
Abstract
Background
Junior residents are not uniformly prepared for, trained in, or comfortable with their roles as teachers. There are few feasible and reproducible published curricula to address that gap and no such curriculum that targets the specific needs of junior surgical residents. We designed and implemented a course for junior residents-as-teachers with the aim of studying the impact on residents’ comfort, confidence, perceptions, and behaviors as well as proving the feasibility and reproducibility of the curriculum.
Methods
Using Kern's model of curriculum development, we designed and implemented a didactic and workshop-based course. The curriculum content focused on the learning climate, expectation setting, teaching, and giving feedback. The course was offered to PGY-1 and PGY-2 general surgery residents at a university-based program over two separate years. The course was evaluated with a retrospective pre/post-survey assessing change in self-reported comfort, confidence, perceptions, and behaviors. Improvement was analyzed using a student’s t-test (1-sided, P < 0.05 as significant).
Results
The course had >90% participation (26 of 30 residents). Statistically significant increases (P < 0.01) were seen in self-reported comfort, confidence, and time spent on expectation setting, teaching, giving feedback, and role-modeling. After the curriculum, participants believed to a greater extent (P = 0.01) that being a skilled teacher as a resident is important. All respondents supported offering the course to future trainees.
Discussion
This junior residents-as-teachers course significantly improved self-reported comfort, confidence, and time spent on teaching activities. The course was feasible even within the constraints of a surgical-training program and was proven reproducible through a second pilot.
Key Takeaways
• A feasible, reproducible, and effective residents-as-teachers curriculum for junior surgical residents is important in achieving the ACGME and LCME missions for resident teachers. • This curriculum improved resident perceptions of the importance of teaching, increased and enhanced resident teaching, and improved residents’ comfort and confidence as teachers.
Introduction
A medical student’s training on a clerkship, unlike the formal curriculum of pre-clerkship education, is derived from informal and even unintended curricula. 1 The actual curriculum depends on the people and situations that the clerk encounters. This model of learning is best described by the “social learning theory” in which a learner ascribes meaning to content via context, observations, and collaborations. 1 Resident trainees are central to this model and are perceived as the most influential teachers with whom a clerk interacts.2,3 Therefore, the way in which residents behave, respond to situations, and interact with their students is a crucial portion of the medical school curricula.
The teaching environment in surgery includes unique challenges that augment the value of the resident teacher. For medical students, the surgical clerkship, compared to other specialties, offers substantially less time for organized didactics. 2 With fewer scheduled conferences, a considerable amount of learning takes place in unstructured settings such as the OR. 2 That learning varies widely between clerks and often on the basis of the clerks’ assigned resident team. 2 For surgery residents themselves, given the time constraints of their training program, little attention is devoted in the resident curriculum to developing and honing skills in teaching and assessment. Unsurprisingly, surgery residents describe their greatest challenges to teaching as lacking both teacher training and having limited time to teach due to competing responsibilities. 4
The Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Surgery acknowledge the importance of teaching and include teaching as a milestone for surgery residents. Level four of this practice domain reads, “…The resident is a highly effective teacher with an interactive educational style and engages in constructive educational dialogue….” 5 Similarly, the Liaison Committee on Medical Education (LCME) outlines in its educational directive that residents should be trained to teach and should be evaluated on their competence in teaching. 6 Unfortunately, despite that guidance, residents are asked and assumed to do a job for which they have insufficient preparation. 7 As of 2017, only 43% of surgery programs provided residents-as-teachers instruction, making surgery the least likely of any specialty to provide a residents-as-teachers course. 8 In 2019, a review of all published general surgery residents-as-teachers curricula found only three curricula published since 2010, and two of those were e-mail-based without an in-person or experiential component. 9 Since that review was published in 2019, 9 a handful of additional single-institution curricula have been published that demonstrate improvement and positive impact.10-12 One study of a published 4-hour workshop noted that confidence was preserved at one year, but knowledge was not preserved. 13 That result suggests that the attitudes toward teaching were durable, but the content and acquired skills were not. There is a need for an easily reproducible curriculum for planned repetition.
Over the last many decades, multiple needs assessments3,4,10 and curricula have been developed to improve resident teacher training across specialties.10-27 Few of them, however, are directed at surgical residents and even fewer target the specific needs of junior surgical residents. Junior residents are both the most novice in their medical training and the least experienced in their roles as educators. The needs of junior residents in teacher training differ from those of more senior residents who more often teach in their leadership roles and in the operating room. Most importantly, few published curricula for surgical residents-as-teachers prioritize the feasibility of the course, such that the course can be easily reproduced each year.
Published needs assessments on resident teaching suggest that residents would benefit from a greater understanding of their roles as educators, guidance on time-efficient teaching techniques, lessons in clear communication and expectation setting, and honing skills in teaching.4,17 Those aims were corroborated by a 2019 consensus guideline from experts in medical education who outlined their approach to residents-as-teachers programs. 16 We therefore designed an interactive curriculum based on those aims.
