
Abstract
Venothromboembolism (VTE) is rare in pediatric trauma but can have devastating consequences. While chemical prophylaxis guidelines exist in adult trauma, guidelines for pediatric populations are sparse. Adherence to the Eastern Association of the Surgery of Trauma (EAST) and Pediatric Trauma Society (PTS) guidelines is unclear. Our objective was to evaluate rate of VTE prophylaxis and adherence to current guidelines in our pediatric trauma population. Methods: We performed a retrospective cohort study at a single ACS-verified adult Level I/pediatric Level II Trauma Center from the years 2014-2024. Patients aged 7-18 were included. A subgroup based on the EAST/PTS guidelines. VTE prophylaxis, deep vein thrombosis (DVT) or pulmonary embolism (PE), injury severity score (ISS), and pubertal status. Results: During the study period, 1271 patients met inclusion criteria. Four patients (0.31%) experienced VTE. Three patients (0.24%) had a bleeding complication. While 787 patients met criteria for prophylaxis by EAST/PTS guidelines, only 279 patients (35.4%) received prophylaxis. Use of chemical prophylaxis increased after publication of EAST/PTS guidelines (20.6% vs 39.9%, p < 0.001). Of patients who qualified for chemical prophylaxis by the EAST/PTS guidelines, two patients (0.3%) developed VTE, while 1 (0.1%) developed a bleeding complication. One patient who developed a DVT was younger than 15 with an ISS <25 and did not meet criteria by EAST/PTS guidelines. Conclusion: Adherence to pediatric VTE prophylaxis guidelines increased over the study period without increase in adverse events. There was no difference in VTE incidence, but VTE was rare.
Key Takeaways
• Venothromboembolism (VTE) prophylaxis use was rare in this study for pediatric trauma patients. • VTE prophylaxis use increased after the publication of EAST/PTS guidelines. • VTE and major bleeding events were rare in the study population, 0.3% and 0.2%, respectively.
Background
Venothromboembolic events (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE) are well established causes of morbidity and mortality in the Trauma patient population. The rate of VTE is high in the adult population, and chemical prophylaxis has been consistently shown to be efficacious for the prevention of VTE.1,2 On the contrary, incidence of VTE is reported to be significantly lower in the pediatric trauma patient population, estimated to be less than 1%. 3 Older age has been reported as a risk factor for VTE in pediatric trauma patients. 4 While the incidence of VTE is significantly lower in the pediatric population, there are reports of rising rates of VTE in pediatric patients in general while hospitalized.3,5 Proposed risk factors for the development of VTE in pediatric trauma patients include obesity, prolonged immobilization, higher injury severity score (ISS), central venous catheter use, and major surgery, but the necessity and efficacy of VTE chemical prophylaxis in pediatric trauma has remained in question.6,7 Given the lower rates of VTE, there are few standardized guidelines for the use of DVT prophylaxis in the Pediatric trauma population.
In 2017, the Eastern Association for the Surgery of Trauma (EAST) and the Pediatric Trauma Society (PTS) created joint guidelines for the use of VTE prophylaxis in pediatric trauma patients. 8 After reviewing the data present at that time, the group recommended, albeit conditionally, chemical prophylaxis in trauma patients older than 15 years old and in younger postpubertal patients with an ISS greater than 25. Additionally, the group conditionally recommended against the use of chemical prophylaxis in children younger than 15 who were prepubertal, regardless of injury severity score.
In this study, we aim to evaluate the incidence of VTE and investigate use of VTE chemoprophylaxis in our pediatric trauma patient population at our mixed trauma center (Adult level I, Pediatric level II) before and after publication of the EAST/PTS guidelines. We hypothesize that use of chemoprophylaxis for the pediatric trauma population increased after publication of the guidelines.
Methods
Following exemption from the IRB, a retrospective case review of all pediatric patients who suffered traumatic injury was performed at an urban ACS-verified Adult Level 1/Pediatric Level 2 trauma center from November 2014 to June 2024. Patients were selected from the institutional trauma registry and included if they were admitted for 24 hours or more. Medical records were reviewed for patient demographics, ISS, deep vein thrombosis prophylaxis, management and outcomes.
Inclusion criteria consisted of patients who suffered trauma and were admitted to the hospital for management of their traumatic injury. Patients between the ages of 7 and 18 years old at the time of presentation were included. Exclusion criteria included age less than 7 years old, age older than 18 years old, and death within 24 hours of presentation.
