
Abstract
Background
Pneumonectomy remains a rare trauma procedure due to its high morbidity and mortality. While previous studies suggest that right-sided pneumonectomy is associated with a higher mortality in patients with lung cancer, there are scarce data in trauma. We aimed to compare patient outcomes following right-sided and left-sided pneumonectomy after trauma.
Methods
This is a retrospective cohort study using the American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) database (2016-2022). Trauma patients (age ≥16 years) who underwent pneumonectomy were included and stratified by the laterality of pneumonectomy. Patient baseline characteristics, injury profile, and clinical outcomes were compared between the right- and left-sided pneumonectomy groups. Multivariable analysis was performed to evaluate the association between the laterality of pneumonectomy and in-hospital mortality.
Results
A total of 301 patients were included. The median age was 30 years, and 85.3% were male. Of those, 137 patients (45.5%) underwent right-sided pneumonectomy. Admission vital signs and Injury Severity Score were comparable between the right- and left-sided groups. Extracorporeal membrane oxygenation (ECMO) was used more frequently in right-sided pneumonectomy patients (8.8% vs 2.4%, P = 0.015). In-hospital mortality following right- and left-sided pneumonectomy was 54.0% and 48.2%, respectively (P = 0.313). In the multivariable logistic regression, right-sided pneumonectomy was not associated with increased odds of in-hospital mortality (adjusted odds ratio: 1.137, confidence interval: 0.641-2.015, P = 0.662).
Conclusion
This study suggests that the laterality of pneumonectomy was not associated with an increased risk of in-hospital mortality. Future research should evaluate the utility of ECMO in trauma patients requiring pneumonectomy.
• Right-sided trauma pneumonectomy was not associated with higher in-hospital mortality compared with left-sided pneumonectomy, suggesting that laterality alone should not drive operative decision-making. • Right-sided pneumonectomy more frequently required ECMO support, likely reflecting greater physiological derangement and underscoring the need for a multidisciplinary approach for cardiopulmonary support.Key Takeaways
Introduction
Trauma pneumonectomy remains one of the least-studied procedures in contemporary trauma care, occurring in only 0.01% of traumatic injuries, with lung resections overall reported in just 0.08%. 1 Although modern techniques such as tractotomy and non-anatomic wedge resection are increasingly preferred, a complete pneumonectomy may still be necessary to control hilar bleeding or when pulmonary and bronchial injuries are irreparable. 2 Nevertheless, trauma pneumonectomy carries high mortality, with reported rates ranging from 50 to 100%. 1,3–6 The physiology associated with removing a substantial portion of the pulmonary circulatory reserve can lead to devastating postoperative complications such as acute right-heart failure,7–9 acute respiratory distress syndrome (ARDS),10,11 mediastinal shifting with vascular/airway compromise, 12 and bronchopleural fistula. 9 Previous work in animal models demonstrated that, in the short-term, a significant part of this mortality is due to a rapid increase in pulmonary vascular resistance and the resultant right-heart failure, a phenomenon worsened in the setting of concomitant hemorrhagic shock. 8 Despite potential complications, pneumonectomy may be the most effective or only option in a selected group of patients who are actively bleeding and hemodynamically unstable. 13
To date, multiple studies have reported the outcomes of pneumonectomy in the non-trauma setting, both for benign14,15 and malignant diseases. 16 Importantly, several studies have addressed the differences in outcome based upon the laterality of pneumonectomy, indicating that patients undergoing right-sided pneumonectomy have an increased risk of mortality and postoperative complications such as bronchopleural fistula.17–21 However, patients undergoing pneumonectomy for malignancy often have underlying cardiovascular and pulmonary comorbidities, 22 whereas trauma patients are generally younger, healthier, and frequently present in hemorrhagic shock, potentially resulting in different outcomes. 23 Trauma literature has largely evaluated pneumonectomy as a single entity, without specifically assessing the impact of laterality, particularly for right-sided resections. This is partly because previous International Classification of Diseases (ICD)-9 procedure codes did not distinguish between right and left pneumonectomy, making it difficult to assess laterality in database studies. Additionally, single-center studies often lack sufficient patient numbers to draw robust conclusions. To date, there are scarce data regarding the effect of laterality on survival following trauma pneumonectomy, and addressing this gap could guide surgeons in decision-making and strategies to improve outcomes in these high-risk patients.
