
Abstract
Background
Patient Safety Indicators (PSIs) are quality metrics developed by the Agency for Healthcare Research and Quality (AHRQ) to identify potentially preventable postoperative complications. The rate of PSIs after lung resection remains poorly defined.
Methods
We retrospectively reviewed our institutional database for all lung resection patients age ≥16 from 2014 to 2024. Patient Safety Indicators evaluated were PSI-9 (hemorrhage/hematoma), PSI-10 (acute kidney injury requiring dialysis), PSI-12 (peri-operative pulmonary embolism [PE] or deep vein thrombosis [DVT]), and PSI-13 (post-operative sepsis). The primary outcome was the incidence of preventable PSIs following lung resection. Secondary outcomes included clinical predictors of PSI, short-term outcomes by PSI status, and PSI-related costs.
Results
Among 2701 lung resection patients, 35 (1.29%) experienced at least one PSI, totaling 43 PSI events (1.59%). Patient Safety Indicator patients were more often male (65.7% vs 48.3%, P = .04), had higher comorbidity burden (Charlson-Deyo 3+: 97.1% vs 73.5%, P = .02), and more frequently had prior lung cancer (80.0% vs 52.3%, P = .001). Patient Safety Indicator patients had higher 30-day mortality (11.4% vs 1.2%, P < .001). Logistic regression identified male sex (aOR 2.20 [1.08-4.46], P = .03) and prior lung cancer (aOR 2.95 [1.22-7.12], P = .02) as independent predictors of PSI. After review, 37 PSIs were classified as preventable or possibly preventable (1.37%), generating an estimated cost burden of $983,059 and largely driven by PSI-13 sepsis events.
Conclusion
Although PSIs after lung resection are infrequent, focus on preventing post-operative adverse outcomes should remain paramount. Targeted strategies to prevent these preventable complications can help improve outcomes and provide a significant cost-saving opportunity.
Keywords
Key Takeaways
• Most PSIs after lung resection were preventable, with post-operative sepsis (PSI-13) accounting for most events and associated costs, which highlights pneumonia prevention, aspiration mitigation, and early infection recognition as critical quality-improvement targets. • Patient Safety Indicators were more common in high-risk subgroups, including patients with higher comorbidity burden, prior lung cancer, longer operations, and more extensive resections, suggesting that tailored post-operative monitoring and risk-adjusted care pathways may reduce preventable harm. • Institutional initiatives to improve documentation accuracy and PSI validation contributed to declining PSI rates over time, underscoring the importance of documentation integrity in both quality measurement and reducing false-positive PSI events.
Introduction
Patient Safety Indicators (PSIs), developed by the Agency for Healthcare Research and Quality (AHRQ), are standardized quality metrics derived from administrative data that are designed to identify preventable in-hospital complications and adverse events following surgery.1,2 Patient Safety Indicators use diagnosis- and procedure-based coding algorithms to flag events such as post-operative hemorrhage, acute kidney injury requiring dialysis, venous thromboembolism, and sepsis. Patient Safety Indicators are widely adopted by health systems as benchmarks of surgical quality and patient safety. Furthermore, PSI-associated complications have been consistently linked to increases in hospital stay, readmissions, and health care expenditures. 3
Although PSIs have been applied across surgical fields, their performance and clinical relevance in thoracic surgery, particularly after lung resection, remain insufficiently characterized. Lung resection carries unique risks related to pulmonary function, post-operative infection, and thromboembolic events, making early identification of preventable harm critically important. Previous studies have emphasized the relationship between post-operative complications, increased mortality, and prolonged recovery in thoracic surgery patients. 4 However, the true incidence and preventability of PSIs in lung resection patients have not been well described.
Accurate PSI surveillance is further challenged by the reliance on administrative coding algorithms, which may misclassify clinical events without rigorous documentation review. 5 As institutions increasingly incorporate PSIs into quality-improvement initiatives, understanding their incidence, clinical predictors, and associated financial impact has become essential. 6 The objective of this study was to evaluate the frequency and preventability of PSIs following lung resection at a high-volume academic medical center over a 10-year period. We also assessed patient- and procedural-level factors associated with PSI occurrence and the estimated financial burden of these events using established national cost data.