Puberty status was defined using Tanner staging as stated explicitly on physical exam. Patients were classified as prepubertal when Tanner stage was equal to 1 and were classified as pubertal when Tanner stage was 2 or greater or if a history of menstruation was documented. Anticoagulation was classified as prophylactic or as therapeutic, depending on the dose and indicated reason for prescription. Intubation was defined as intubation outside of the need for intubation for a procedure or operation, unless the patient remained intubated postoperatively. Patients were admitted to either a primary Trauma Surgery Service or a Pediatric Medicine Service. Traumatic brain injury (TBI) was defined as moderate or severe traumatic brain injury, as defined by Glasgow Coma Scale and abnormal imaging. This did not include concussion or mild TBI. Spinal cord injury was defined as any injury to the spinal cord. Operation was defined as a surgical procedure requiring intubation. Orthopedic repair was defined as the operative repair of the pelvis or a long bone of the upper or lower extremity.
At this institution, there is no universal deep vein thrombosis (DVT) screening policy. Duplex ultrasound and computed tomographic angiography are only used diagnostically, when DVT or PE is suspected clinically.
The primary endpoint was venous thromboembolism (VTE), which included both DVT and pulmonary embolism (PE). The secondary endpoint was bleeding complication, which was defined as a clinically relevant bleeding event that required intervention, transfusion, or increased level of care.
A subgroup was created for analysis based on the guidelines created by EAST/PTS, consisting of patients who were either older than 15 years or patients younger than 15 years and postpubertal with an ISS greater than 25. Characteristics and outcomes were reviewed and compared among patients treated before and after the publication of the EAST/PTS guidelines.
Statistical Analysis
Group characteristics were compared using chi-square and Kruskal-Wallis tests. Categorical variable values are represented by (n, percentage, P-value). Continuous variable values are represented by (median, interquartile range, P-value).
Statistical analysis was completed on SPSS (SPSS Version 29, IBM).
Results
Demographics and Outcomes for All Patients n (%) Median (Interquartile Range)
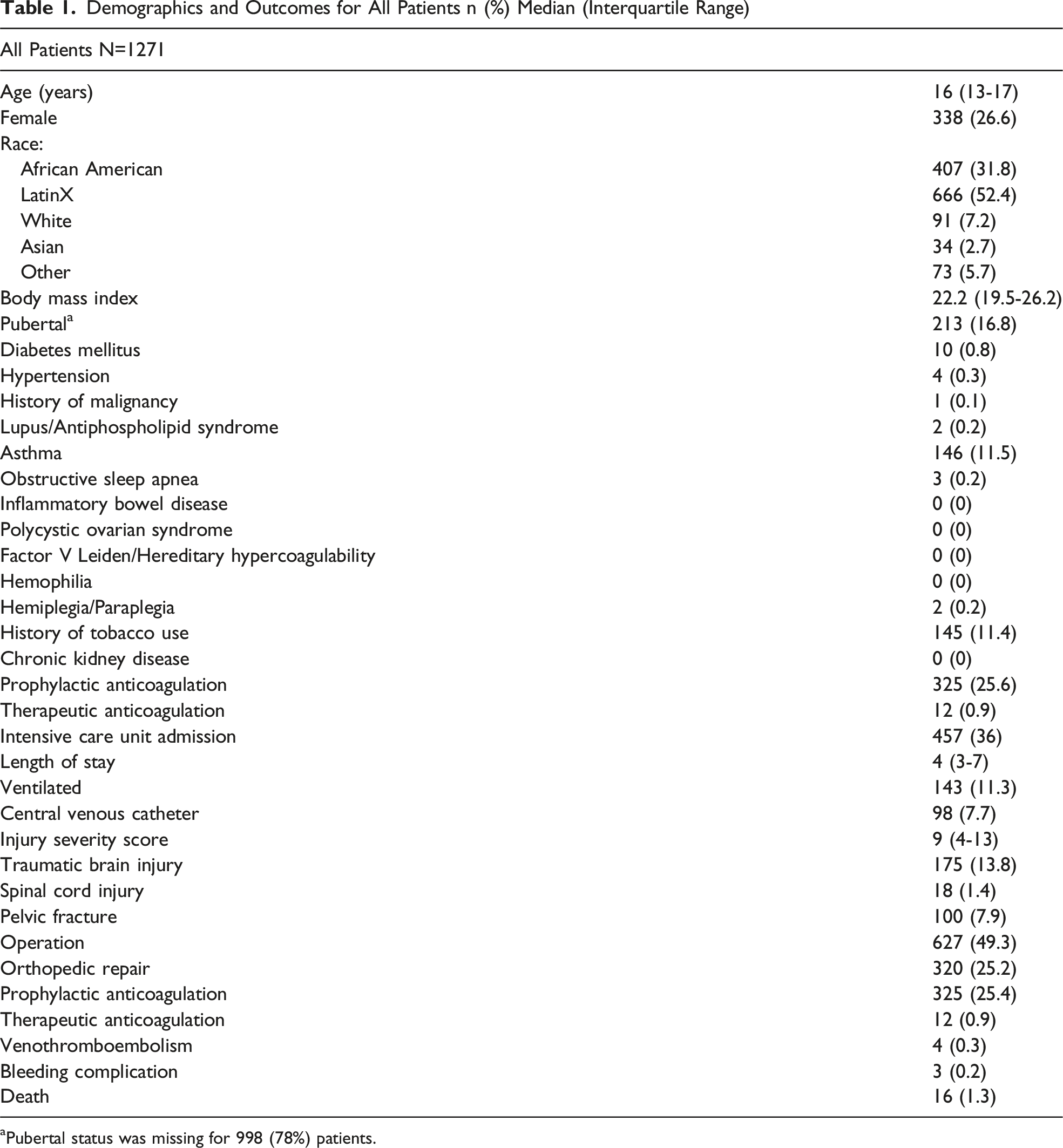
aPubertal status was missing for 998 (78%) patients.
Three patients (0.24%) experienced a bleeding complication. Two of these patients were on therapeutic anticoagulation, while the last was on prophylactic enoxaparin (Lovenox). There were 16 deaths (1.3%) total, and none were attributable to VTE or a bleeding complication.
Analysis of Subgroup by EAST/PTS Guidelines