The purpose of this study is to present the largest contemporary analysis of trauma pneumonectomy using a nationwide trauma data set, providing an objective comparison of outcomes between right- and left-sided resections, along with a detailed description of mortality timing and the perioperative course. We hypothesized that right-sided pneumonectomy would be associated with worse outcomes compared with left-sided resections in the trauma population.
Methods
Study Design and Patient Eligibility
The study was approved by the Institutional Review Board at the University of Southern California. This is a retrospective cohort study using the American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) database between January 2016 and December 2022. We included trauma patients (age ≥16 years) who underwent pneumonectomy identified by using the ICD-10 codes (right-sided pneumonectomy: 0BTK0ZZ and left-sided pneumonectomy: 0BTL0ZZ). Exclusion criteria included patients who underwent bilateral pneumonectomy, those who underwent interfacility transfer, and patients that were pronounced dead on arrival to the Emergency Department.
Data Collection and Outcomes
Patient baseline characteristics, injury profile, and clinical outcomes were compared between the right- and left-sided pneumonectomy groups. Data collected regarding patient demographics included age, sex, and comorbid conditions (smoking, hypertension, diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD)). Clinical data obtained at the time of presentation to the Emergency Department included systolic blood pressure (SBP), pulse rate (PR), and Glasgow Coma Scale (GCS). Injury profile and procedure data were abstracted to include mechanism of injury, Abbreviated Injury Scale (AIS) in each body region, Injury Severity Score (ISS), associated pulmonary hilar injury, other pulmonary procedures (wedge resection and lobectomy) prior to pneumonectomy, time to pneumonectomy, the use of extracorporeal membrane oxygenation (ECMO), and blood transfusion requirements within first 4 hours (Supplemental file 1). The primary outcome was in-hospital mortality, and secondary outcomes included pulmonary complications (pulmonary embolism (PE), ventilator-associated pneumonia (VAP), ARDS), 6-hour and 24-hour mortality, hospital length of stay (HLOS), intensive care unit (ICU) LOS, and ventilator days.
Statistical Analysis
Descriptive statistics were used to summarize the patient characteristics, injury data, and study outcomes. Continuous variables are presented as medians with interquartile ranges (IQRs), and categorical variables are presented as numbers with percentages. Comparison between categorical variables was performed with Pearson’s chi-squared test while continuous variables were compared with the Mann-Whitney U test. Multivariable logistic regression analysis was performed to evaluate the association between the laterality of pneumonectomy and in-hospital mortality. Correlation between the covariates in the regression model was tested with multi-collinearity analysis. A P-value <0.05 was considered statistically significant. All statistical tests were performed using SPSS for Mac version 23.0 (SPSS Inc, Chicago, IL). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline was followed to report the performance of the observational study (Supplemental file 2).