Methods
This retrospective cohort study included all patients who underwent lung resection at a single academic medical center between January 2014 and December 2024. The study was exempt from IRB approval. All patients age 16 years or older who underwent lung resection during this period were included. Patients with missing surgical information, missing PSI data, or incorrect PSI documentation were excluded. Demographic variables included age, sex, race/ethnicity, smoking history, alcohol use, drug use history, and comorbidity burden using the Charlson-Deyo comorbidity (CDC) index. Clinical history included prior cancer and prior lung cancer. Operative variables included approach (open, VATS, robotic), laterality, and procedure type. Post-operative outcomes included readmission status, 30-day/90-day mortality, and survival status at last follow-up. The primary outcome was the incidence of preventable PSIs following lung resection. Secondary outcomes included total and preventable PSI-related costs, clinical predictors of PSIs, and short-term outcomes by PSI status.
Patient Safety Indicators were defined according to the AHRQ algorithms based on ICD-coded data and post-operative clinical documentation. Our study evaluated four PSIs, which included the following: PSI-9: post-operative hemorrhage or hematoma, PSI-10: acute kidney injury (AKI) requiring dialysis, PSI-12: peri-operative pulmonary embolism (PE) or deep vein thrombosis (DVT), and PSI-13: post-operative sepsis. For PSI-13, infections were separated into pneumonia, bacteremia, urinary tract infection (UTI), or multiple sources. PSI-11 (post-operative respiratory failure) was excluded, as lung cancer patients are not eligible for this