In this study, we developed a curriculum for junior surgical residents-as-teachers aiming to increase resident comfort, confidence, and practice across teaching skills. We sought to create a curriculum that was feasible and easily reproducible accounting for the many competing demands on resident time. Finally, we assessed the impact of this curriculum given twice over two years by creating a new self-assessment tool.
Methods
This study was deemed exempt from the Institutional Review Board. The junior resident-as-teachers curriculum was designed following Kern’s et al 19 6-step approach:
Step 1: Problem Identification and General Needs Assessments
Residents are not uniformly equipped with fundamental teaching skills. Often, the ability to teach is assumed and additional skills are gained via observation, which is insufficient to produce doctors who are adept educators. Specifically, junior residents, who are newest to being doctors and have the least experience in supervising and guiding medical students, need training in their roles as educators. A scoping literature review demonstrated no such curriculum targeted to the junior surgery resident.
Step 2: Targeted Needs Assessment
Four main areas of need were identified: (1) Communication and expectation setting, (2) the learning climate, (3) skills in teaching, and (4) giving feedback. Those areas were each considered within the practical context of surgical training.
Step 3: Goals and Objectives
The aims of this curriculum were for residents to gain comfort and confidence in teaching, to increase their teaching practices, and to perceive that being a skilled teacher was an important goal of their training program. To this end, we used a deliberative curriculum framework
24
and developed measurable objectives for the curriculum: 1. Residents will gain comfort and confidence in their roles as educators. 2. Residents will gain comfort in teaching, setting expectations, and giving feedback. 3. Residents will gain confidence in teaching, setting expectations, and giving feedback. 4. Residents will increase the amount of time they spend teaching. 5. Residents will increase the frequency with which they set expectations for their learners. 6. Residents will perceive that becoming a skilled teacher is a goal of their training program and one toward which they should work.