Results
A total of 354 pneumonectomy cases were identified in the 2016-2022 ACS-TQIP data (Figure 1). Of these, 7 patients underwent bilateral pneumonectomy and were excluded. Additionally, 43 interfacility transfer cases and 3 patients who were dead on arrival were excluded, resulting in a final cohort of 301 patients. Of those, 137 (45.5%) and 164 (54.5%) underwent right- and left-sided pneumonectomy, respectively. Patient flow diagram. ACS-TQIP: American College of Surgeons Trauma Quality Improvement Program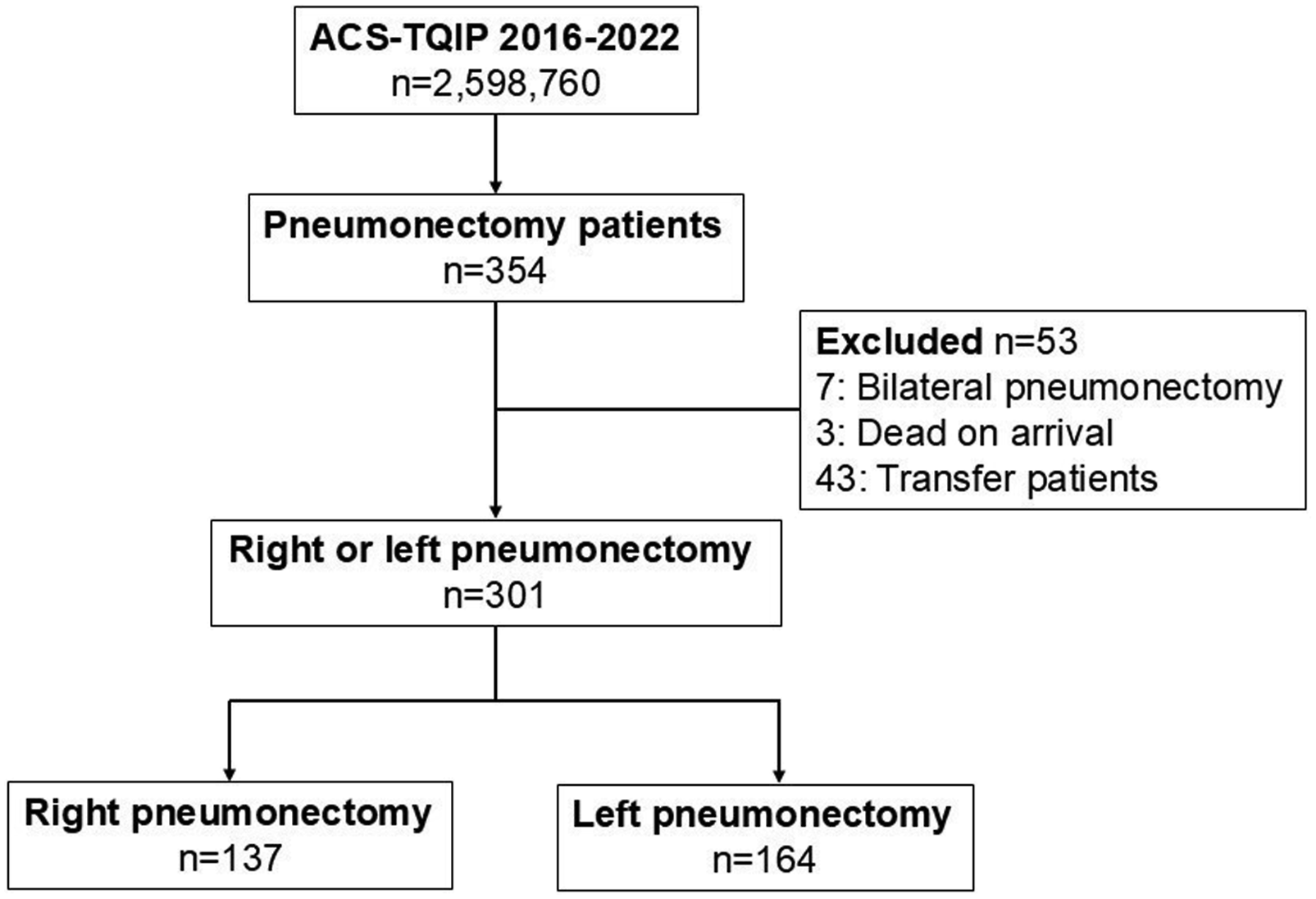
