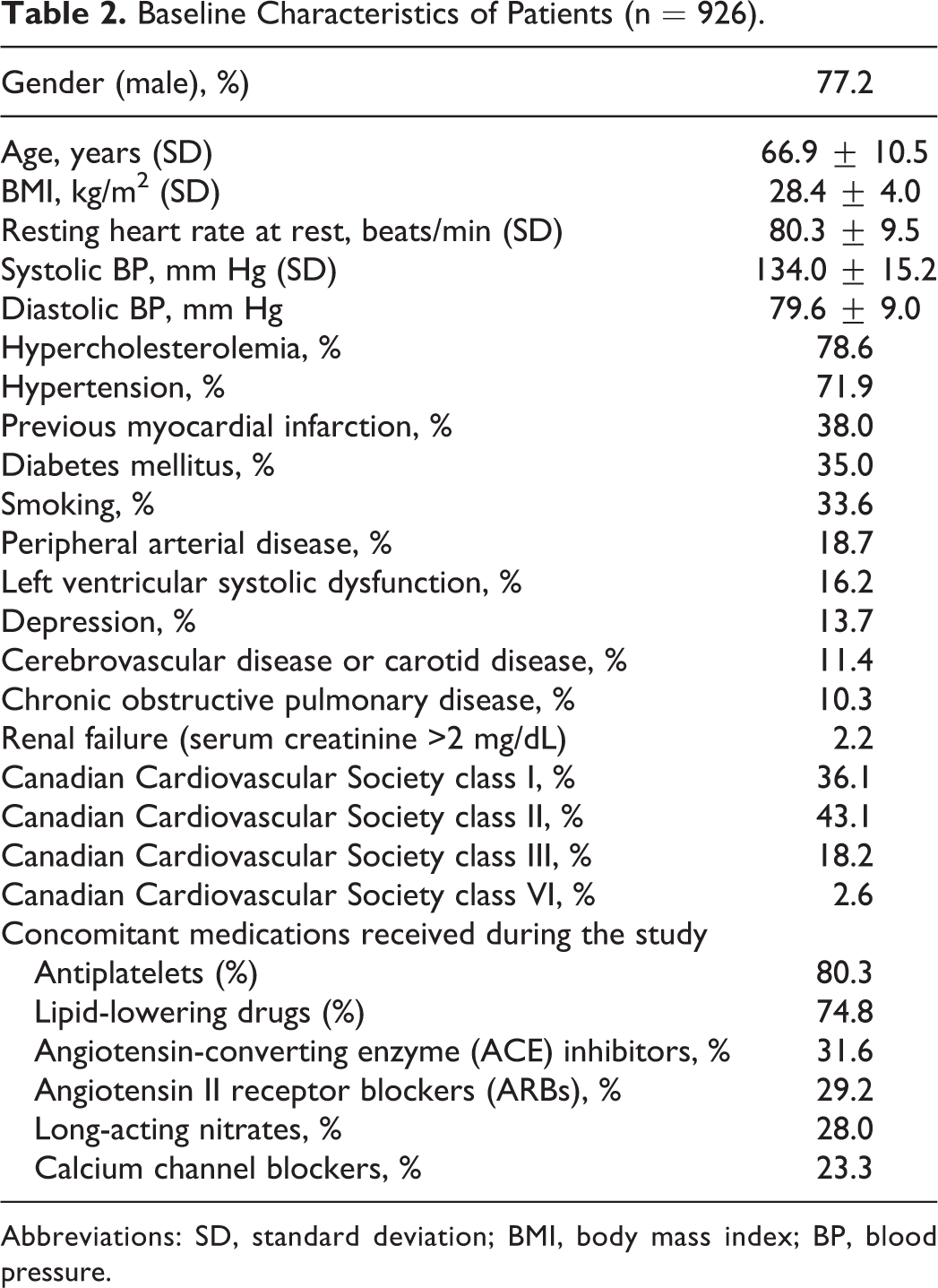
Abbreviations: SD, standard deviation; BMI, body mass index; BP, blood pressure.
Total daily dose (mg) of the b-blockers and ivabradine received on each study visit.