Step 4: Educational Strategies
We utilized a deliberate practice model
21
to design a curriculum that uses instructional methods such as discussion, reflection, role modeling, role playing, and self-reviews for a learner-centered approach.21,22 Residents started the course by reflecting on their own good and bad experiences with teaching. They were then taught teaching techniques, concepts about the learning climate, and tools for giving feedback. Finally, they completed the curriculum by practicing both teaching and giving feedback. The content of the curriculum is derived from the Stanford Faculty Development Course on Clinical Teaching
25
and includes the following: 1. Communication and expectation setting: introductions; the explicit setting of expectations; identifying goals; how to prepare; how to optimize role-modeling. 2. The learning climate: teacher enthusiasm; learner involvement; respect and comfort by using a learners’ name and by inviting opinions; acknowledging common problems faced by learners; admitting one’s own limitations. 3. Skills in teaching: organizing material by using overviews, summaries, enumeration, and advanced organizers; clarifying content; emphasizing important points via repetition and visual aids; fostering active learning by encouraging notetaking, reflection, and skill practice. 4. Giving feedback: the ADAPT model described in the ACGME clinical competency guidebook consists of four distinct parts: Asking the learner for self-reflection and assessment; Discussing points of the learners’ strength and weakness; having the learner Ask for clarity; Planning together for steps toward improvement.
26
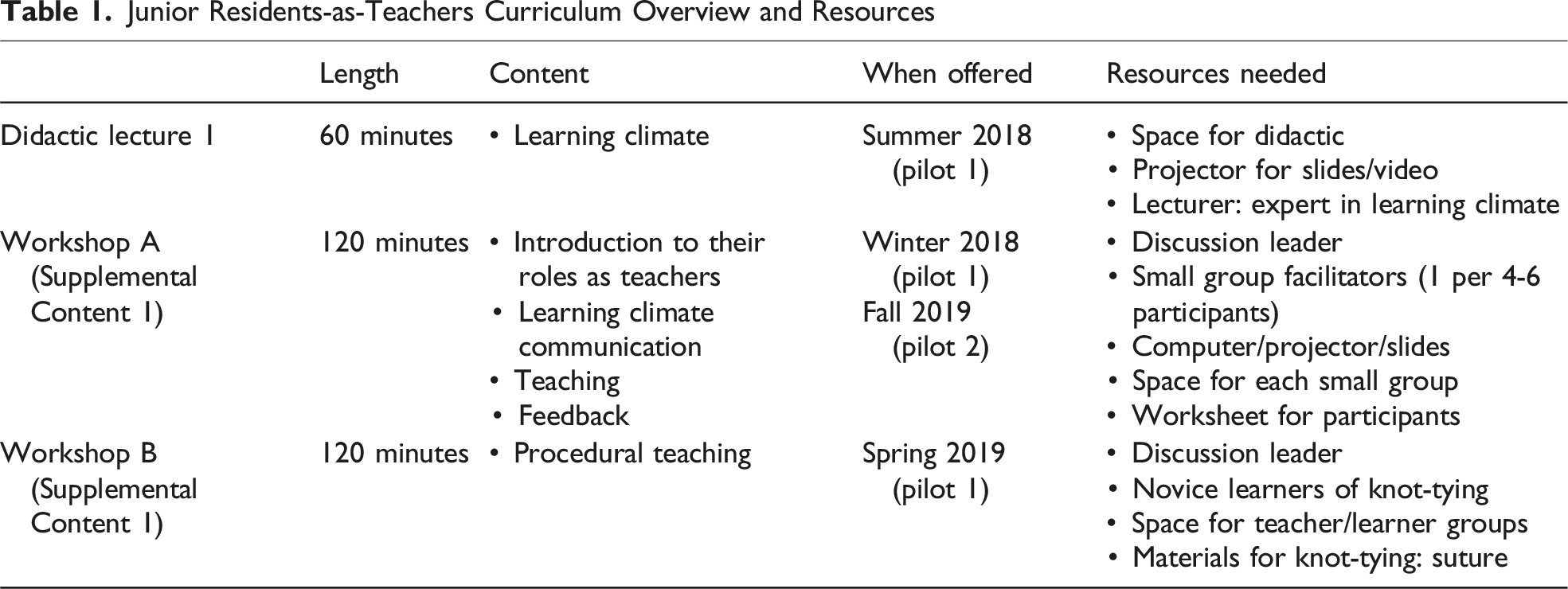
Junior Residents-as-Teachers Curriculum Overview and Resources
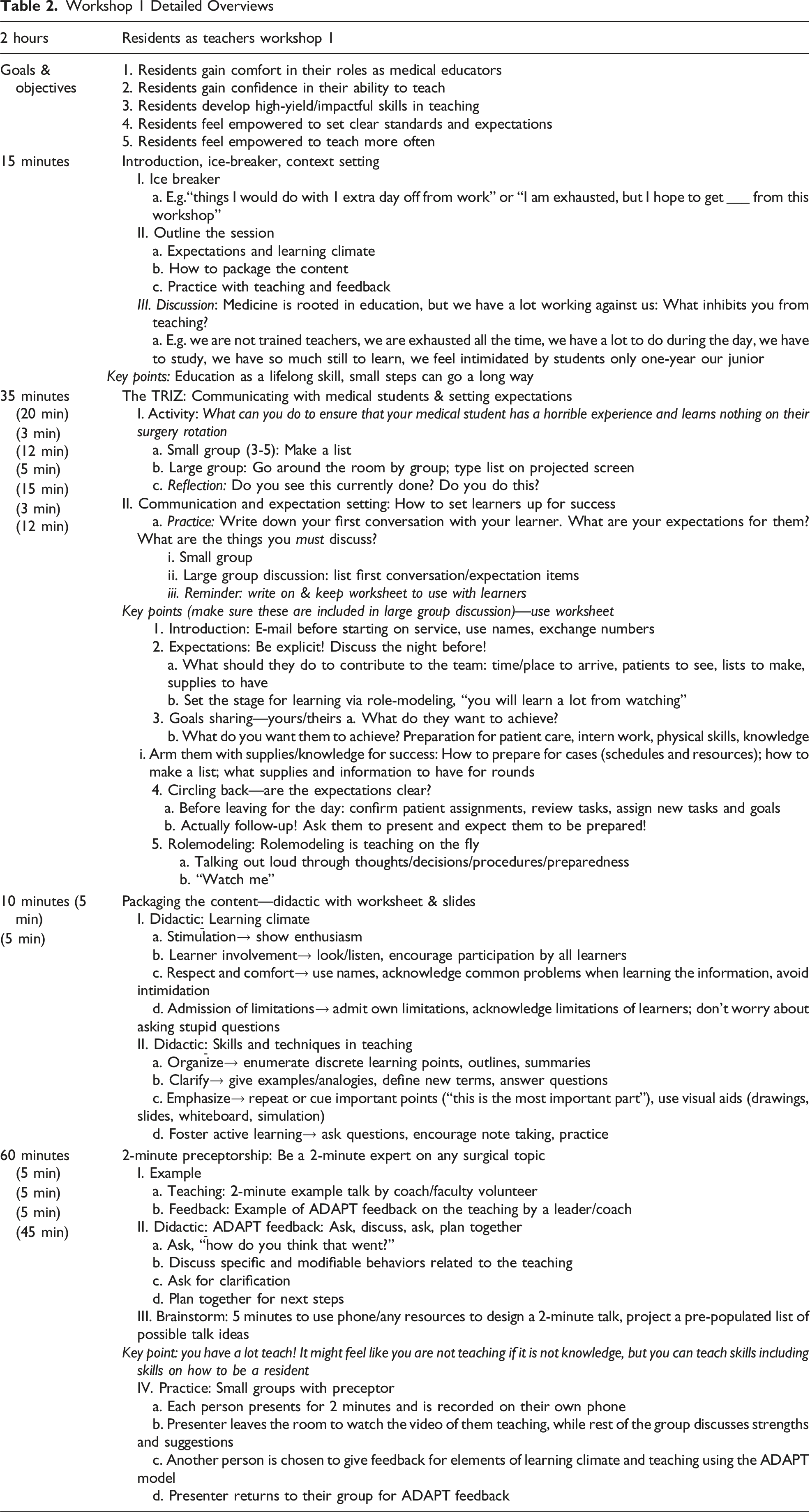
Workshop 1 Detailed Overviews
Step 5: Implementation
Pilot 1
The full curriculum was first piloted in academic year 2018/2019. Participation was limited to general surgery residents in post-graduate years (PGY) 1 and 2 from a single university-affiliated institution (n=30). Participants of this pilot attended the learning climate didactic (1 hour) and two 2-hour workshops (workshop A and workshop B).