Patient and Injury Characteristics
Patient Characteristics and Therapeutic Interventions
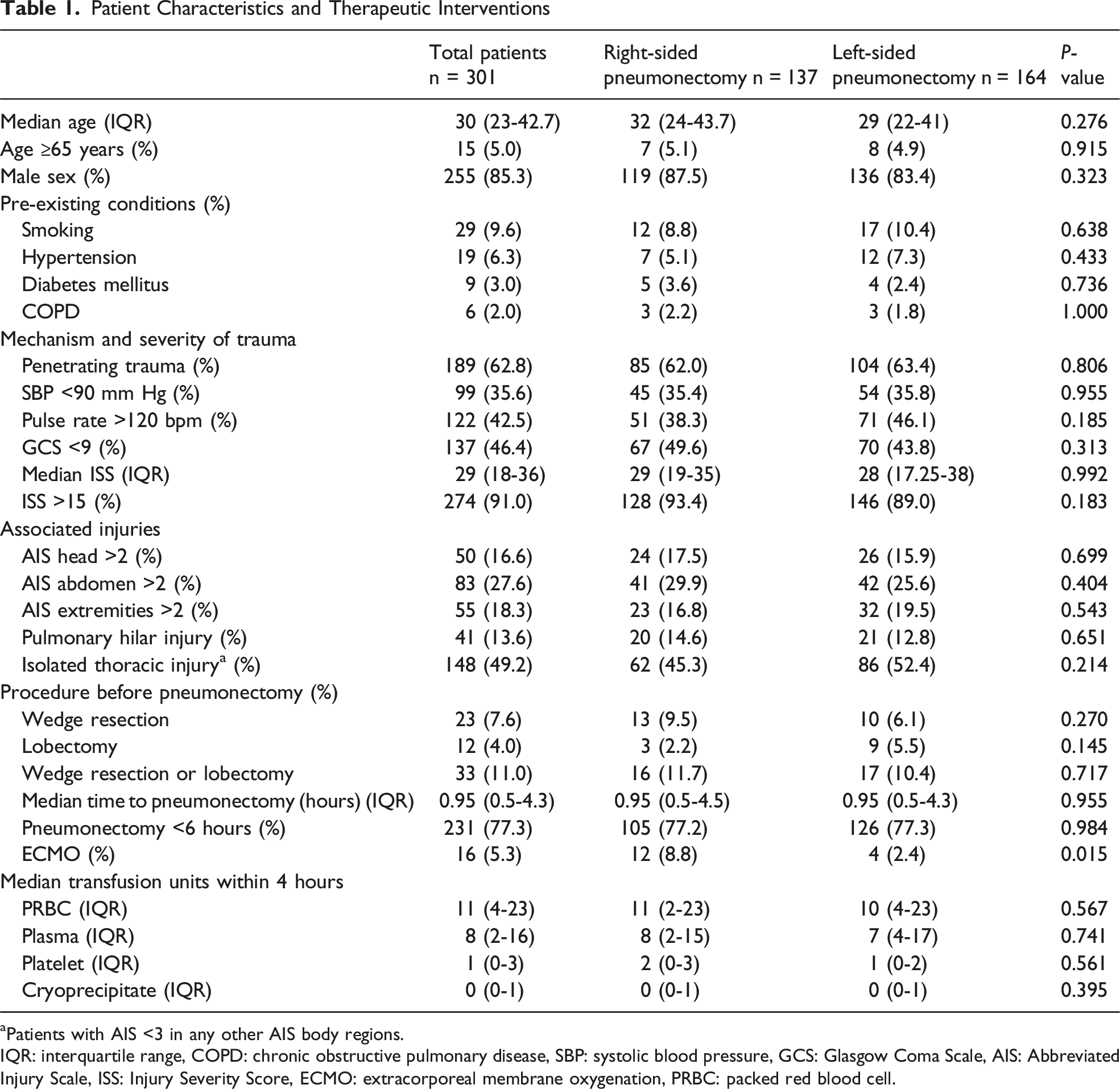
aPatients with AIS <3 in any other AIS body regions.
IQR: interquartile range, COPD: chronic obstructive pulmonary disease, SBP: systolic blood pressure, GCS: Glasgow Coma Scale, AIS: Abbreviated Injury Scale, ISS: Injury Severity Score, ECMO: extracorporeal membrane oxygenation, PRBC: packed red blood cell.
