
Abstract
Perforated peptic ulcers are surgical emergencies typically treated by omental patch repair. This report describes the first successful pedicled gallbladder flap for duodenal perforation repair in the setting of inadequate patch material. A previously healthy 28-year-old male was taken emergently for surgery after presenting with intra-abdominal sepsis in the setting of rapid, unintentional weight loss. Findings of feculent peritonitis and multiple colonic perforations were managed with a subtotal colectomy and temporary abdominal closure. At re-exploration, a perforated duodenal ulcer was identified. The patient’s critical status and absent omentum, insufficient falciform ligament, and friable small bowel precluded traditional repair options. A pedicled gallbladder flap was fashioned instead, with the patient experiencing a successful recovery. He was discharged within a month, tolerating an oral diet and free of surgical drains. The use of a pedicled gallbladder flap to seal a duodenal perforation is a potentially viable approach rooted in existing animal models. Further research is warranted.
Keywords
Background
Peptic ulcer disease (PUD) comprises a spectrum of foregut pathologies, ranging from superficial mucosal erosion to full-thickness perforation. Perforated PUD is a surgical emergency that often necessitates operative intervention, with most simple perforations effectively managed by primary repair or omental patch closure. 1 When omental tissue is unavailable or inadequate, alternative materials such as the falciform ligament or small bowel serosa may be employed. In cases of extensive duodenal injury or hemodynamic instability, a damage control strategy may be required. This report presents the first successful human case of a duodenal ulcer perforation repair using a novel technique: the pedicled gallbladder flap.
Case Description
A previously healthy 28-year-old male presented with severe abdominal pain and rapid, unintentional weight loss. On presentation, he was found to be cachectic, septic, and diffusely peritonitic. He was taken for an emergent exploratory laparotomy where the index surgeon encountered extensive intra-abdominal contamination and multiple abscesses. Findings of multiple colonic perforations in a hemodynamically compromised patient prompted a subtotal colectomy followed by damage control temporary abdominal closure.
After a period of resuscitation in the intensive care unit (ICU), the patient returned to the operating room (by WSL) for a second look laparotomy, during which an undrained right upper quadrant bilious abscess and a 1.5 cm anterior duodenal perforation were identified (Figure 1). At that point, the omentum was surgically absent, the falciform ligament was diminutive, and the small bowel was severely edematous, matted, and friable. The patient remained on significant vasoactive support and was deemed unfit for prolonged surgery. Standard anatomic configuration of the right upper abdomen, with location of the perforated duodenal ulcer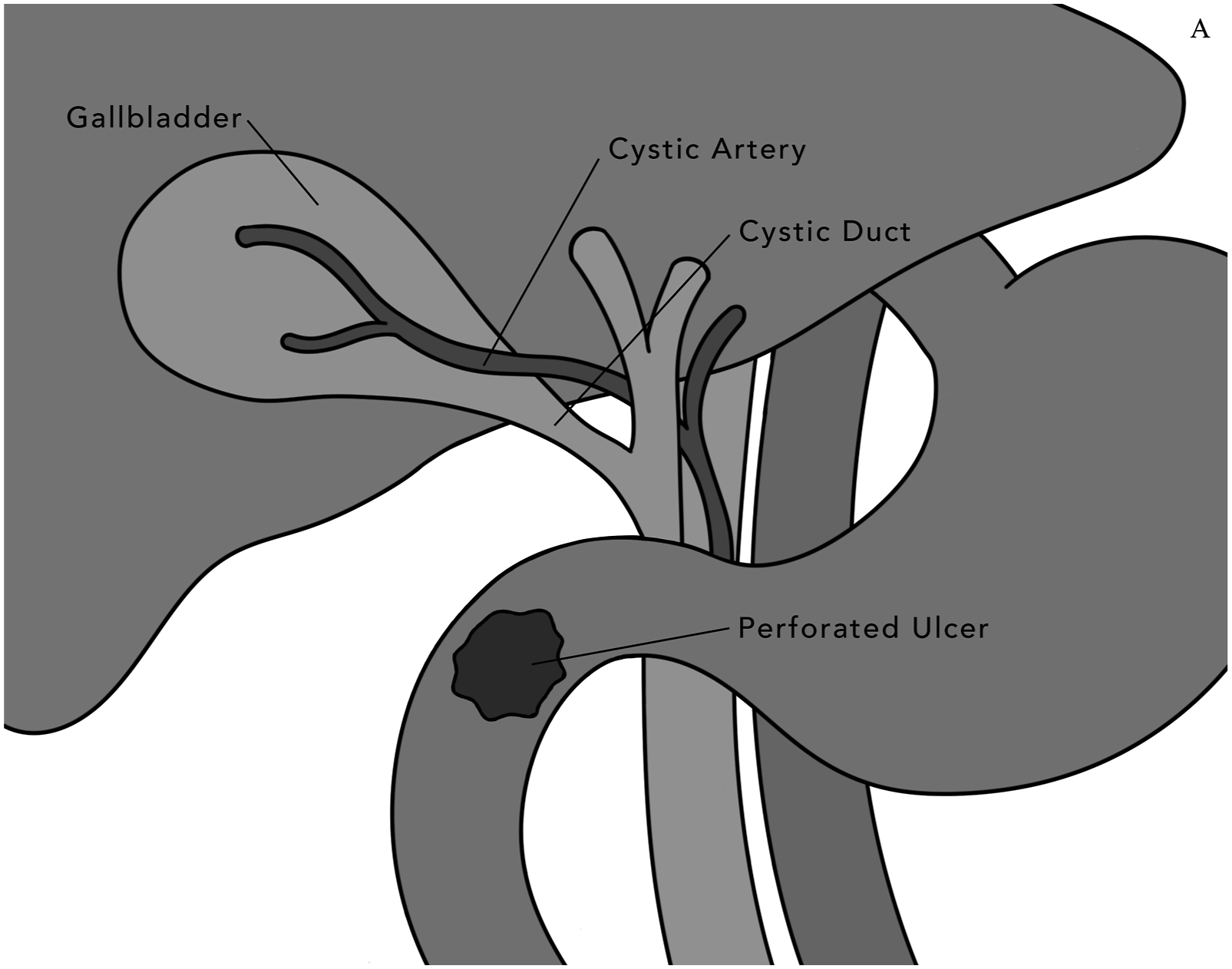