Pilot 2
A second pilot was undertaken the following year (academic year 2019/2020) to exclusively study the feasibility, reproducibility, and impact of the workshops. Participation was broadened for pilot 2 to both general surgery and surgical subspecialty (orthopedic, urologic, otolaryngology, and plastic) PGY-1 and -2 residents. Only workshop A was able to be studied due to the constraints of COVID-19. Workshops A and B in pilot 1 and workshop A in pilot 2 were offered twice to account for vacations, call schedules, and urgent clinical matters (Tables 1 and 2).
Step 6: Assessment Design
The curriculum was assessed using a retrospective pre/post-survey. In this design, residents responded retrospectively to how they felt before the curriculum at the same time as they responded to how they felt after the curriculum. This assessment strategy was chosen instead of Observed Structured Teaching Exercises (OSTEs) as OSTEs are resource intensive and may not accurately represent performance in real situations. A retrospective pre/post is also favored over separate pre- and post-surveys in educational studies whose participants commonly over-estimate their initial self-assessment in teaching and tend toward over-confidence before they understand the nuances of the curricula.13-15,27,28 We sought to assess change in comfort (defined as a task that can be done with ease) and confidence (defined as a task one feels skilled or good at), as well as change in practices.
The survey tool was created using an iterative approach. The questions were created and then assessed by several senior residents and faculty members. After edits for clarity and ease, the tool was then sent as an anonymous survey that was completed 2-4 weeks after each pilot.
The survey assessed the first three Kirkpatrick Levels of Evaluation: reaction to the curriculum, lessons learned, and behavior change.
The survey had four main sections: 1. Demographics: PGY level and training program. 2. Self-reported pre-curriculum and post-curriculum comfort, confidence, and practices or beliefs for each of roles in and perception of teaching, setting expectations, teaching, and giving feedback. 3. Recall and application. 4. Evaluation of the curriculum.
Pilot 1 was assessed on a 4-point Likert scale, with no neutral option, to distinctly assess if this curriculum was helpful and valuable. This scale was utilized to encourage participants to choose a definitive response (ie, confident vs not confident) since the neutral response is theorized to be chosen to reduce cognitive effort as described by the central tendency bias. Pilot 2 was assessed on a 5-point Likert scale that included a neutral response option. Strongly disagree was coded as 1 and strongly agree was coded as 4 or 5 based on either the 4- or 5-point scale. Only complete surveys were included in the analysis. The complete survey tool is provided as supplemental content.
Statistical Analysis
For unadjusted analysis of pre-curriculum to post-curriculum change, Student’s t-tests were employed. For analyzing improvement, a 1-sided P-value of <0.05 was deemed significant to reduce the risk of a type II statistical error. A 1-sided statistic was deemed appropriate as the curriculum was not to felt carry a risk of detriment. Multivariate analysis with linear regression was used to assess the impact of PGY level, additional attendance at workshop B, and personal pre-curriculum self-assessment mean baseline score on mean overall pre-to-post change (2-sided P-value >0.05 as significant). Initially, unadjusted models were calculated followed by the development of a parsimonious model utilizing a backward elimination strategy. Descriptive statistics were used to analyze the course evaluation questions.
Results
Pilot 1
26 of 30 general surgery PGY-1 and PGY-2 residents participated in this course, 21 of whom responded to the survey in full (81% response rate). Survey respondents comprised 12 PGY-1 and 9 PGY-2 residents. The didactic session and workshop A were better attended (100% of respondents) than was workshop B (14 of 21, 67% of respondents).