The median time to pneumonectomy was similar between the two groups, and most patients underwent pneumonectomy within 6 hours after admission (77.2% vs 77.3%, P = 0.984). Wedge resection was performed in 9.5% vs 6.1% of right- vs left-sided cases (P = 0.270), and lobectomy in 2.2% vs 5.5% (P = 0.145). Overall, either procedure was performed in 11.7% vs 10.4% of right- vs left-sided pneumonectomies, respectively (P = 0.717). ECMO, however, was significantly more frequently used in right-sided pneumonectomy patients compared to the left-sided group (8.8% vs 2.4%, P = 0.015).
Study Outcomes
Study Outcomes
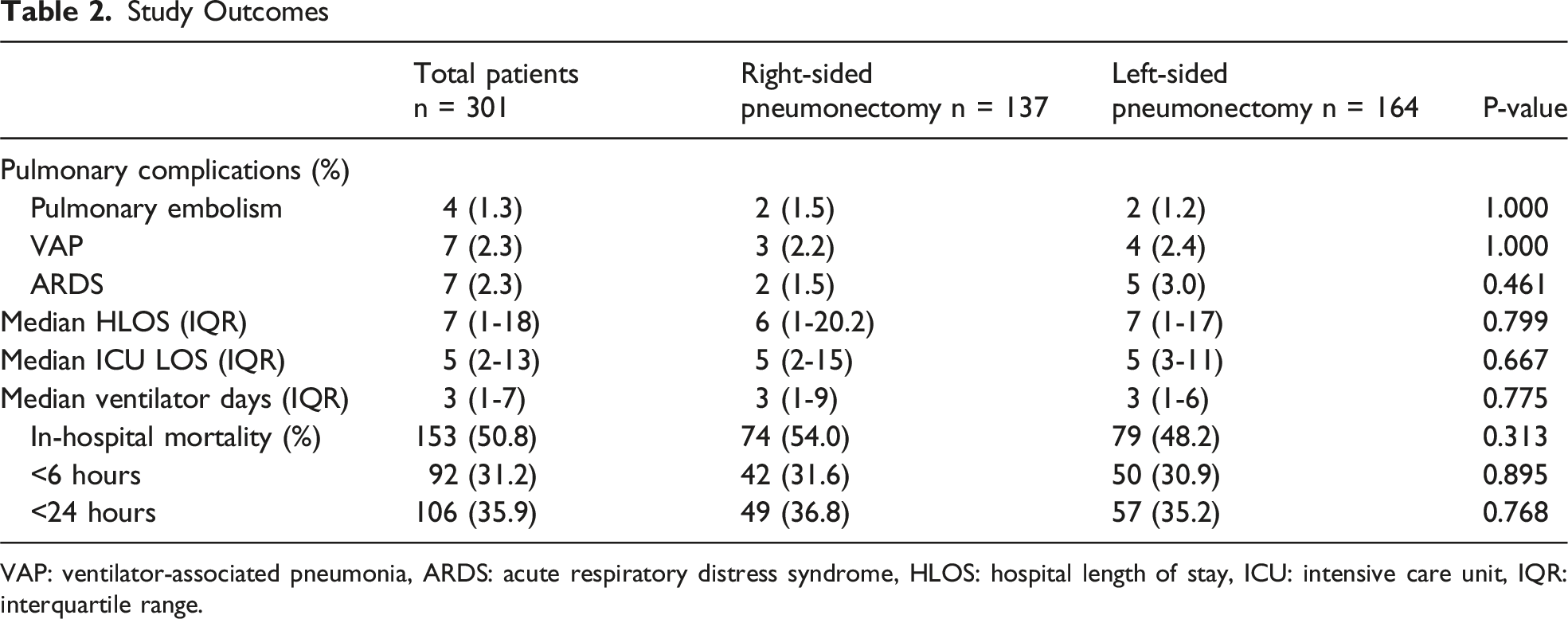
VAP: ventilator-associated pneumonia, ARDS: acute respiratory distress syndrome, HLOS: hospital length of stay, ICU: intensive care unit, IQR: interquartile range.
Logistic Regression Analysis on In-Hospital Mortality

Collinearity diagnostics for independent variables included in the binary logistic regression model. Variance Inflation Factor (VIF) values were all below 3, and tolerance values were above 0.5, indicating no significant multicollinearity among the predictors. SBP: systolic blood pressure, GCS: Glasgow Coma Scale, ISS: Injury Severity Score, AIS: Abbreviated Injury Scale, ECMO: extracorporeal membrane oxygenation.