indicator. Because PSIs represent potentially preventable events, each identified PSI underwent structured case-level review to determine preventability. The study authors reviewed operative notes, clinical documentation, and post-operative course and assessed preventability using clinical judgment, classifying events as preventable/possibly preventable or not preventable. Importantly, all PSI events at our institution are independently reviewed by an institutional clinical quality and patient safety team, which includes clinicians and quality specialists with expertise in PSI evaluation. The findings from this formal quality review process were incorporated into the final preventability classification. Cost estimates were derived from previously published national cost data for each PSI category.7,8
For statistical analysis, continuous variables were summarized as median with interquartile range, and categorical variables as frequency and percentage. Comparisons between patients with and without PSIs were done using chi-square test for categorical variables and the Wilcoxon rank sum for continuous variables. A multivariable logistic regression was constructed to identify independent predictors of PSI occurrence; covariates were selected based on clinical relevance. All statistical analyses were performed using STATA 19.5 (StataCorp).
Results
Baseline Characteristics and Operative Details Stratified by PSI Status After Lung Resection
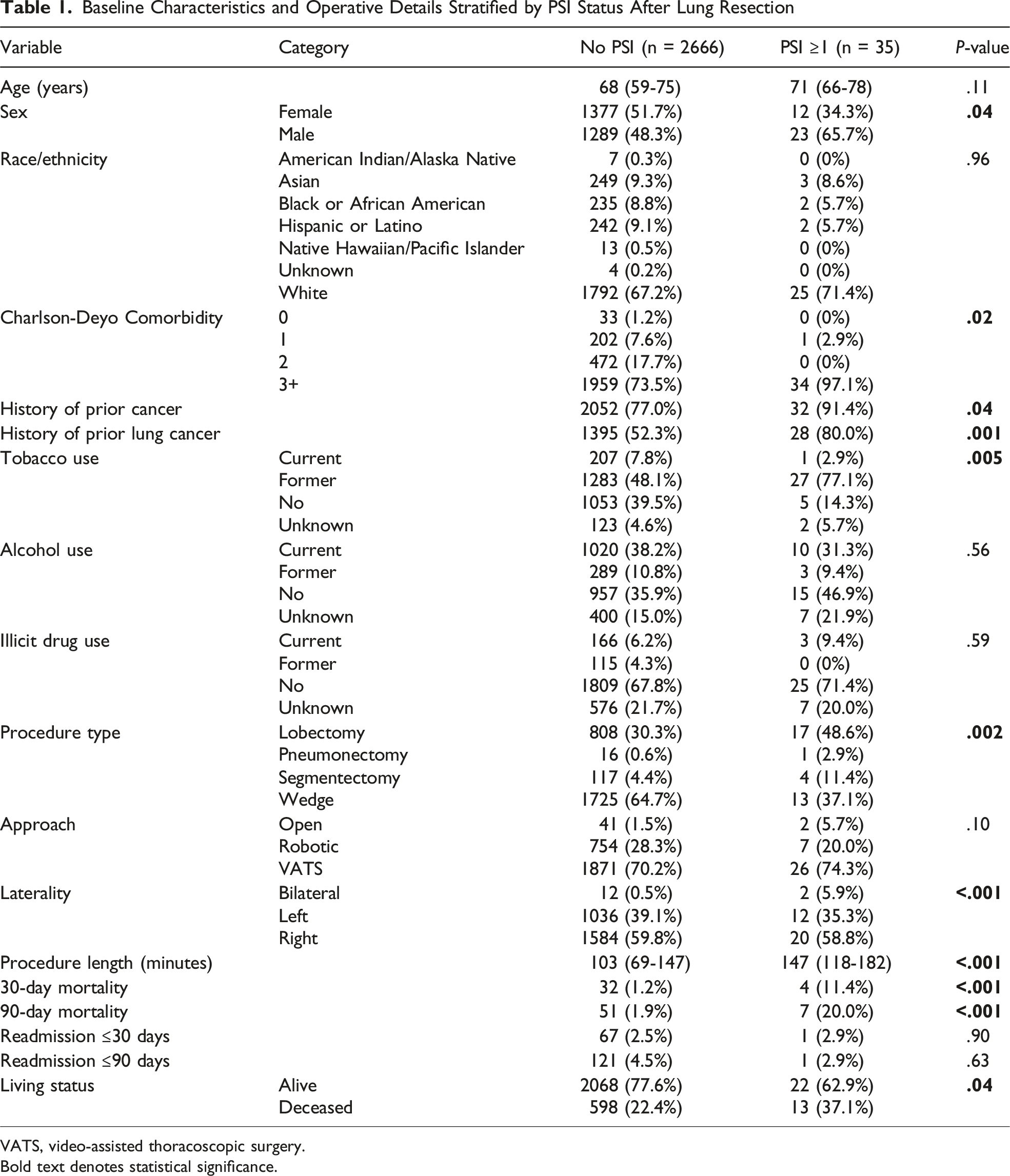
VATS, video-assisted thoracoscopic surgery.
Bold text denotes statistical significance.
Multivariable Logistic Regression for Predictors of PSI
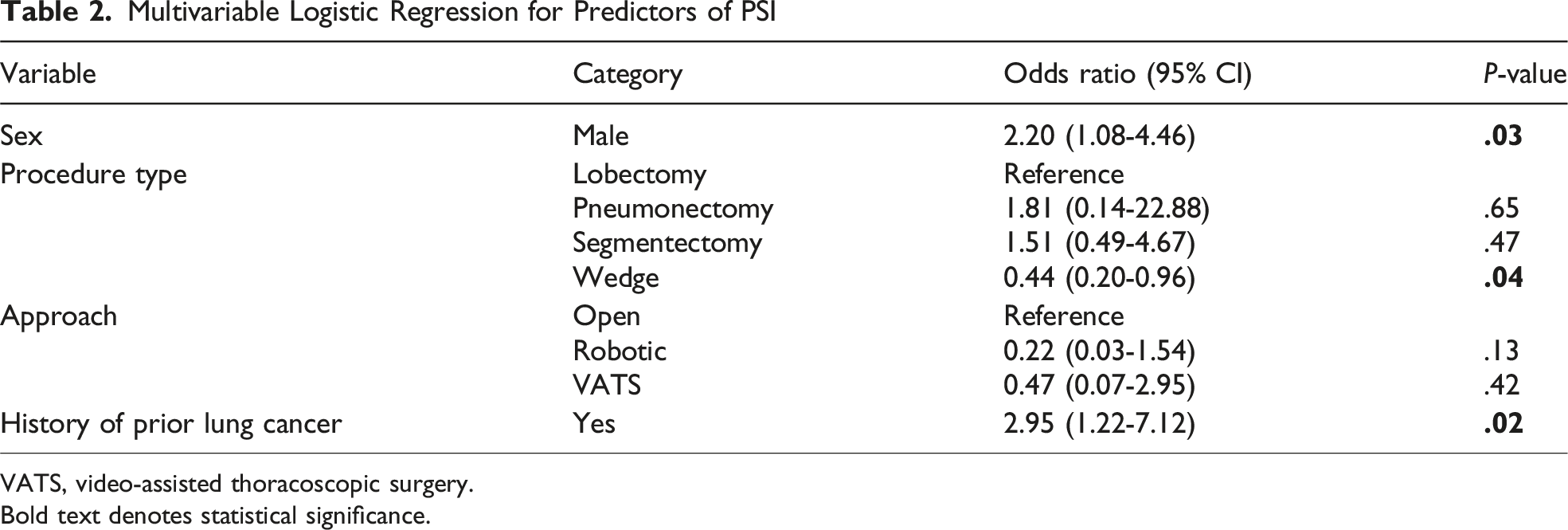
VATS, video-assisted thoracoscopic surgery.