Demographics and Outcomes for Patients that Qualified for Chemical Prophylaxis by EAST/PTS Guidelines. n (%) Median (Interquartile Range)
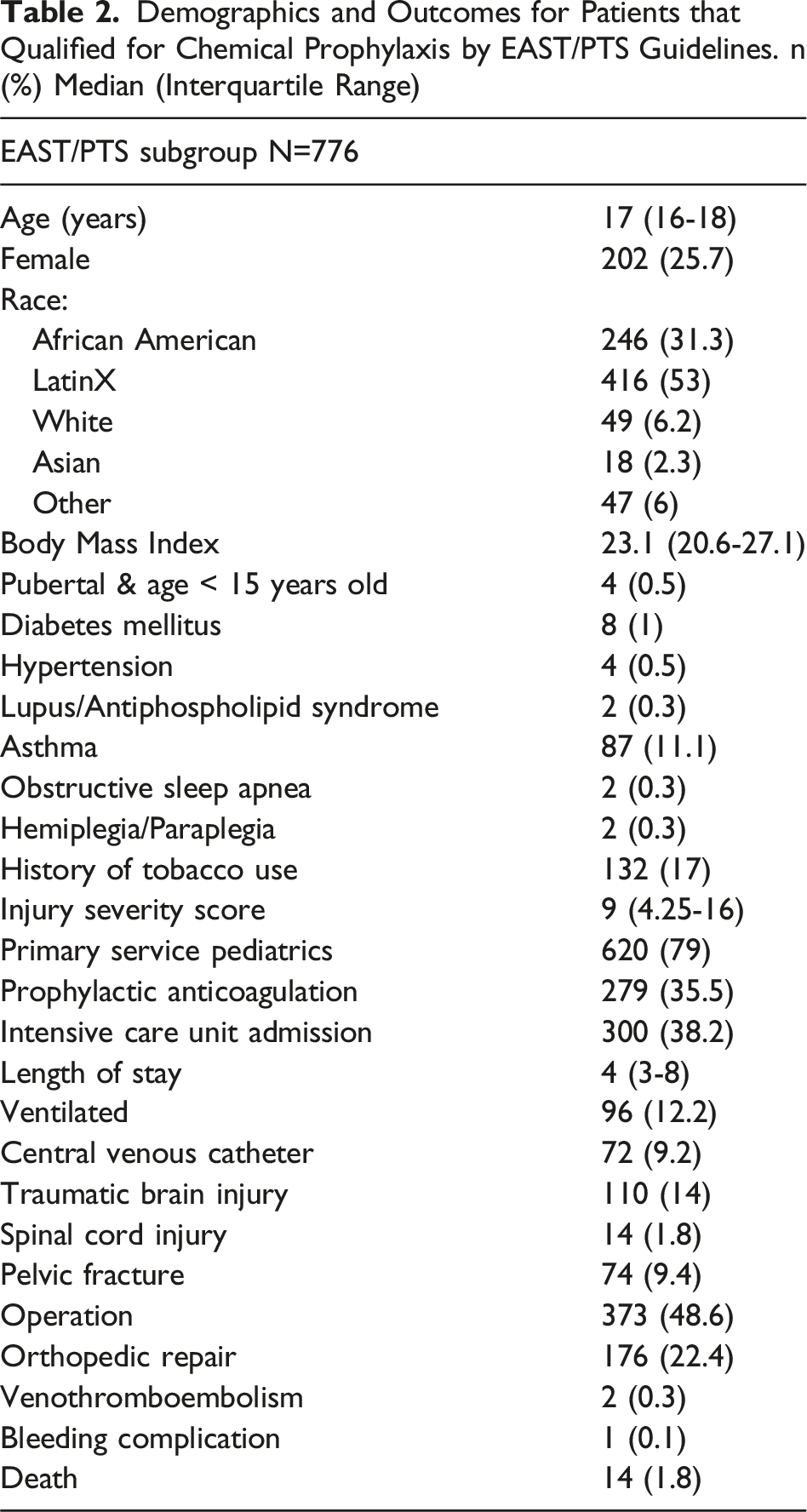
The pediatric team was the primary team for most of these patients, 620 patients in total (79%). Use of DVT prophylaxis was low among this subgroup (279, 35.4%) and was less common when Pediatric Medicine was the primary service as compared to Trauma Surgery (28.9% vs 61.4%, P < 0.001). Two patients developed a VTE, 0.3% of the subgroup. One patient was receiving chemical prophylaxis at the time of their diagnosis.
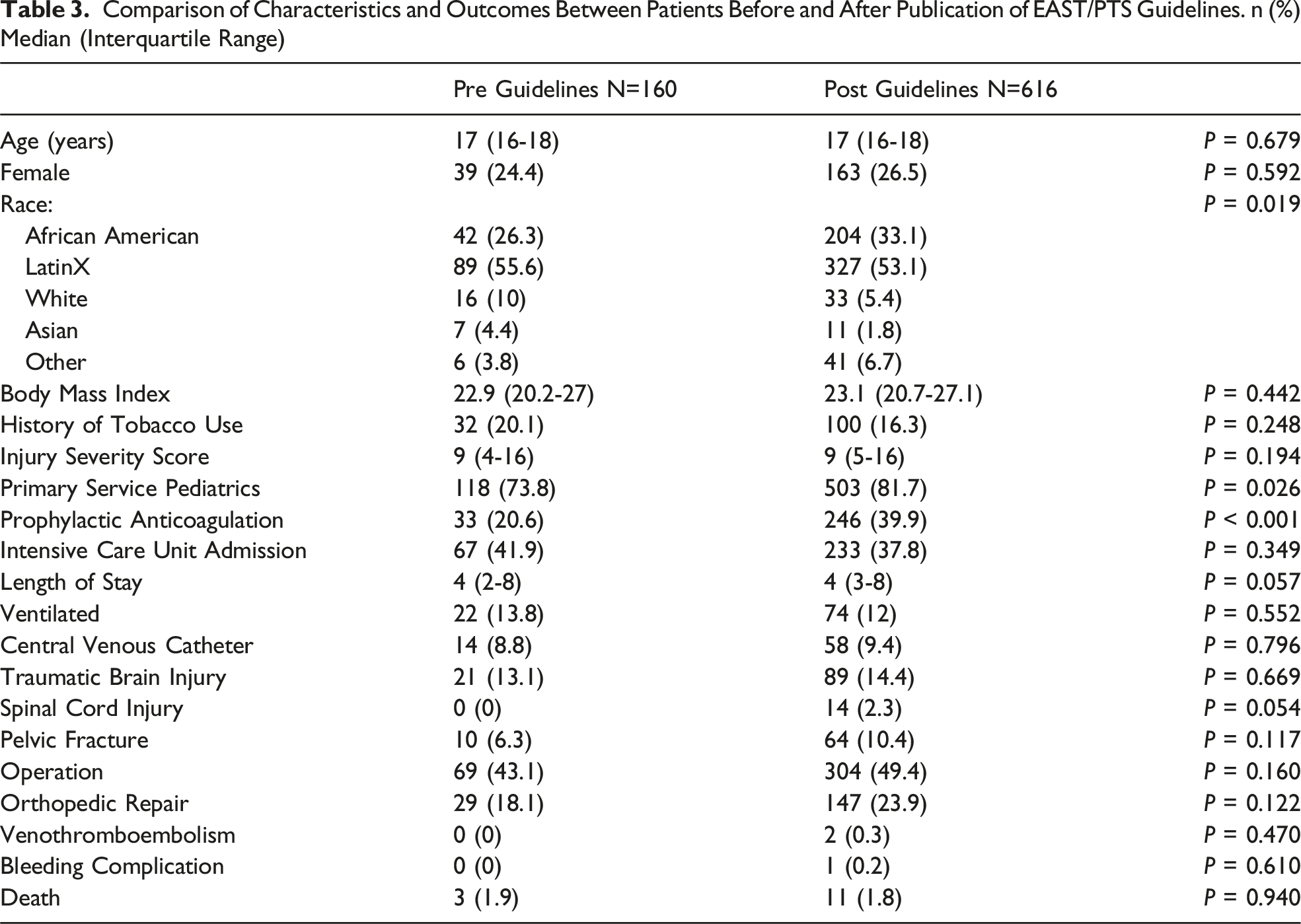
Comparison of Characteristics and Outcomes Between Patients Before and After Publication of EAST/PTS Guidelines. n (%) Median (Interquartile Range)
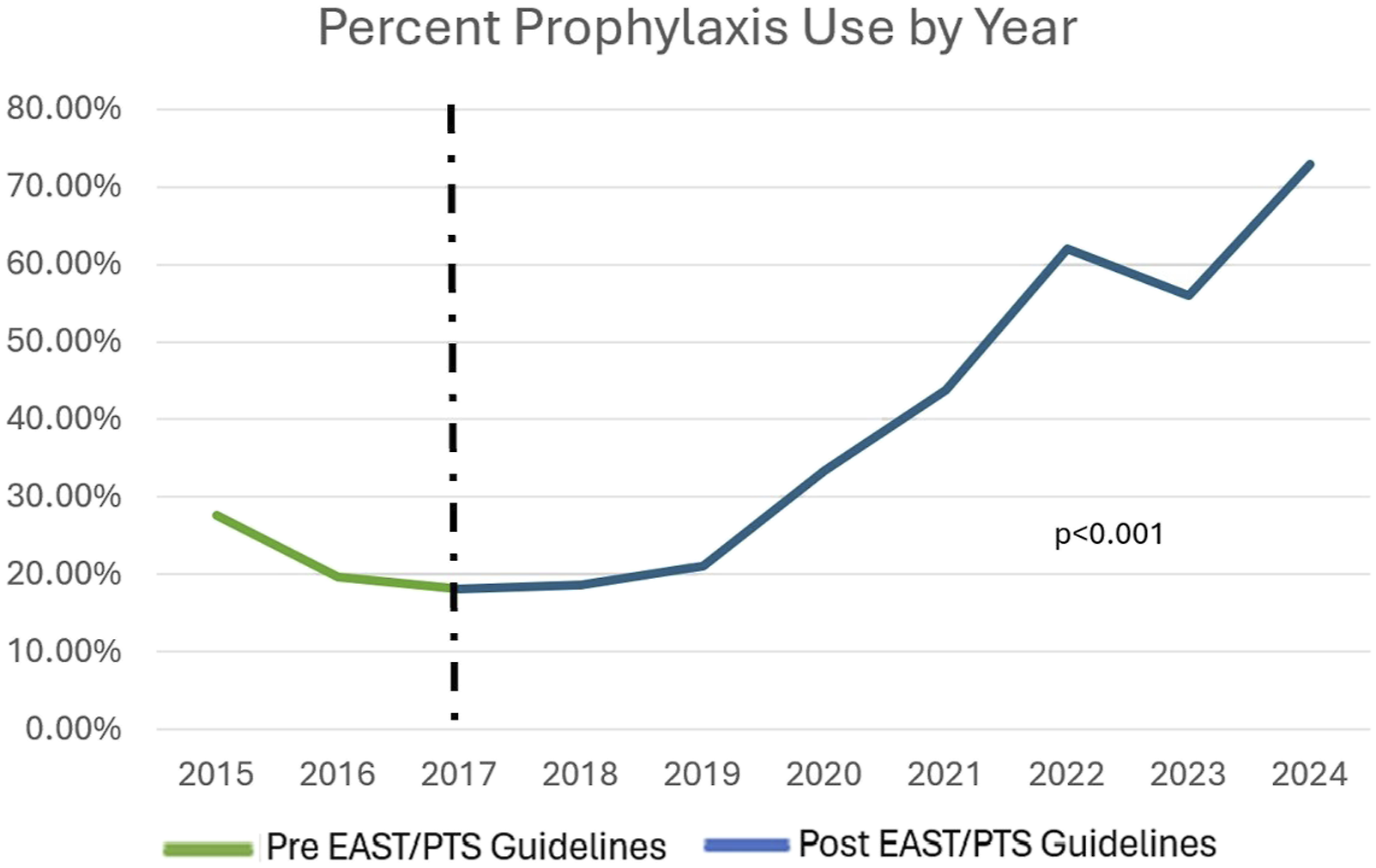
Rate of Chemoprophylaxis Use by Year. The use of VTE chemical prophylaxis increased significantly after publication of EAST/PTS guidelines
Discussion
In this study, the rate of VTE was low, 0.31% of the patients studied. The rate of bleeding complication was similarly low (0.2%), paralleling a previous study that found that adolescent trauma patients treated with chemical VTE prophylaxis failed nonoperative management of blunt solid organ injuries at a similar rate to those without chemical prophylaxis. 7 Rates remained low even when patients were selected by EAST/PTS chemoprophylaxis guidelines. Of note, one DVT occurred in a patient who did not meet EAST/PTS guidelines for prophylaxis.