Discussion
In this study using the ACS-TQIP, 50.8% of patients died overall, with 31.2% dying within just 6 hours. This aligns with previously reported overall pneumonectomy mortality rates of 50% to 100%.1,3–6 Importantly, our study is novel in that it specifically evaluates pneumonectomy laterality in the trauma setting, a population in which this question has not been previously studied. Our results suggest that, in trauma patients who underwent a pneumonectomy, the laterality of pneumonectomy was not significantly associated with improved or worse outcomes. This finding contrasts with prior studies in the non-trauma population, where right-sided pneumonectomy for lung malignancy has been associated with increased perioperative mortality.24,25 While the outcome between right- and left-sided pneumonectomy was similar, it is important to note that ECMO is more frequently used in patients undergoing right-sided pneumonectomy. The results may imply that right-sided pneumonectomy is associated with increased risks of cardiopulmonary complications during the perioperative period. Trauma surgeons may need to consider a multidisciplinary approach for perioperative cardiopulmonary support including the use of ECMO when performing a right-sided pneumonectomy.
Compared to left-sided pneumonectomy, right-sided pneumonectomy is considered a higher-risk procedure due to the larger size and more complex anatomy of the right lung, which can result in greater loss of alveolar volume, reduced pulmonary reserve, and impaired respiratory function. 20 In addition, the procedure can elevate pulmonary artery pressures, potentially leading to right ventricular strain or heart failure. 8 Although pneumonectomy laterality has not been specifically studied in trauma due to its rarity, oncologic studies have reported higher mortality in patients undergoing right-sided pneumonectomy, along with increased risks of ARDS, empyema, pulmonary edema, and bronchopleural fistula (BPF).15,21,26–28 One study suggested that the higher mortality associated with right-sided pneumonectomy was largely due to BPF, and optimizing surgical techniques to minimize the risk of early bronchopleural fistula could help reduce mortality. 21 Anatomical factors reported to increase BPF risk include a more exposed, less supported right bronchial stump and a right bronchus with a single arterial supply, which increases the risk of devascularization. 21 While these findings are derived from oncologic populations, trauma patients may experience similar risks, potentially compounded by acute blood loss and tissue hypoperfusion. 29
In our study, ECMO was used significantly more often in patients undergoing right-sided pneumonectomy, despite similar mortality compared with left-sided resections. This finding is notable given that ECMO is a highly selective intervention that has assumed an increasingly important role in trauma care in recent years.30,31 Interpretation of ECMO utilization should be approached cautiously, as its use is influenced by multiple factors, including physiological derangements, patient selection, and institutional practice patterns. 32 One study reported that although definitive indications for VV-ECMO in adult ARDS remain ill defined, its use in post-pneumonectomy ARDS may be reasonable in patients with an estimated mortality risk of approximately 80% from respiratory failure. 33 The higher frequency of ECMO after right-sided pneumonectomy may reflect the greater functional lung loss and abrupt increase in pulmonary vascular resistance associated with right-sided resections, predisposing patients to severe cardiopulmonary instability. A case report described a patient with penetrating trauma who required postoperative ECMO support due to the development of ARDS. 33 In this case report, ECMO was presented as a supportive modality that may help reduce mortality by providing temporary cardiopulmonary support during the period of physiologic adaptation following pneumonectomy. The authors further emphasized the importance of a multidisciplinary approach to minimize complications related to pneumonectomy, ECMO use, and prolonged hospitalization. Nevertheless, the role of ECMO in improving survival cannot be determined from this database analysis. Furthermore, our findings may be influenced by selection bias and institutional ECMO availability, as patients must survive the immediate perioperative period to be eligible for ECMO cannulation. Additionally, the TQIP data set lacks granular data regarding ECMO indications, timing of initiation, and duration of support, which limits interpretation. Prior studies have suggested that early ECMO initiation may improve outcomes in selected trauma populations. Henry et al reported lower in-hospital mortality among trauma patients with ARDS who received ECMO within seven days. 30 Overall, ECMO use in this cohort likely represents a marker of physiologic severity rather than a direct survival benefit, underscoring the need for future studies to reduce bias and better define patient selection, timing, and outcomes of ECMO following trauma pneumonectomy.