Bold text denotes statistical significance.
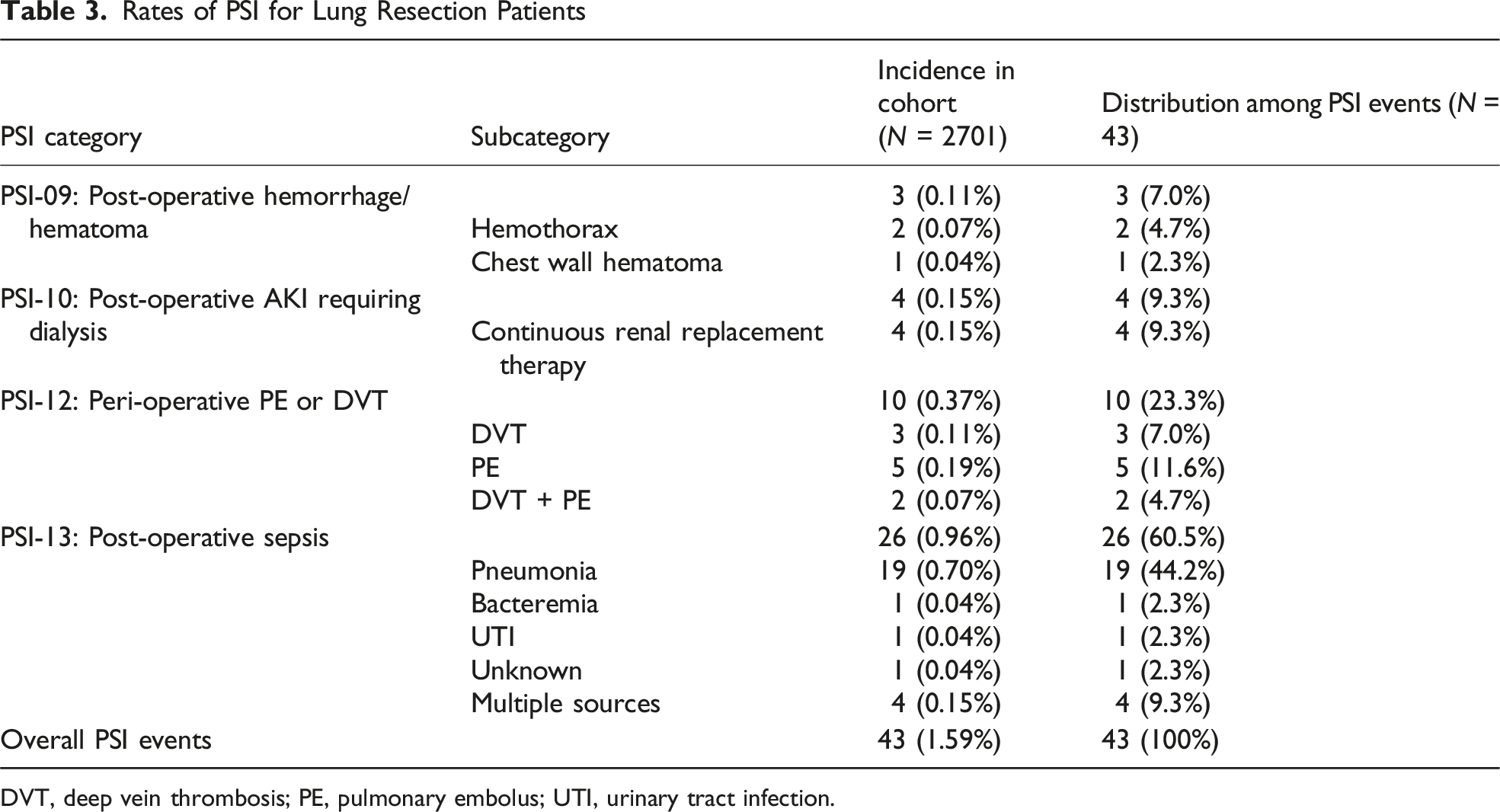
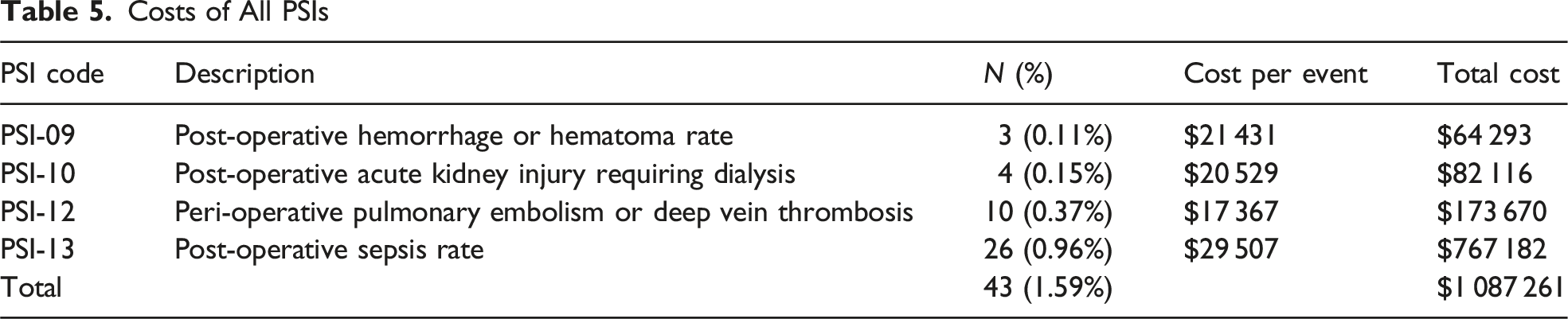
Year-by-year analysis demonstrated that PSIs were more common in the earlier years (2014: 27.9%, 2015: 23.3%, Figure 1). The distribution of PSIs is listed in Table 3, which include the following: PSI-9: 3 (0.11%, 2 hemothorax and 1 chest wall hematoma), PSI-10: 4 (0.15%), PSI-12: 10 (0.37%, 5 PE, 3 DVT, 2 DVT + PE), and PSI-13: 26 (0.96%, 19 pneumonia, 1 bacteremia, 1 UTI, 1 unknown, and 4 with multiple sources). After structured case review, 37 PSIs (1.37%) were classified as preventable or possibly