Chemoprophylaxis use within the subgroup of individuals that met EAST/PTS criteria was low (35.4%) and resembles similar studies of the pediatric trauma population. In a study by Cyprich et al, Pediatric Trauma Centers were less likely to use chemoprophylaxis (5.0%) as compared to Mixed (24.9%) and Adult Trauma Centers (51.0%). 9 In our study, the patients cared for primarily by the Pediatric Medicine service were significantly less likely to receive chemoprophylaxis. This may be due to a difference in the triage and navigation of primary service in this study’s hospital, as the Trauma service tended to take primary on older patients with higher ISS, but may indicate significant practice differences between the two services. Notably, the rate of prophylaxis in our study increased significantly when comparing rates prior to publication of the EAST/PTS guidelines to after. It is also important to note that the Pediatric Medicine service was primary significantly more often after guideline publication, signaling a possible shift in practice patterns and evolving multidisciplinary care of the pediatric trauma patient. It is unclear the cause behind the increased rate of chemoprophylaxis in this study and may be due to adherence to guidelines, though a survey study by Cunningham et al in 2020 showed that application of the EAST/PTS guidelines was low amongst all responders from Pediatric, Mixed, and Adult Trauma Centers. 10
This study was limited by a small, single institution population. Its limitations primarily stemmed from the infrequent occurrence of VTE and bleeding complications. Additionally, medical records were unable to provide the method of dosing chemoprophylaxis, missed doses of anticoagulation, use of mechanical prophylaxis, and level of ambulation. The second condition of the EAST/PTS guidelines potentially highlighted a high-risk subgroup of the pediatric trauma population of patients younger than 15 years old, but who were significantly injured and postpubertal. We found documentation around pubertal development lacking, suggesting a possible barrier to real world use of this portion of the guidelines.
Debate continues around the use of chemoprophylaxis in the pediatric trauma population. The incidence is so low as to potentially argue against similar use as in the adult population. This study adds to previous research, showing that chemical VTE prophylaxis is safe in the pediatric trauma population. Further research is needed to isolate the high-risk subgroup that would benefit from prophylactic anticoagulation.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.