The gallbladder was then dissected off the cystic plate in a top-down fashion, leaving the cystic artery and duct intact. It was mobilized to cover the duodenal perforation without tension or angulation and circumferentially sewn to the perforation edges using full thickness, interrupted, non-absorbable, 3-0 monofilament sutures (Figure 2). Two surgical drains were left. An end ileostomy was matured and the abdomen closed. Schematic illustration of the pedicle gallbladder visceral patch repair of a perforated duodenal ulcer. Final configuration following completion of gallbladder serosal patch, illustrating covered defect (dashed) along with suture placement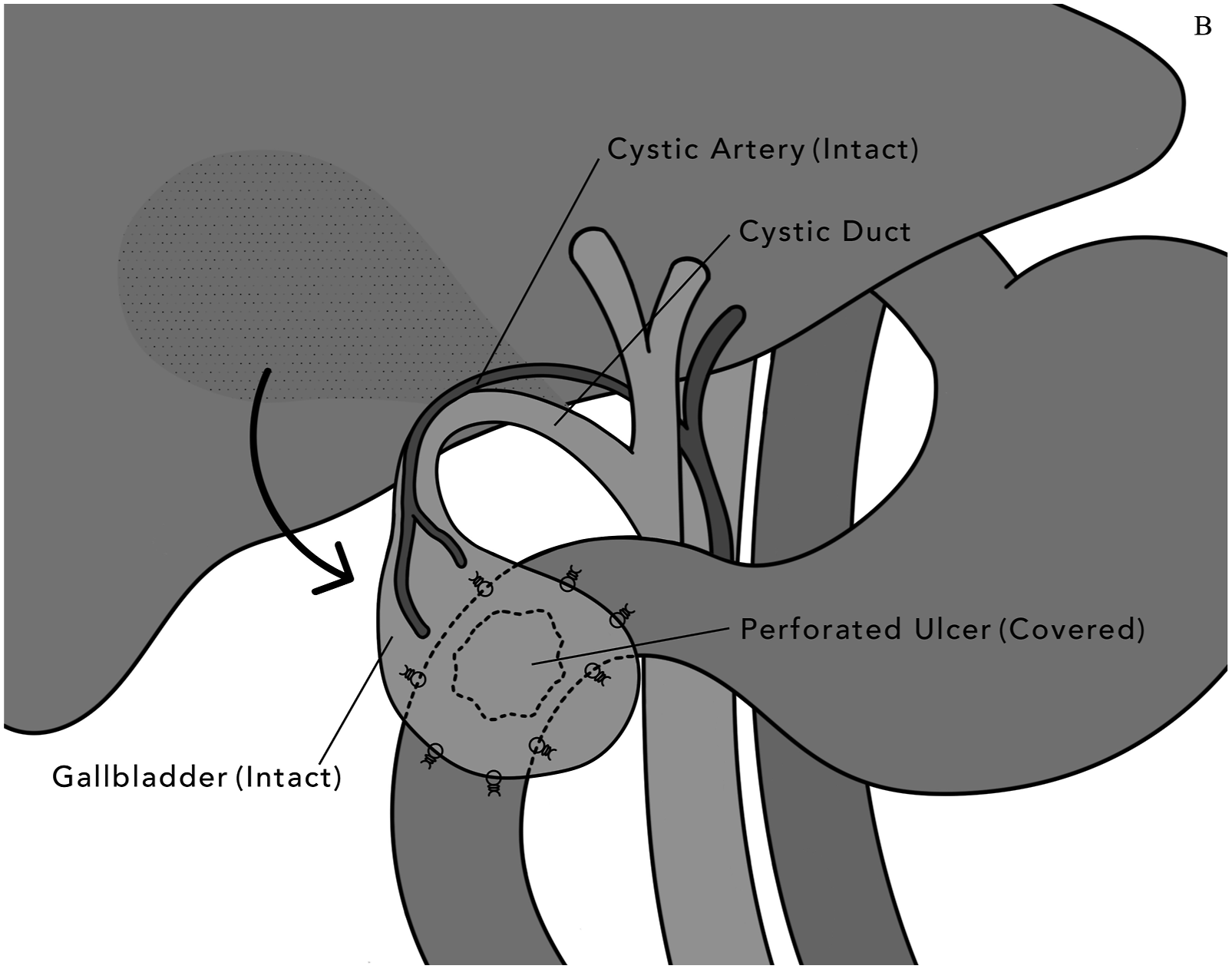
Final pathology report revealed Crohn’s disease. The patient was weaned off all vasoactive agents by postoperative day (POD) 1. He was extubated on POD 4 and discharged from the ICU on POD 6. An initial upper gastrointestinal series (UGIS) was performed, demonstrating no active extravasation of contrast. However, delayed images revealed a subtle curvilinear density in the right upper quadrant and trace amount of extraluminal contrast could not be definitively excluded. As he had been clinically well and afebrile, with low volume and generally serosanguinous drain outputs, a decision was made to maintain the patient nil per os out of an abundance of caution. Nutritional support was provided via a gastrostomy tube with jejunal extension and parenteral nutrition (PN).