preventable and included the following: PSI-9: 3 (0.11%), PSI-10: 4 (0.15%), PSI-12: 4 (0.15%), and PSI-13: 26 (0.96%, Table 4). Temporal trend of PSIs 9, 10, 12, and 13 by year Rates of PSI for Lung Resection Patients DVT, deep vein thrombosis; PE, pulmonary embolus; UTI, urinary tract infection. Costs of Preventable or Possibly Preventable PSIs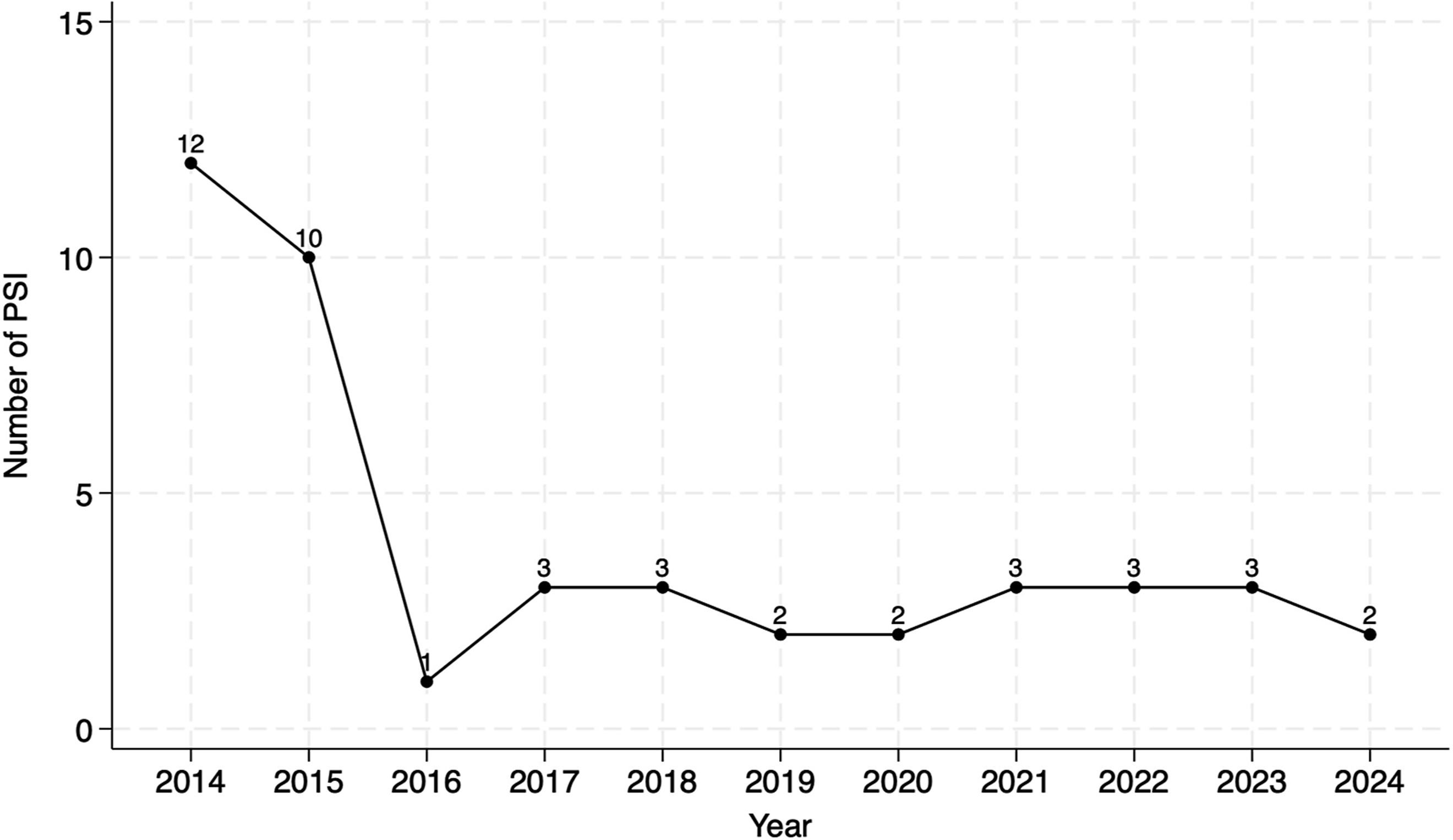
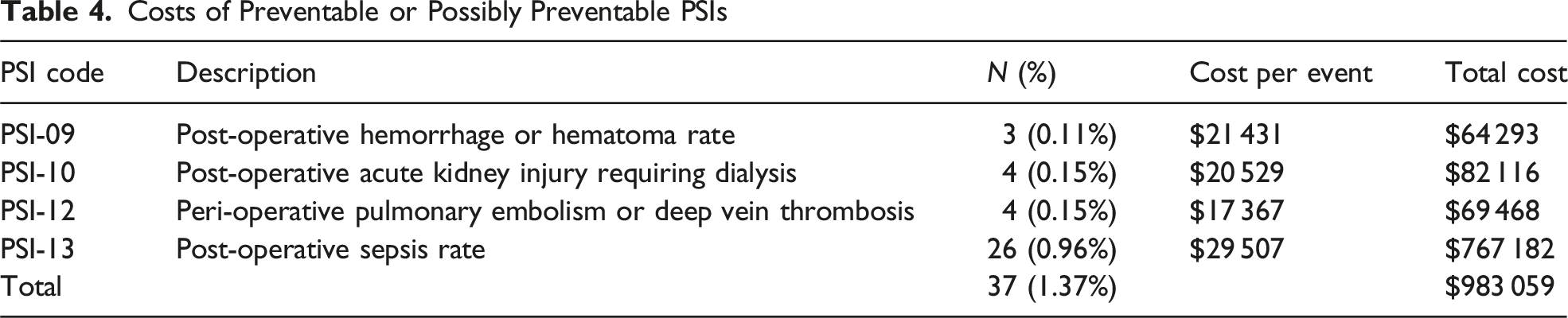
Costs of All PSIs
Discussion
In this 10-year retrospective cohort of 2701 lung resection patients, PSIs occurred infrequently, with only 1.59% of patients experiencing at least one event. Despite their low incidence, PSI events were associated with clinically meaningful differences in patient characteristics, procedural factors, and post-operative outcomes. Our findings suggest that underlying patient complexity and operative intensity are important contributors to PSI occurrence, consistent with prior thoracic risk modeling studies. 9 In addition to quality-improvement efforts and standardization of care among thoracic surgeons, the downward trend of PSI events over the study period also reflects institutional efforts to enhance documentation improvements, which reduced inadvertent PSI misclassification and improved PSI reporting.