Pre-Curriculum to Post-Curriculum Change
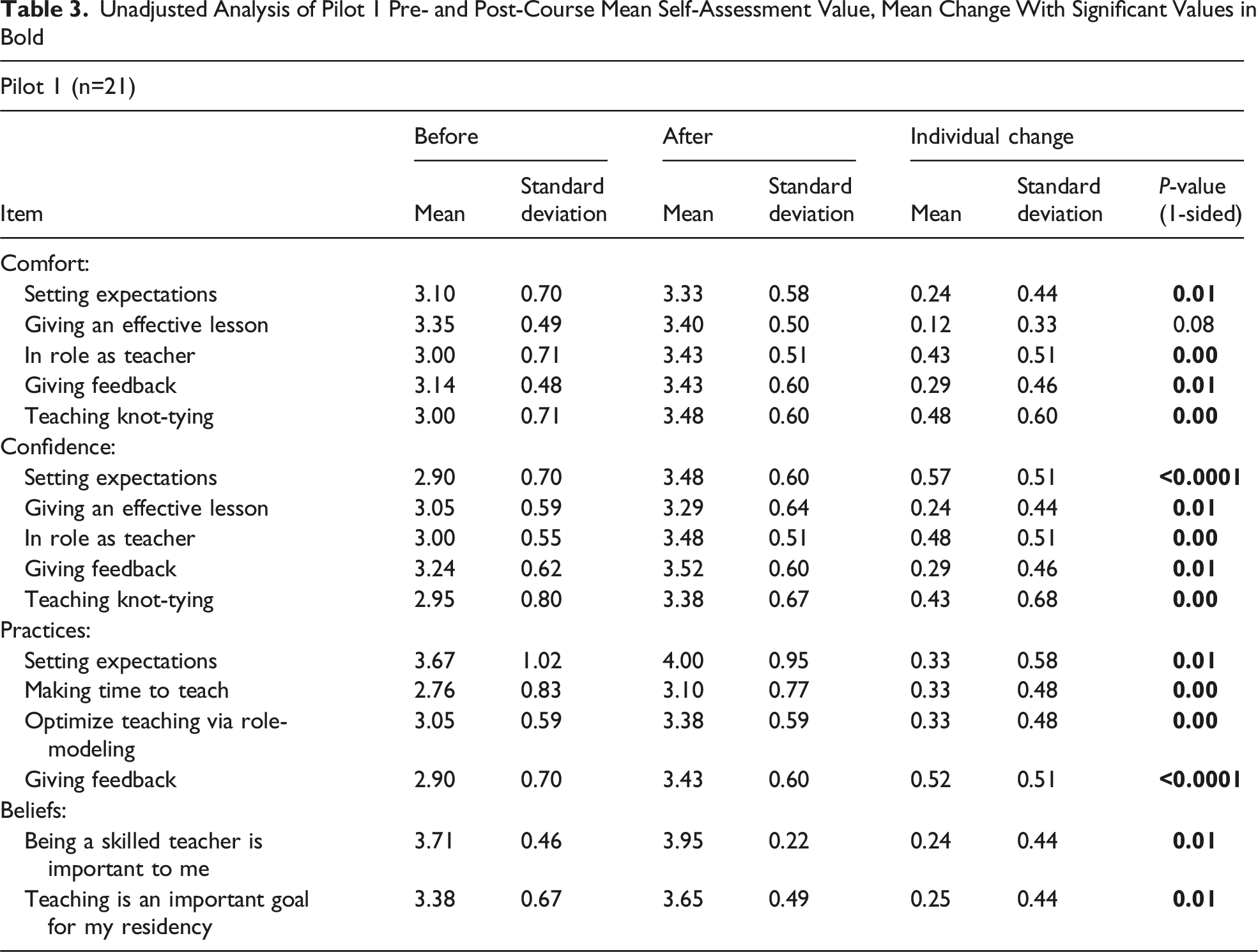
Unadjusted analysis demonstrated a statistically significant improvement in self-assessment and teaching perceptions from before to after the curriculum in all areas except comfort giving an effective lesson. Comfort, defined as a task that can be done with ease, improved in setting expectations, roles as a teacher, teaching knot-tying, and giving feedback (P < 0.02 for all) (Figure 1A). Confidence, defined as feeling skilled or good at, improved in setting expectations, roles as a teacher, teaching knot-tying, giving an effective lesson, and giving feedback (P < 0.02 for all) (Figure 1B). Residents also significantly increased how frequently they set expectations, made time to teach, gave feedback, and taught via role-modeling. Additionally, respondents reported a greater belief that being a skilled teacher was important to them and that teaching was an important goal of the residency program (P < 0.02 for all) from before-to-after the curriculum (Figure 1C) (Table 3). Pre- and post-curriculum self-assessment Unadjusted Analysis of Pilot 1 Pre- and Post-Course Mean Self-Assessment Value, Mean Change With Significant Values in Bold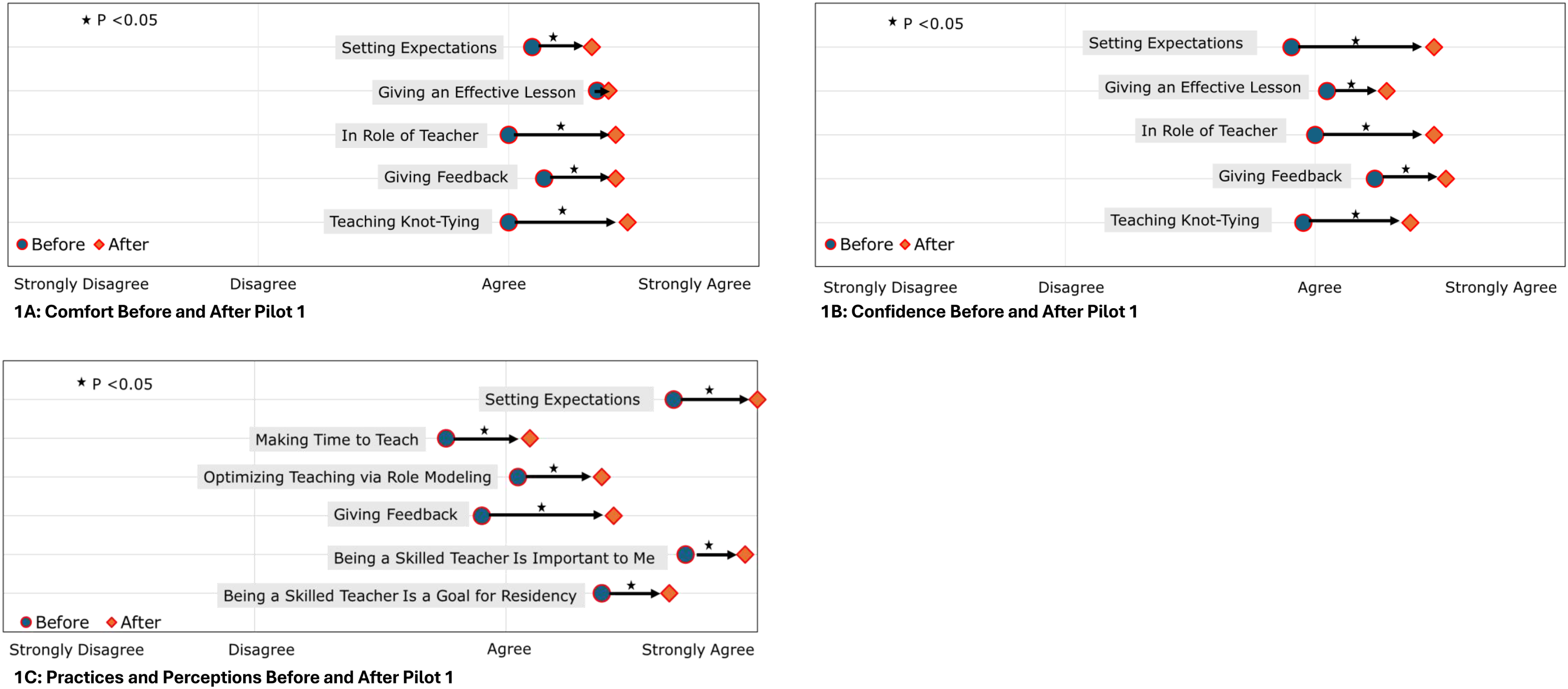
On multivariate analysis, PGY level, mean baseline score, and attendance at workshop B did not significantly alter mean overall change from pre-to-post curriculum (P > 0.05 for all, supplemental table 1).
Content Application and Course Evaluation
One hundred percent of respondents reported that they applied the content learned from these sessions (14 strongly agree and 7 agree) and 100% agreed or strongly agreed that this course was a good use of their time (13 strongly agree and 8 agree). One hundred percent of respondents also described the course as being an effective way to teach them to teach (16 strongly agree and 5 agree). Lastly, 100% of respondents reported that the course should be given to future classes as well.
Pilot 2
After pilot 1 demonstrated the residents-as-teachers curriculum was useful and valuable, junior residents from subspecialty programs were invited to participate along with the following year's general surgery residents in a second pilot that exclusively studied workshop A. The 30 participants in this pilot included 12 PGY-1 general surgery residents, 2 PGY-2 general surgery residents who did not previously take the course, and 16 PGY-1 and -2 residents from surgical subspecialties.
In total, 30 junior residents attended this year's workshop A, of whom 26 started the survey tool and 19 completed it in full. Of the 19 completed surveys, 13 were by general surgery residents and 6 were by subspecialty surgical residents.