His hospitalization was otherwise largely uneventful except for physical deconditioning addressed by rigorous physical therapy, a left upper quadrant intra-abdominal abscess drained percutaneously, and a superficial surgical site infection treated by standard wound care. On POD 16, a repeat UGIS confirmed no contrast extravasation. On POD 23, he was tolerating an oral diet, had all surgical drains removed, and was discharged from the hospital. At his 1-month follow-up, he had met all his nutritional goals and was gaining weight by oral intake alone. His gastrostomy tube was removed, and he was referred to gastroenterology for continued care.
Discussion
The omental patch, a well-established technique for the management of duodenal perforations, may not be feasible in patients lacking adequate omentum due to previous resection or malnutrition. Alternatives include the use of the falciform ligament or the small bowel serosal patch, gastroduodenal resections, and wide drainage procedures. Foregut resections are technically demanding, time-consuming procedures generally unsuitable for hemodynamically compromised patients. 1 The combination of wide drainage and decompressive duodenostomy, with or without pyloric exclusion, is typically reserved for major duodenal injuries not amenable to repair or resection and aims to convert a free perforation into a controlled fistula. However, it is associated with significant morbidities such as the need to manage multiple drains and prolonged reliance on tube feeding and/or PN. The comparative effectiveness of these techniques remains poorly defined. 2
In our case, standard repairs were not feasible due to absent omentum and a diminutive falciform ligament. The small bowel integrity was questionable due to its edematous, friable, and densely adherent nature. Additionally, the ultimate diagnosis of Crohn’s disease further validated the decision to avoid unnecessary bowel manipulation. All these factors, combined with a critically ill patient, would have traditionally favored the use of a wide drainage procedure.
In this case, the gallbladder, palpably free of stones, was the only relatively healthy, serosalized tissue in close proximity to the duodenal defect, making it a suitable candidate for the construction of a pedicled flap. A top-down dissection was performed with careful attention to maintaining the correct tissue plane in order to avoid both bleeding from the liver and perforation of the gallbladder, the latter of which would have necessitated a primary repair. Dissection proceeded until the cystic triangle was freely mobile, but without dissecting or isolating the cystic duct or artery, effectively creating a gallbladder flap on a vascularized pedicle.
The flap was then positioned serosal side down onto the duodenal defect, taking care to avoid any acute angulation or tension. Had the flap been deemed unsuitable at this stage, a completion cholecystectomy would have been performed and the organ discarded before proceeding with an alternative ulcer management strategy. As the flap was satisfactory, it was sutured circumferentially to the healthy margins of the duodenal defect, beginning with an anchoring stitch at the far corner, near the gallbladder neck. Full-thickness or seromuscular bites were taken in healthy tissue on both the gallbladder and the duodenum. Kocherization of the duodenum can be considered to improve exposure, though this was not required in this case.
The positive clinical outcome that the patient experienced is encouraging as, to the authors’ knowledge, this is the first documented pedicled gallbladder patch of a perforated duodenal ulcer in humans. Previously, its feasibility has been demonstrated in several animal studies.3–5 Notably, Hosseini et al. used eight dogs with surgically created duodenotomies as their subjects. Half of the group was repaired using an exposed gallbladder mucosal patch (created by ligating the cystic duct, opening the gallbladder fundus, and then covering the duodenal defect with the exposed gallbladder mucosa) and the other half using an intact gallbladder serosal patch. Both groups reported excellent outcomes though, interestingly, histological analysis revealed complete healing (i.e., re-epithelialization of the duodenal defect) only in the serosal patch group. In contrast, the mucosal patch group demonstrated mucosal undergrowth resulting in partial patch separation. These findings suggest a histopathologic rationale favoring the use of the serosal surface, concordant with the technique utilized in our report. Ultimately, caution is warranted when extrapolating results from limited animal studies.
The clinical outcome observed in our experimental pedicled gallbladder flap repair suggests that this technique, while not yet validated in humans, could be considered for further study as a potential option of last resort in select salvage scenarios where conventional approaches are not feasible. Its theoretical advantages include the fact that the gallbladder provides a well-vascularized tissue surface and lies in close proximity to the duodenum. Its use would also avoid the need for small bowel manipulation in a potentially hostile abdomen.