Patient Safety Indicators are designed to identify potentially preventable post-operative events, which should not occur in routine, uncomplicated surgical care. 1 In our study, 37 of the 43 PSIs (1.37% of the entire cohort) were deemed preventable or possibly preventable after case review. The predominance of PSI-13 (post-operative sepsis), largely driven by pneumonia, highlights post-operative infection as the most important preventable complication in thoracic surgery. Prior investigations have similarly shown that pneumonia is a leading cause of morbidity after lung resection and a major driver of delayed recovery and mortality.10,11 Many of the PSI-13 cases occurred despite opportunities for earlier recognition of clinical deterioration or incomplete implementation of preventive measures, which highlights system-level targets for improvement. Given the prevalence of PSIs in patients with prior lung cancer and higher comorbidities, our findings highlight the need for tailored, proactive post-operative monitoring in high-risk patients and in those with diminished pulmonary reserve. 12
Similarly, PSI-12 events (post-operative DVT/PE) were also frequently classified as preventable. Review of these cases identified incomplete adherence to chemoprophylaxis timing, interruptions in prophylaxis, or prior central line placement. Our findings reflect national data that venous thromboembolism after thoracic surgery is both under-recognized and preventable with adherence to prophylaxis protocols and timely post-operative assessment.13,14 While PSI-9 (hemorrhage/hematoma) and PSI-10 (AKI requiring dialysis) were less common, most of these events were also labeled as preventable. Prior literature has also shown that post-operative bleeding and AKI often reflect care-process lapses instead of unavoidable physiological events.15,16
Patient Safety Indicators provide an opportunity to identify potentially avoidable harm. In our study, PSI events were associated with longer operations, high comorbidities, prior cancer, and more extensive lung resections, offering actionable insight into which patient populations warrant heightened surveillance. Furthermore, multivariable analysis showed that male sex and history of lung cancer increased PSI risk, while wedge resections were protective, providing further insight to refine pre-operative counseling, risk stratification, and targeted post-operative pathways.
Although the financial implications of PSI events were substantial, with preventable PSIs nearing $1 million in costs, the primary significance of these findings lies in the opportunity to intervene. Preventable complications represent the most meaningful quality-improvement targets because they directly reflect modifiable aspects of care delivery. As thoracic surgery continues to evolve toward minimally invasive approaches and enhanced recovery paradigms, systemic efforts to reduce preventable PSIs, particularly pneumonia and thromboembolic events, may yield the greatest improvements in patient outcomes.
Our study has some limitations. It is retrospective, single-center, and limited by the inherent constraints of PSI definitions. Patient Safety Indicators are derived from administrative coding algorithms and are sensitive to the accuracy and timing of clinical documentation. 5 Poor documentation can falsely trigger a PSI, which is why each PSI case was thoroughly reviewed. Also, PSI preventability status was determined after review, which is susceptible to subjectivity and potential bias. Our cost analysis was done using prior published data, which may be outdated. Lastly, our small PSI cohort limits statistical power to fully evaluate outcomes within this group.
Nevertheless, the study represents a comprehensive institutional analysis of PSIs following lung resections and illustrates the strengths of PSI metrics as a quality indicator. Future initiatives should focus on strengthening pneumonia-prevention bundles, optimizing DVT/PE prophylaxis adherence, improving clinical documentation accuracy, and deploying real-time PSI surveillance tools to reduce preventable harm. By prioritizing preventability rather than simply quantifying post-operative outcomes, institutions can more effectively target quality-improvement resources and improve both clinical and operational outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure Statement
Drs. Harmik Soukiasian and Andrew Brownlee are consultants for Intuitive. The other authors have nothing to disclose.
Meeting Presentation
The abstract will be presented at the American College of Surgeons Southern California Chapter annual meeting in Santa Barbara, CA, on January 10, 2026.