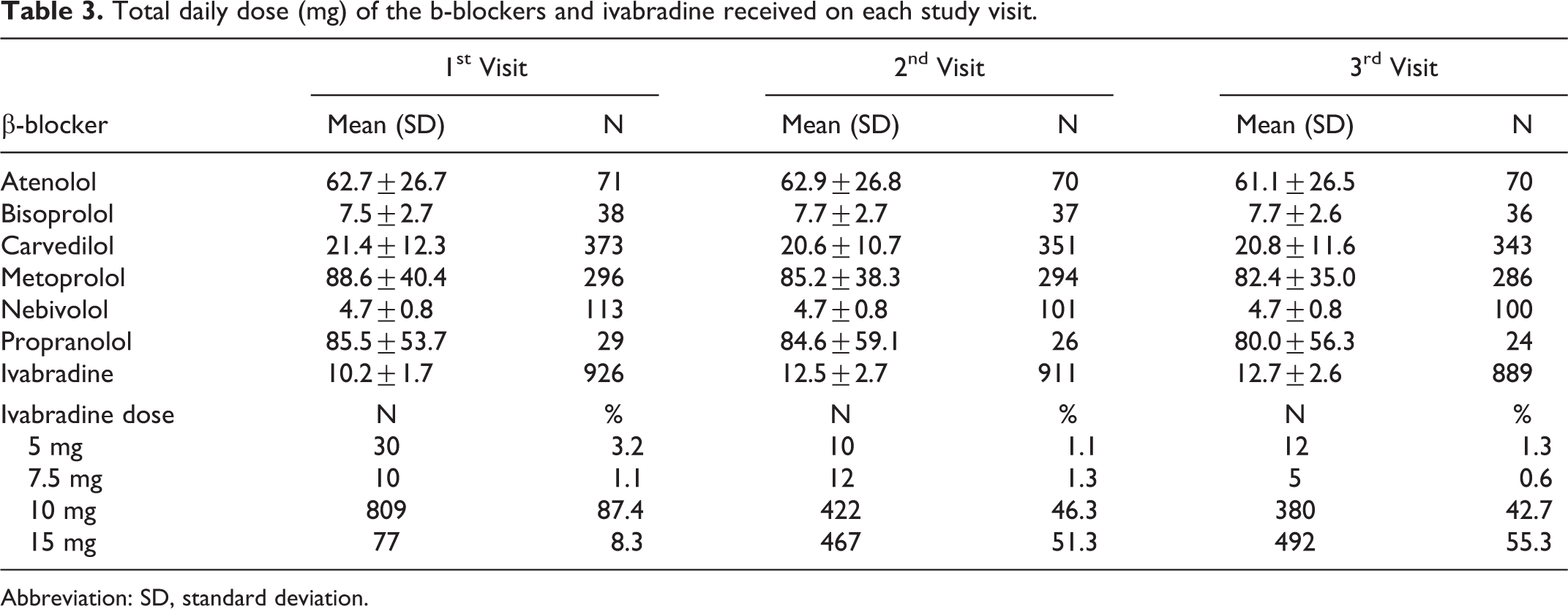
Abbreviation: SD, standard deviation.
In addition to ivabradine and β-blockers, 31.6% also received angiotensin-converting enzyme (ACE) inhibitors, 29.2% received angiotensin II receptor blockers (ARBs), 23.3% received CCBs (0.6% received nondihydropyridine CCBs), 28% received long-acting nitrates, 23.5% received diuretics, 80.6% received anticoagulants (antiplatelets 80.3%) and 74.8% received lipid-lowering drugs.
At baseline, 85.2% of the patients had a resting HR ≥70 bpm, despite treatment with β-blockers. Ivabradine decreased mean resting HR from 80.3 ± 9.5 bpm at the first visit to 67.8 ± 7.3 bpm at the second visit and 63.9 ± 6.2 bpm at the third (P < .001). The magnitude of HR decrease was related to baseline HR. Patients with higher HR at baseline (>80 bpm) showed greater HR decrease (average decrease −22.6 bpm) than patients with HR 70-80 bpm (average decrease −14.0 bpm) as well as from those with HR <70 bmp (average decrease −7.5 bpm; P < .001; Figure 1). The percentage of patients with HR >80 bpm decreased from 40.3% at the first visit to 3.4% at the second visit, while it was further decreased to 1.0% at the third visit. In contrast, the percentage of patients with HR <70 bpm increased from 14.8% at the first visit to 71.9% at the second visit, while it was further increased to 88.9% at the third visit (P < .001). Mean HR decrease was not related to β-blocker dosage when patients who received ≥50% or <50% of target β-blockers dose were compared for the total trial duration (P = not significant [ns]).
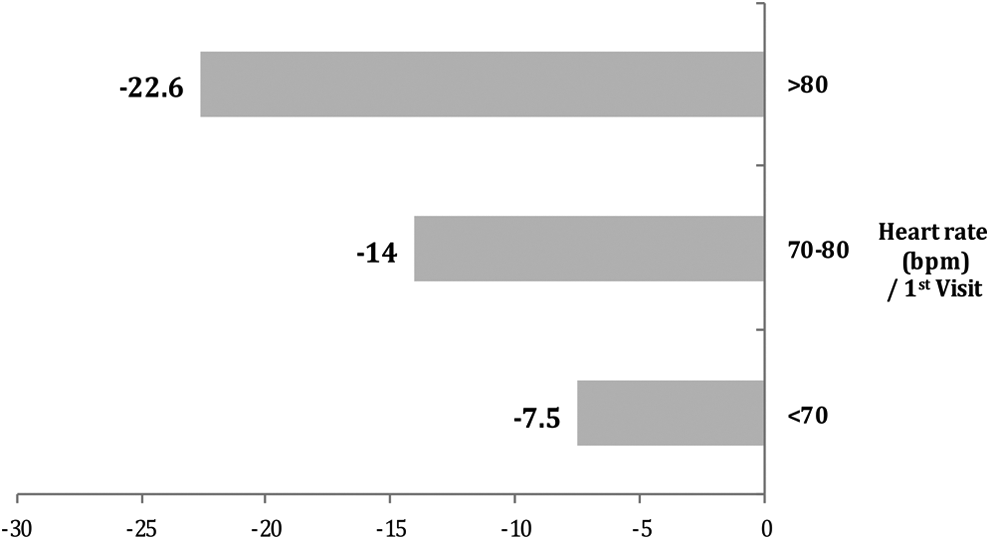
Heart rate at rest/difference between the first and the third visit of the study (N = 884).