In our multivariable analysis, early pneumonectomy (within 6 hours) and low GCS (GCS <9) had higher odds ratio for in-hospital mortality (OR: 4.7 and 3.4, respectively). This aligns with a previous NTDB study which found patients with GCS <9 have higher odds of death. 6 The underlying rationale for rapid pneumonectomy is that uncontrolled intrathoracic hemorrhage from the pulmonary hilum is uniformly fatal, whereas a timely pneumonectomy performed in the appropriate clinical setting may be lifesaving. Although our study demonstrates higher mortality among patients undergoing pneumonectomy within 6 hours, this time window likely reflects the severity and extent of local injury rather than the timing of the operation itself. Importantly, comparisons of “rapid” pneumonectomy in prior studies often distinguish between immediate pneumonectomy and attempts at hemorrhage control before pneumonectomy, yet even patients who initially undergo hemorrhage control would likely fall within a 6-hour period. Another relevant consideration is whether lobectomy or wedge resection preceded pneumonectomy. In our analysis, prior lobectomy or wedge resection was not associated with worse survival, and pneumonectomy following these procedures was not identified as a negative prognostic factor. Therefore, the higher mortality observed with pneumonectomy within 6 hours should be interpreted in the context of injury severity and the clinical implications of early pneumonectomy, rather than timing alone.
There are several limitations to our study. First, the use of a retrospective database introduces potential misclassification, selection, and reporting biases, as coding errors may occur and access to certain technologies such as ECMO may vary. Second, the study period was limited by the implementation of the ICD-10 codes that identify pneumonectomy laterality, as previous ICD-9 codes do not capture the laterality of pneumonectomy, and TQIP only mandated ICD-10 reporting since October 2015. Third, given the overall rarity of trauma pneumonectomy, this also limits statistical power, particularly for secondary outcomes that occurred infrequently, such as ARDS (2.3%) and VAP (2.3%). Additionally, the database does not capture the cause of death, ECMO indications, or parameters on mechanical ventilator, which only allowed us to evaluate the association, not causal relationship between the laterality of pneumonectomy and patient outcomes. Early mortality observed in our study (31% within 6 hours) likely reflects injury severity and resuscitation-phase physiology rather than operative factors. Lastly, although logistic regression allowed adjustment for confounders such as early pneumonectomy and ECMO, unmeasured confounding factors may still exist due to the limitations inherent in a database study.
Conclusion
Our results suggest that in-hospital mortality in trauma patients is not influenced by the laterality of pneumonectomy. However, the indication for pneumonectomy should be carefully considered, particularly in patients with Glasgow Coma Scale<9 or those requiring the procedure within 6 hours of presentation. Future research should involve larger, prospective cohorts and clarify the role of ECMO in the management of trauma patients undergoing pneumonectomy.
Supplemental Material
Supplemental Material - Right-Sided Versus Left-Sided Pneumonectomy in Trauma: A Nationwide Analysis
Supplemental Material for Right-Sided Versus Left-Sided Pneumonectomy in Trauma: A Nationwide Analysis by Negar Nekooei, Delbrynth P. Smigel, C. Isabella Bent, Matthew J. Ashbrook, Kemp Anderson, Cameron A. Ghafil, Alberto Aiolfi, Takashi Harano, and Kenji Inaba, Kazuhide Matsushima in The American Surgeon™
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ashbrook is a lieutenant in the United States Navy, Medical Corps, Naval Medical Leader and Professional Development Command. This work was prepared as part of his official duties. Title 17, U.S.C., §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C., §101 defines a U.S. Government work as a work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. The views expressed in this manuscript reflect the results of research conducted by the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U.S. Government. No COI in all other authors.
Supplemental Material
Supplemental material for this article is available online.