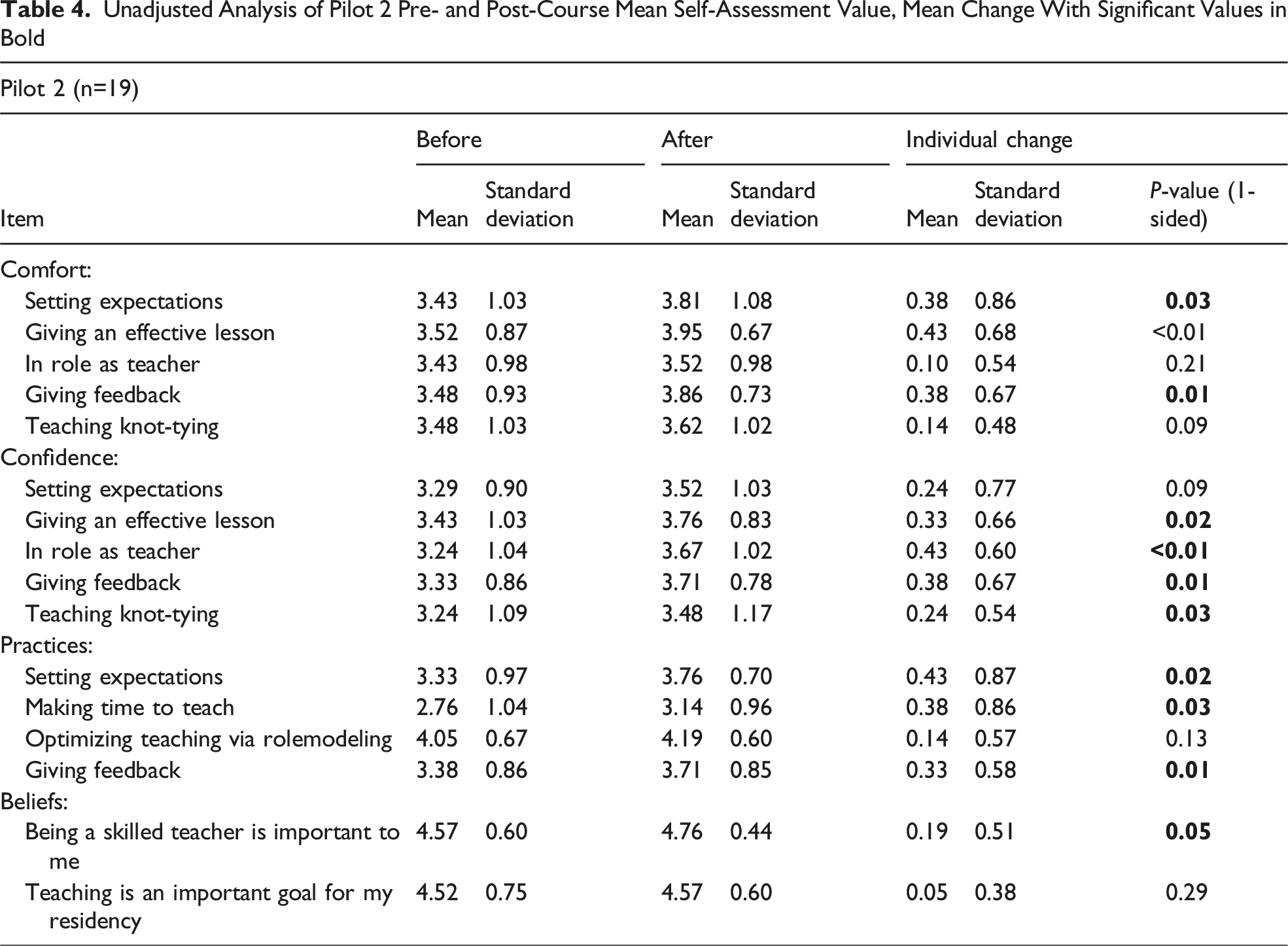
Pre-Workshop to Post-Workshop Change
Unadjusted analysis shows a statistically significant improvement in self-assessed comfort from pre-to-post workshop in setting expectations, giving an effective lesson, and giving feedback (P < 0.05 for all). Confidence improved in their role as a teacher, teaching knot-tying, giving an effective lesson, and giving feedback. Residents also significantly increased how frequently they set expectations, teach their learners, and give feedback.
Unadjusted Analysis of Pilot 2 Pre- and Post-Course Mean Self-Assessment Value, Mean Change With Significant Values in Bold
Discussion
A residents-as-teachers course is a necessary and often neglected part of surgical training. Upon entering residency, the surgical intern prioritizes learning the intricacies of patient care, studying diseases, and honing their operative skills. In addition to those daunting missions, residents immediately become teachers, a role that is unfamiliar and under-prioritized. Surgery residents are nonetheless vital to undergraduate medical education.2,3,29 Because competing demands and work-hour regulations limit residents’ availability for non-clinical skill-building, any residents-as-teachers course must be time efficient. The workshop-based course we present here, constructed on consensus guidelines and published assessments, is both feasible and effective. Importantly, our curriculum is easy to reproduce and is experiential with opportunities for teaching and giving feedback.