At baseline, 17.2% of the patients had no angina events at the week before inclusion. The mean number of angina events decreased from 2.2 ± 2.3 (median: 2.0, minimum: 0.0, maximum: 21.0, range: 21.0) times/week at the first visit to 0.5 ± 1.0 (median: 0.0, minimum: 0.0, maximum: 10.0, range: 10.0) at the second visit, and 0.3 ± 0.6 (median: 0.0, minimum: 0.0, maximum: 7.0, range: 7.0) times/week at the third visit (P < .001; Figure 2). The percentage of patients with no angina events during the week prior to the study visits increased from 17.2% at the first visit, to 67.3% at the second visit, while it was further increased to 81.6% at the third visit (P < .001; Figure 3).
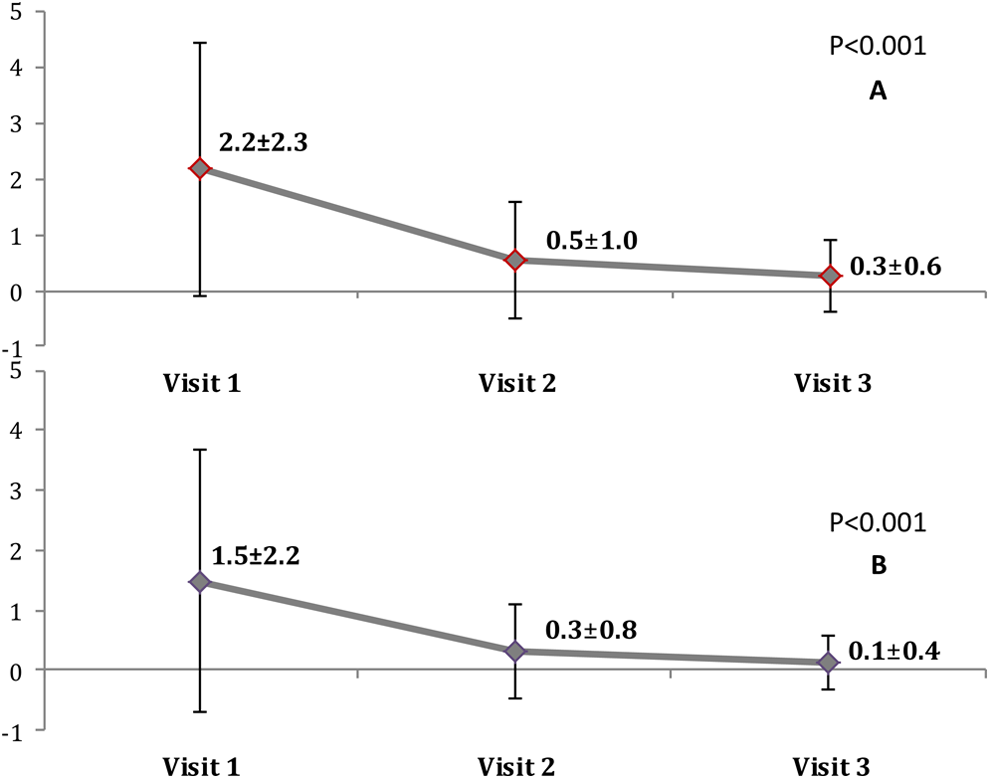
Number of angina events (A) and nitroglycerin consumption (B) /mean ± SD at the 3 visits of the study (N = 884).
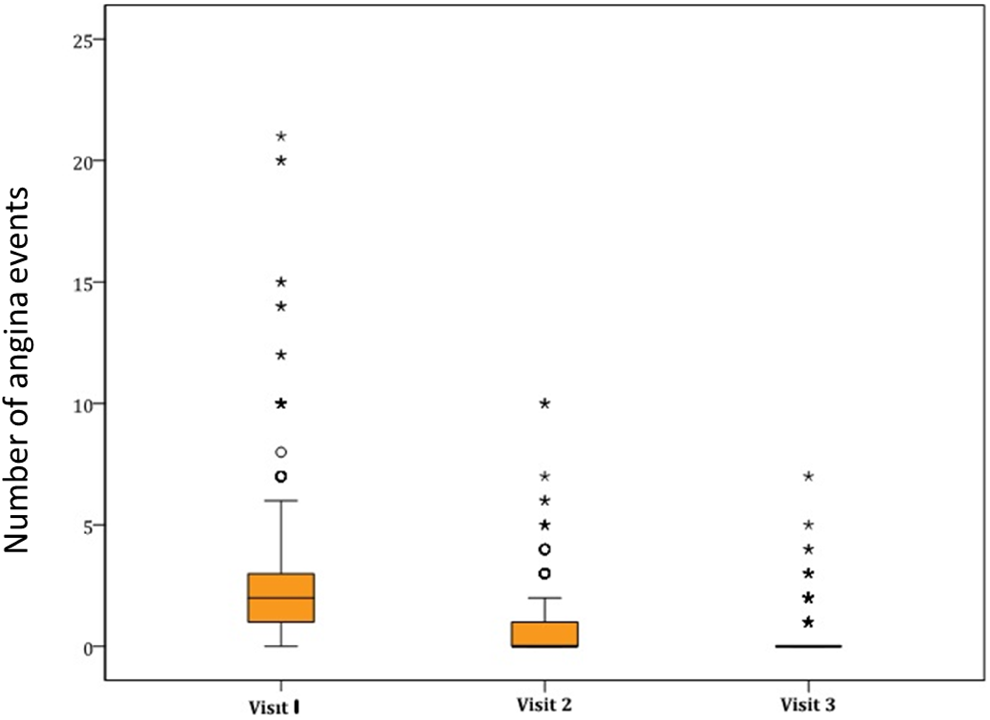
Box-Whisker graph/number of anginal events on the 3 visits of the study (N = 884).