However, this novel and unproven technique is not without significant risk. Dissection of the gallbladder in a hostile abdomen introduces the potential for biliary tree injury, compounding an already challenging clinical scenario. The most consequential long-term concern is the development of acute cholecystitis or other biliary pathology. Should this occur, the greatest danger would stem from an attempted cholecystectomy performed without a clear understanding of the patient’s altered anatomy, with the potential of recreating a large duodenal defect and all its attendant complications. To mitigate this risk, we emphasized the patient’s unique anatomy repeatedly throughout his medical records. Furthermore, we explicitly instructed the patient and his family to alert future surgeons to review these materials prior to any abdominal surgeries.
If such a patient were to present with acute cholecystitis, the safest operative strategy would likely be a subtotal cholecystectomy that preserves the cystic artery and duodenal portion of the gallbladder, which should have theoretically re-epithelialized and developed its own blood supply over time. An alternative strategy, relatively novel in its own right, would be the creation of an endoscopic ultrasound-guided cholecystoduodenostomy with stent placement to provide internal drainage, an approach theoretically facilitated by the direct surgical apposition of the gallbladder to the duodenum. To mitigate the risk of iatrogenic gallstone ileus, this strategy should be undertaken with caution in patients harboring sizeable gallstones. A recent systematic review and meta-analysis by Canakis et al. evaluating outcomes of endoscopic gallbladder drainage demonstrated high technical and clinical success rates (95.8% and 94.3%, respectively). 6 Reported complications, including recurrence of cholecystitis (4.2%) and need for reintervention at 1 year (6.0%), were relatively infrequent. However, the long-term effectiveness and durability of this treatment modality remain under evaluation. Ultimately, caution and sound clinical judgment are warranted when combining multiple novel therapeutic strategies, as such approaches may carry the risk of unforeseen and potentially catastrophic consequences. Consultation with a hepatopancreatobiliary surgeon, a surgeon experienced in complex duodenal and biliary anatomy, or an advanced gastrointestinal endoscopist is strongly advised.
Conclusion
The surgical treatment of a perforated duodenal ulcer is classically managed using a primary repair or omental (Graham) patch technique. In response to the absence of viable patch material in a critically ill patient with a hostile abdomen, we performed the first successful human pedicled gallbladder serosal patch repair of a duodenal perforation, achieving positive clinical outcomes. Further systematic evaluation of this technique is needed to delineate safety, efficacy, and long-term outcomes.
Lessons Learned
• Routinely evaluate the duodenum during surgical exploration for peritonitis, as perforated peptic ulcers may be overlooked in contaminated fields. • Preserve as much omentum as feasible to maintain its availability for future surgeries. • Consider surgical enteric access at the index operation (such as a surgical gastrostomy or jejunostomy) when prolonged nil per os status is anticipated. • Review established techniques for addressing perforated peptic ulcers (such as primary repair, omental patch, traditional serosal patch, resection, and wide drainage procedure) and their indications. • Acknowledge the highly experimental nature of a pedicled gallbladder serosal patch, even as a last-resort option. Although animal and histologic models suggest potential viability, human experience is limited, and careful clinical judgment must be exercised. • When fashioning the gallbladder into a pedicled flap, employ a top-down dissection while preserving its structural integrity and vascular supply. The flap should be circumferentially sutured onto the duodenal defect without acute angulation or undue tension. • Recognize the potential for future complications (such as cholecystitis and other biliary pathologies) in the setting of altered anatomy and the lack of established diagnostic or therapeutic strategies for managing such issues.
Footnotes
Acknowledgment
We express our gratitude to Katarina Miles, medical illustrator, for her work on the original technical illustrations and figures.
Ethical Considerations
Per UNC-Chapel Hill policy (OHRE SOP 2501), this single-patient case report did not require formal IRB review.
Consent to Participate
Written informed consent was obtained from the patient for publication of this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed. Data sharing is not applicable.