Our first pilot proved that our designed curriculum was both feasible and effective. It also identified that the initial 2-hour interactive workshop (workshop A) was the most valuable part of the curriculum. There was no discernable difference in assessed outcomes if workshop B was or was not attended. The course was implemented without issue and required minimal resources: a conference room, one faculty member, additional facilitators (other faculty or chief residents) for an ideal ratio of one facilitator per four-to-six residents, and dinner. Workshop A is included in Tables 1 and 2 to support reproducibility. Accommodating call schedules, avoiding clinical distractions, and remaining within duty hours were some of the greatest obstacles for implementation. To overcome this, we offered each workshop on two separate occasions in the evening from 6 to 8 pm so that nearly all residents were able to attend (86%). We created a schedule based on the residents’ call schedules, designated the workshop as mandatory with the Program Director’s approval, counted the hours in the workshops toward their 80-hour work week, and provided dinner. During the second pilot, workshop A alone was offered to a broader audience of both general and subspecialty junior surgery residents. There was no difference in the impact from the workshop between general and subspecialty residents. Successful reproduction of this workshop once again confirmed feasibility and established reproducibility to a wider participant group.
We assessed the course with retrospective pre/post-self-assessment surveys that clearly identified improvement in resident comfort, confidence, behaviors, and perceptions across tasks. Building confidence—having the resident feel skilled or good at teaching—was a goal of our curriculum as we postulated that if a resident felt more confident teaching, they would teach more effectively and more often. We also sought to improve residents’ comfort with teaching—making them feel like teaching behaviors were easy or natural—as we postulated that this would encourage and empower residents to teach and role-model. For example, if a resident lacked a clear model for giving feedback, they would be uncomfortable giving and therefore unlikely to give feedback.
As a reflection of having increased comfort and confidence with teaching, residents reported that after the course they had indeed enhanced their teaching behaviors. Residents reported that they more often set expectations with their learners, made time to teach, gave their learners clear feedback, and optimized teaching via role-modeling.
Notably, this curriculum significantly increased participants’ perceptions of the importance of being a skilled teacher and the extent to which they understood that learning to teach was a goal of their residency training—ideals aligned with the ACGME and the LCME.5,6 Perhaps the most impactful outcome of the curriculum is the enhanced perspective that being a skilled teacher is a goal, as goals motivate residents to further focus on and improve their skills. We attribute this shift to the close involvement and clear support of the program leadership, as had been suggested by prior successful programs.20,29
There are several limitations to this study. This is a single-institution study and thus its broad reproducibility is yet to be proven. Additionally, the facilitator of the sessions was the same individual over the two pilot years; although the curriculum is designed so nearly anyone could facilitate it, this too has not yet been proven. Finally, a retrospective pre/post survey may not be an accurate measurement of the impact of the course because it is vulnerable to recall bias due to the nature of pre/post-assessments and the time delay in completion of the survey tool (2-4 weeks). For future studies, this course and assessment tool could be offered and validated by an outside institution.
An additional limitation is the subjective nature of comfort and confidence and notable issues surrounding a portrayal of confidence. The sociocultural context of surgical training has been shown to add pressure on surgery residents to portray confidence. 28 The curriculum is not intended to enhance false confidence; our hope is that real comfort and genuine confidence in teaching are obtained through the acquisition of actual skill. An advantage of training junior residents, particularly early in the year, is that they are less likely to portray over-confidence. Rather, junior resident teaching may be hindered by undeserved insecurity in their roles as teachers.
In conclusion, this feasible, interactive, and reproducible course improved residents’ comfort and confidence in teaching, their perception of the importance of teaching, and the frequency of their teaching.
Supplemental Material
Supplemental Material - Teaching the Learner to Teach: An Effective and Reproducible Curriculum to Engage Junior Residents as Educators, a 2-Year Experience
Supplemental Material for Teaching the Learner to Teach: An Effective and Reproducible Curriculum to Engage Junior Residents as Educators, a 2-Year Experience by Mollie R. Freedman-Weiss, Nathan A. Coppersmith, Martin Slade, Dana Dunne, John Encandela, Samantha L. Ahle, Janet P. Hafler, and Peter S. Yoo in The American Surgeon™.
Supplemental Material
Supplemental Material - Teaching the Learner to Teach: An Effective and Reproducible Curriculum to Engage Junior Residents as Educators, a 2-Year Experience
Supplemental Material for Teaching the Learner to Teach: An Effective and Reproducible Curriculum to Engage Junior Residents as Educators, a 2-Year Experience by Mollie R. Freedman-Weiss, Nathan A. Coppersmith, Martin Slade, Dana Dunne, John Encandela, Samantha L. Ahle, Janet P. Hafler, and Peter S. Yoo in The American Surgeon™.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.