Nitroglycerin consumption decreased from 1.5 ± 2.2 (median: 1.0, minimum: 0.0, maximum: 20.0, range: 20.0) times/week at the first visit to 0.3 ± 0.8 (median: 0.0, minimum: 0.0, maximum: 10.0, range: 10.0) at the second visit, and 0.1 ± 0.4 (median: 0.0, minimum: 0.0, maximum: 5.0, range: 5.0) times/week at the third visit (Figure 2; P < .001).
The reduction of angina events and nitroglycerin consumption were both positively correlated with the reduction of HR (P = .046 and P = .006, respectively).
The percentage of patients with angina CCS classification III or IV decreased from 20.8% at the first visit to 2.2% at the third, while the percentage of patients with angina CCS classification I increased from 36.1% at the first visit to 83.1% at the third (P < .001; Figure 4).
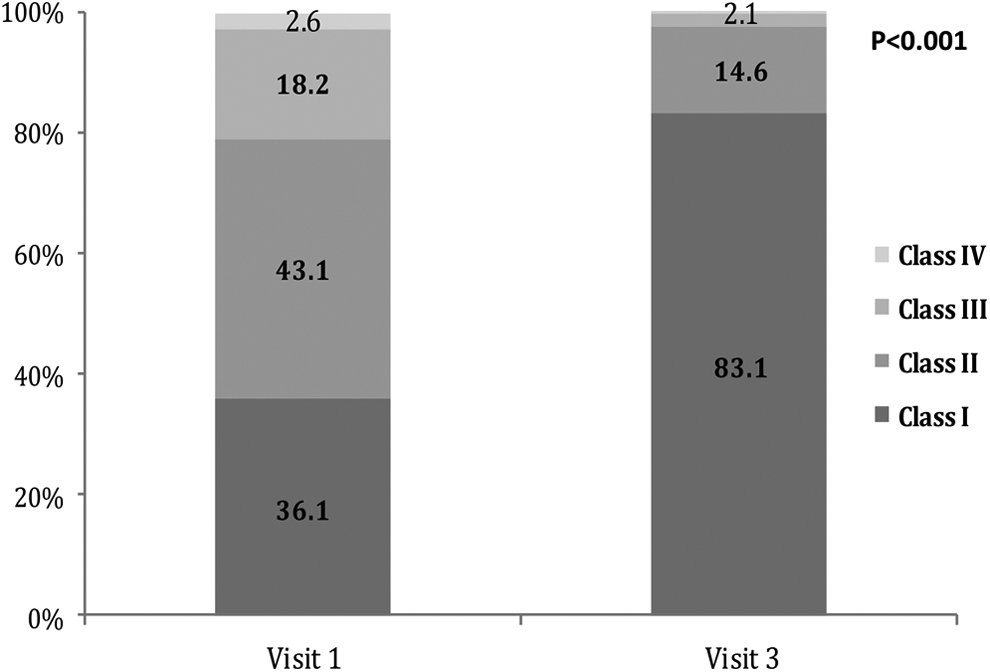
Angina classification according to the Canadian Cardiovascular Society (% of patients) at visits 1 and 3 (N = 884).
For the total trial duration, 206 patients (22.2% of the total sample) received CCBs (6 [0.6%] patients received nondihydropyridine CCB) and 248 (26.8%) patients received long-acting nitrates. Patients who received CCBs and long-acting nitrates were predominantly older (P < .001).
For all dimensions of the EQ-5D questionnaire, the percentage of patients who answered “no problem”/“not at all” increased substantially at study completion compared with baseline (P < .001). Ivabradine administration increased the percentage of patients with no “mobility problem” by 26.1% (231 more patients), the “autonomous in self-care” by 11.4% (101 patients), those with “no problem in usual activities” by 27.1% (240 patients), the percentage of patients with no pain/discomfort by 54.1% (478 more patients) and the percentage of patients with no stress/distress by 20.2% (179 patients; Table 4; P < .001). The mean EQ-5D index increased at study completion by 0.2 points compared to baseline (from 0.6 ± 0.3 to 0.8 ± 0.2; P < .001), while VAS increased by 15.5 points (from 62.6 ± 16.4 to 78.1 ± 17.3; P < .001). The EQ-5D VAS was significantly correlated with HR; patients with higher HR decrease showed greater increase in the VAS (P < .001). Improvement in QOL was not associated with the dose of β-blockers (P = ns, between the 2 groups <50% and ≥50% of the β-blocker target dose). Reduction in angina events, nitroglycerin consumption, and angina scaling and increase in EQ-5D VAS scale on the third visit compared with baseline in patients with HR > 70 bpm or <70 bpm are shown in Figure 5.
The Distribution of the 5 Dimensions of the EQ-5D Questionnaire at Visits 1 and 3 (N = 884).
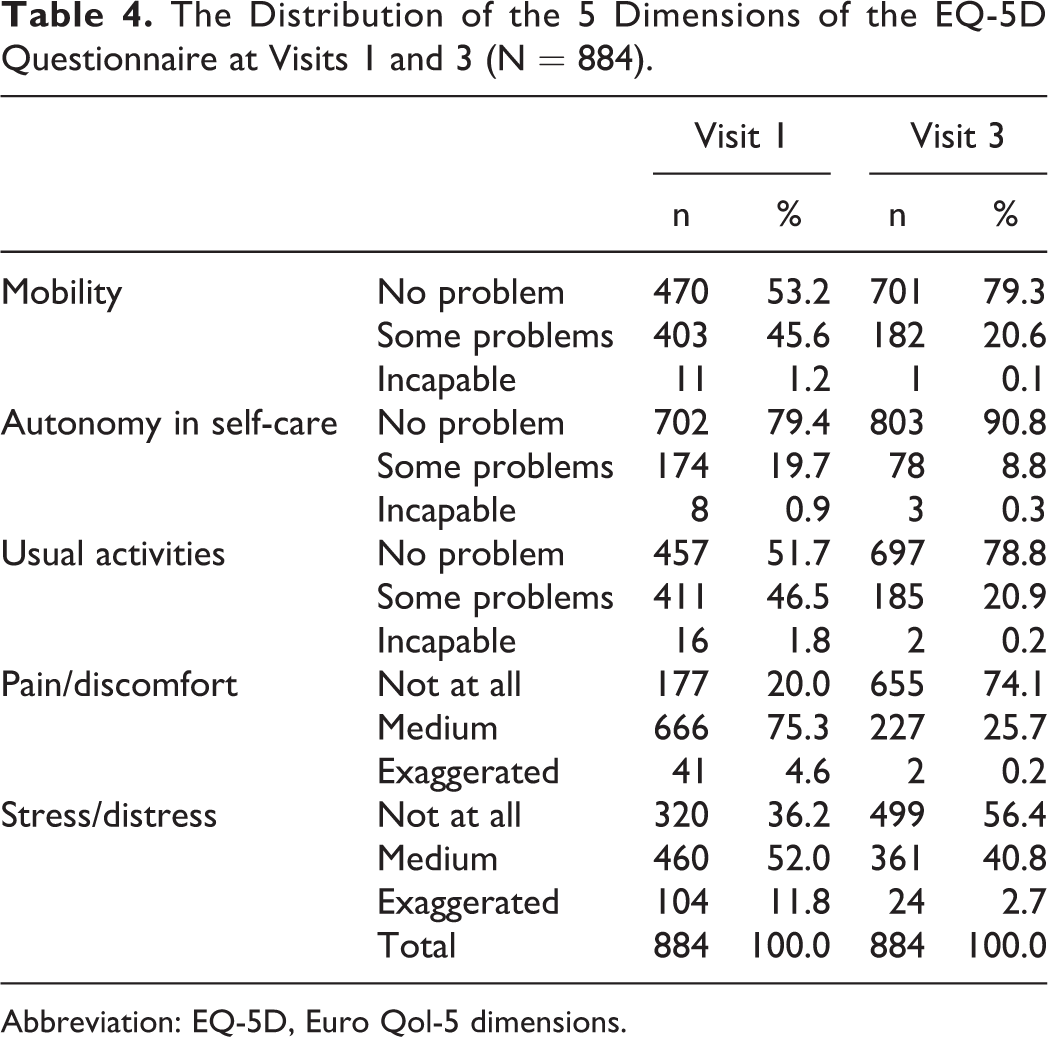
Abbreviation: EQ-5D, Euro Qol-5 dimensions.
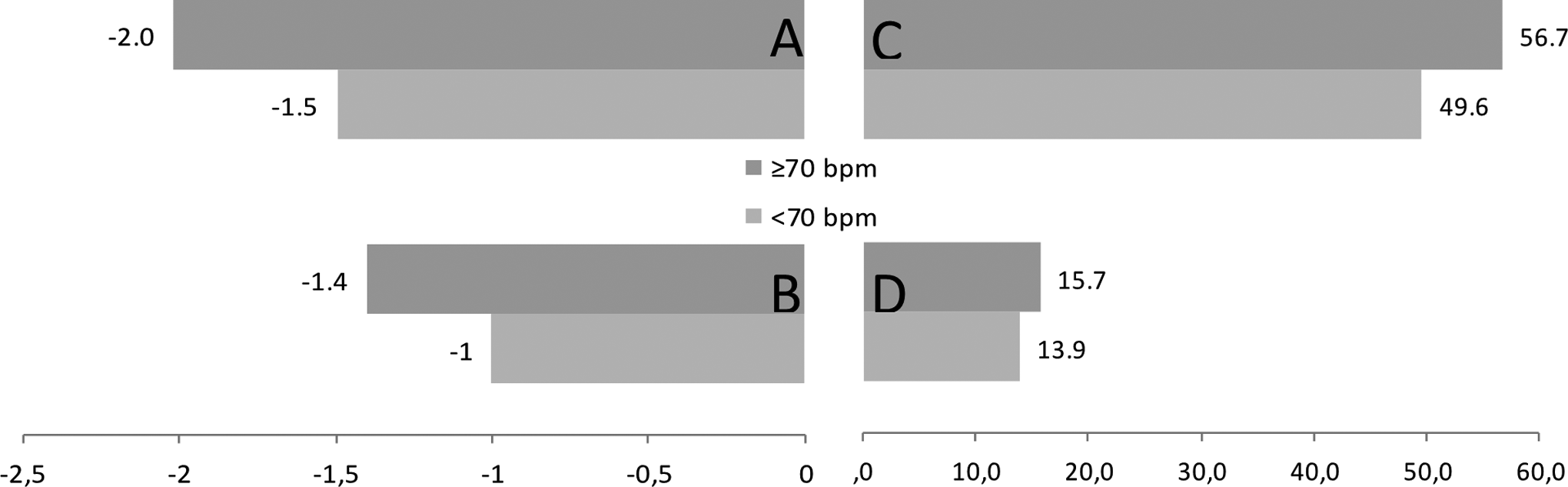
Reduction in angina events (A), nitroglycerin consumption (B) angina scaling (C), and increase in EQ-5D VAS scale (D) on the third visit compared to baseline (N = 884).
Adherence to treatment with ivabradine was high; throughout the study, 884 (95.5%) patients were taking their treatment “everyday” or “quite often.” A constant ivabradine dosage was administrated throughout the study to 408 patients (44.1% of the total sample). In 335 of those patients, ivabradine was administrated at 5 mg twice daily. At the second visit, 467 patients (51.3% of the total sample) were receiving ivabradine 7.5mg twice daily and maintained this dosage during the whole study.
Safety Assessment
Seventeen patients presented adverse reactions and/or adverse events during the study and discontinued. The most common adverse events leading to treatment discontinuation were 2 cases of bradycardia, 3 cases of atrial fibrillation and 2 cases of blurred vision.
Discussion
Coronary revascularization as expressed by PCI or CABG is performed worldwide as treatment of flow-limited coronary stenosis, in order to reduce ischemia and its manifestations. 15 Unfortunately, a significant percentage of these patients remain symptomatic or will present with angina in the future. 2 Data from the Project of Ex-vivo graft Engineering via Transfection IV study (PREVENT IV) revealed a significant proportion of failure of one or more venous grafts (45%) after 12 to 18 months from CABG, 16 while another study suggests that almost 9% of those patients will present with recurrent angina in 16 months. 17 Recurrence of symptoms is also observed after PCI, while the presence of angina 6 months after the procedure is mainly attributed to coronary disease progression, other than in the target vessel. 18 In addition, several studies and systematic reviews 19 –21 which compared PCI with medical treatment failed to show a difference in terms of mortality and risk of myocardial infraction (MI). Thus, according to the guidelines, 3,22 optimal medical treatment in those patients is imperative in order to reduce morbidity and mortality independent of the decision of possible reattempt for revascularization.
In the present study, 85.2% of the patients had HR ≥70 bpm, despite treatment with β-blockers. Although the percentage of patients with increased HR is high, this phenomenon has also been observed in several other studies and registries, 5,7,8,23 despite β-blocker treatment. In this study, increased HR may be attributed to the fact that only 43.6% of the patients were receiving β-blocker dosage ≥50% of the target dose. However, this has also been observed in several other studies and surveys with post-myocardial infarction or stable angina patients. 5,24,25 Uptitration of a β-blocker to target dosage usually presents difficulties because of poor tolerance and adverse effects such as dizziness, fatigue, and hypotension 26 or because of physicians’ reservations in case of existing comorbidities. 24
Adding ivabradine to the treatment plan led to a decrease (−16.4 bpm) in resting HR. Interestingly, in our study, patients receiving higher doses of β-blockers (≥50% of target dosage) did not present a statistical significant difference in HR with respect to patients having lower β-blocker dosage (<50% of target dose). However, this phenomenon was also observed in several other studies (Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure [MERIT-HF] 27 and Cardiac Insufficiency Bisoprolol Study II [CIBIS II]), 28 where achieved HR or HR reduction was similar in patients receiving metoprolol or bisoprolol, respectively, regardless of the dose administrated.
The addition of ivabradine led to a reduction in angina events and nitroglycerin consumption, while improved CCS angina classification. This was mainly driven by HR reduction. However, emerging data suggest that ivabradine also exerts other actions, since it also improves endothelial function, 29 while it attenuates the progression of atherosclerosis. 30 In addition, ivabradine also improves left ventricle diastolic function, 31 as well as coronary flow reserve 32 and coronary collateral function in patients with chronic stable CAD, effects that influence ischemia at least to the same degree as HR reduction. 33 Finally, there are studies suggesting that ivabradine administration also improves hyperemic coronary flow velocity and coronary flow reserve in patients with stable CAD. These effects remained even after HR was restored by pacing correction, indicating improvement in microvascular function, 34 which is frequently altered in patients with angina. 35
The improvement in symptoms with ivabradine restored a level of satisfactory usual activity, and this was reflected in QOL. This is an essential finding since the data regarding QOL and antianginal treatment in this population are few and inconsistent. In the Angina Prognosis Study in Stockholm (APSIS), 36 uptitration of metoprolol and verapamil to target dosage in 800 patients with stable angina was not related to a significant improvement in QOL after 3.4 years of follow-up. In the present study, the improvement in QOL was mainly related to HR-lowering effect of ivabradine and not to β-blocker dosage, since the difference in HR was not statistically significant in patients receiving ≥50% or <50% of the target β-blocker dose. In addition, the magnitude of QOL improvement (by 15.5 points) is in line with a previous report, where ivabradine administration resulted in an improvement in EQ-5D VAS score by 15.3 points. 5
The question may arise whether uptitration of β-blockers at target dose could achieve the same results. However, according to several studies and registries mentioned earlier, in everyday clinical practice, uptitration of a β-blocker to optimum dose presents difficulties and is rarely achieved. 24,26,37 Patients may not be able to tolerate higher doses for hemodynamic reasons or due to noncardiac adverse effects or a more severe medical condition. Also, in terms of survival, the contribution of β-blocker therapy is not as prominent. 37,38 Moreover, it appears that the dosage of a β-blocker is not always related to HR reduction, 27,28 while there are clear data from double-blind controlled studies proving that adding ivabradine to a β-blocker is more effective (in terms of antianginal effect) than the uptitration of a β-blocker in patients with stable angina. 7,39
In terms of survival, ivabradine addition does not improve prognosis in patients with stable angina and CAD without left ventricular systolic dysfunction (LVSD). 40 In the Study Assessing the Morbidity–Mortality Benefits of the If Inhibitor Ivabradine in Patients with Coronary Artery Disease (SIGNIFY) study, although ivabradine addition improved symptoms, it did not reach the primary outcome, while in a prespecified subgroup analysis of patients with angina CCS II-IV, it was associated with an increase in the primary end point (cardiovascular death and nonfatal infarction). However, we have to keep in mind that in the SIGNIFY study, the dose regimen used was above the maximal dose of the product summary characteristics (SmPC), with a target dose of 10 mg twice daily instead of 7.5 mg twice daily. In addition, drugs such as verapamil or diltiazem were coadministered; it is now well known that these drugs can triple the plasma concentration of ivabradine, 41 which was already higher than that approved by the ivabradine SmPC. Thus, the European Medicines Agency has reaccredited the use of ivabradine in patients with stable CAD without LVSD, 41 since it is effective in reducing angina at the dose regimen suggested in the SmPC.
Adherence to treatment with ivabradine was high. During the total duration of the trial, 884 (95.5%) patients were taking their treatment everyday or quite often, while 408 patients (44.1% of the total sample) were administered a constant dosage of ivabradine. The increased adherence to treatment may be explained by the antianginal efficacy and the few adverse events of ivabradine.
Noninterventional studies reflect the routine clinical management adopted by treating physicians. Those studies also include patients with comorbidities who are usually excluded from clinical trials, and in conjunction with randomized controlled studies provide additional information regarding the burden of the disease in question. 42 Finally, this study also included a significant number of patients >75 years old (22% of the sample) who are usually represented in a small percentage in randomized clinical trials regarding coronary syndromes (≈7%). 43
Limitations
This was a post hoc analysis, and, therefore, the results should be considered as hypothesis generating. However, the sample size was relevant, and the results are plausible and in line with previous data for ivabradine in a pure anginal population. 5 –8 In addition, this was an observational study. Thus, there is no control group, while patient enrollment was sequential and no randomization was implemented. However, patients enrolled and practices are representative of the daily clinical management in private cardiology offices. Moreover, the study had a relatively short duration, whereas large randomized, double-blind, placebo-controlled trials that have established the role of ivabradine had a significantly larger duration. 26,44
Conclusion
Ivabradine administration on top of optimal individualized dose of β-blockers is associated with a decrease in angina events and nitroglycerin consumption and with an improvement in angina classification and QOL in patients with stable angina and history of coronary revascularization.
Footnotes
Authors’ Note
On behalf of the investigators of the “Prospective, noninterventional, observational study of the antianginal efficacy of ivabradine during a 4-month treatment of a Greek population with coronary artery disease.” All authors made substantial contributions to (1) conception and design or acquisition of data or analysis and interpretation of data and (2) drafting the article or revising it critically for important intellectual content. All authors approved the final version to be published.
Investigators of “Prospective,noninterventional,observational study of the antianginal efficacy of ivabradine during a 4-month treatment of a Greek population with coronary artery disease”
Akifoglou Birol, Afaras Georgios, Agathos Athanasios, Aggistrioti Aglaia, Agrafiotis Elias, Albanis Charalabos, Aldakos Georgios, Aleksandridis Elias, Aleksoudis Apostolos, Almaidi Irini, Anastopoulos Panagiotis, Antonakis Vasilios, Antoniou Ioannis, Apostolopoulos Athanasios, Argiriou Theodoros, Arvanitakis Georgios, Arvanitis Konstantinos, Asimakopoulos Christos, Babarakos Anastasios, Babas Georgios, Bakiris Pavlos, Bakirtzis Athanasios, Bakirtzis Pantelis, Balaskas Andreas, Banias Dimitrios, Benis Thomas, Beroukas Antonios, Bogiatzis Dimitrios, Bountioukos Emmanouil, Charaktsis Ioannis, Charbas Christos, Chasapis Dimitrios, Chatzisavas Spiridon, Chondrokoukis Georgios, Chorozopoulos Emmanouil, Chousakos Panagiotis, Christodoulou Spiridon, Christogiannis Zacharias, Christoulakis Stelios, Dalamagka Emmanouela, Demerouti Eftichia, Dermitzakis Georgios, Dimitriadou Aleksandra, Dimopoulos Panagiotis, Dimopoulos Vasileios, Dimoulis Nikolaos, Doulgeridis Panagiotis, Drakos Thomas, Drolias Apostolos, Efthimiou Georgios, Ellinoudis Georgios, Floros Dimitrios, Fotopoulou Vasiliki, Fournarakis Georgios, Fragkiadakis Charalabos, Galanouli Vasiliki, Gavrielatos Gerasimos, Georgakis Andreas, Georgakis Antonios, Georgariou Dimos, Georgariou Kiriakos, Gerasimidou kaltsa Ioanna, Geropoulos Vasilios, Giannakodimos Vasilios, Giannoulis Thomas, Giazitzoglou Eleftherios, Gkentsidis Stilianos, Gkilitsis Christos, Gkiokas Stefanos, Gkiti Eleni, Gkotsis Konstantinos, Gkoutzios Theodoros, Gogou Maria, Goupios Ioannis, Gourgiotis Kiriakos, Graikos Athanasios, Grapsa Georgia, Grigorakis Panagiotis, Grigoriadou-Skouta Eleni, Grillis Nikolaos, Ipirotis Konstantinos, Kabitsi Efterpi, Kakedis Spiridon, Kallintzi Kalliopi, Kalos Aggelos, Kamvrogiannis Panagiotis, Kanellopoulos Konstantinos, Kapetanios Konstantinos, Kara ali Chairidin, Karakoulakis Sokratis, Karalioliou Silvia, Karavasilis Konstantinos, Kardogiannis Theodoros, Karouzos Nikolaos, Kassos Dimitrios, Katelouzos Nikolaos, Katsaflianis Asterios, Katsaris Christos, Katsoulas Triantafillos, Kavakaki Evagelia, Kazakos Evangelos, Kenellos Georgios, Kioupeloglou Georgios, Kipouridis Nikolaos, Kiriazopoulos Panagiotis, Kitikidou Korina, Klapsinos Nikolaos, Klidarias Margaritis, Kontopoulos Georgios, Kopsida Zeta, Kostakis Georgios, Kostoulas Ioannis, Kotridis Panagiotis, Kotsaridis Avraam, Koukoulas Andreas, Koukoulekidis Georgios, Kouremetis Michail, Kourouklis Spiridon, Koutras Ioannis, Koutrouli Eleanna, Koutsakis Georgios, Koutsimanis Vasilios, Krobas Nikolaos, Labiris Nikolaos, Labrou Ioannis, Labrou Xrisostomos, Lafazanis Georgios, Lagoudi Eleni, Lefakis Michail, Logothetis Dimitrios, Loukatzikou Anna-Aleksandra, Loukeris Konstantinos, Madas Antonios, Mainas Konstantinos, Makaronas Georgios, Makrakis Georgios, Marakas Stilianos, Markatou Paraskevi, Marketakis Dimitrios, Markoulis Theocharis, Marousis Panagiotis, Martiadou Konstantina, Martsekis Loukas, Matziridis Anestis, Mavrepis Ioannis, Mavridis Aggelos, Mavrothalassitis Chrisostomos, Mazaraki Despina, Meidanis Evaggelos, Mentesidis Dimitrios, Meras Michail, Michailidis Georgios, Micheloggonas Ioannis, Mitakidou Anastasia, Mitrou Vasilios, Mitroulas Christos, Moschidis Athanasios, Nasiadis Ioannis, Nikiforos Savvas, Nikolakeas Stefanos, Nikolaou Attalos, Nikolopoulos Christos, Nomikos Vasilios, Orkopoulos Anestis, Panagiotopoulos Grigorios, Panagoulias Georgios, Pantelia Maria, Papachristos Christos, Papadakis Emmanouil, Papadakis Miltiadis, Papadakis Panagiotis, Papadatou Aggeliki, Papadimitriou Christos, Papadimitriou Evaggelos, Papadopoulos Apostolos, Papadopoulos Dimitrios, Papadopoulos Georgios, Papadopoulos Paris, Papageorgiou Anastasios, Papaioannou Georgios, Papargiriou Theodoros, Papastamou Christos, Papavasiliou Dimitrios, Pappas Panagiotis, Pardalis Elias, Patsilinakos Aleksandros, Pegka Evgenia, Petinakis Pantelis, Petras Charalabos, Petrogiannis Spiros, Pilis Antonios, Pinnas Michalis, Pollatos Dionisios, Prattis Nikolaos, Primerakis Georgios, Psarogianni Paraskevi, Psilogenis Christos, Raftopoulos Leonidas, Reppas Evaggelos, Riga Maria, Routsakos Damianos, Samartzi Maria, Sarantakos Nikolaos, Sassalos Konstantinos, Savvopoulou Gkolfo, Servetas Nikolaos, Sfikas Georgios, Sikiotis Ioannis, Siliogkas Georgios, Siskos Georgios, Skarpas Konstantinos, Sofilas Kosmas, Soulas Dimitrios, Stamatopoulos Georgios, Stathakopoulos Dimitrios, Stathopoulou Konstantina, Stavropoulos Rafail, Stefanakis Emmanouil, Stergiou Aggeliki, Stergiou Leonidas, Stratis Panagiotis, Tanidou Paraskevi, Tasoulas Elias, Teneketzi Eleni, Theofilis Anastasios, Toumanidis Iraklis, Tsaknakis Leonidas, Tsamis Nikolaos, Tsavdaris Konstantinos, Tsirakis Panagiotis, Tsotsoros Nikolaos, Tzeltzes Georgios, Tzortzis Kiriakos, Vakalis Ioannis, Vardakis Konstantin
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I Zarifis has received honoraria for advisory boards from SERVIER HELLAS, V Grammatikou and E Kallistratos are employed by the Medical department of SERVIER HELLAS, A. Katsivas has no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by SERVIER HELLAS.