
Abstract
Background
Although frequent, patient bypass of local surgical care (bypass) remains understudied. No prior work has evaluated the association between bypass and local surgeon workforce density.
Methods
This is a retrospective cohort study of North Carolina patient bypass (receiving care at a hospital ≥ 10 miles farther from the nearest surgery-capable hospital) from 2016 to 2019 for urgent/emergent surgery. The association between bypass and clinical, sociodemographic, and NSH characteristics was estimated using logistic regression.
Results
23.7% of patients (n = 9864) bypassed local surgical care. These patients traveled further for care (median miles 25.8 vs 7.4). Living in counties with the lowest general surgeon workforce density (aOR: 1.58, 95% CI: 1.16, 2.16) and second lowest workforce density (aOR: 1.55, 95% CI: 1.26, 1.90) was associated with bypass.
Discussion
Approximately 25% of patients undergoing urgent/emergent general surgeries bypassed their nearest surgical care. Patients in counties with lower workforce density were more likely to bypass the nearest surgical hospital.
Introduction
Worsening access to general surgical care in the U.S. poses a substantial threat to patients with surgical diseases. 1 Concurrently, patients are migrating their care to higher-resource centers. Bypass for elective surgeries exceeds 50% of cases, with rates of Emergency General Surgery (EGS) bypass approaching 40% in some cohorts.2,3 Patients who bypass local surgical care are at increased risk of complications, prolonged length of stay, ICU admission, and mortality. 4 Despite these adverse outcomes, the patient and hospital factors influencing bypass of local care have received limited study. While bypass has been associated with low spatial access to care, 3 previous work has not directly tested the association between local surgeon workforce density and patient bypass. Additionally, bypass rates were shown to be spatially autocorrelated at the Zip Code Tabulation Area (ZCTA) level in a retrospective study of California EGS patients. 3 Whether this remains true in a different geography is unknown.
This study sought to describe bypass among patients receiving urgent and emergent surgery for general surgical diseases, evaluate for spatial autocorrelation of bypass rates, and estimate associations between patient clinical, sociodemographic, and hospital characteristics and the probability of bypass. We hypothesized that bypass rates would exhibit geospatial clustering at the ZCTA level and that bypass would be more likely in counties with lower surgeon workforce density.
Methods
This retrospective cohort study evaluated inpatient admissions of North Carolina residents from 2016 to 2019, utilizing the North Carolina Acute Care Discharge Data, a statewide database of all non-federal hospital discharges in North Carolina. 5 We included patients admitted between October 1, 2015, and September 20, 2019, who were ≥ 18 years old, and underwent urgent or emergent surgery for common surgical diseases within 7 days of admission. We excluded patients who transferred from another health care facility. We included patients undergoing enterectomy, lysis of adhesions, gastric resection or repair, duodenal repair, appendectomy, cholecystectomy, and abdominal wall hernia repair. Patients presenting with complications of enteral access surgeries, or of existing enterostomies, were excluded as we assumed they would preferentially present to their operative surgeon, confounding their decision to bypass local surgical care. Diagnosis codes and procedure codes were evaluated using ICD-10-CMS, ICD-10-PCS, and CPT codes (Supplemental Data 1).
Defining Bypass
Bypass of surgical care was defined as patients who underwent surgery at a hospital farther from the closest hospital providing general surgical care (Nearest Surgical Hospital or NSH). Nearest Surgical Hospitals performed at least 36 cholecystectomies, herniorrhaphies, or colectomies per year (a proxy for at least three general surgery procedures per month). Prior work has defined NSHs by procedural volume and presence of EGS service lines.2,3 A threshold that is too low might include hospitals that report a procedure due to coding errors, while one that is too high might exclude surgery-capable rural and critical access hospitals.
To determine the distance between patients and hospitals, patient ZIP was matched to Zip Code Tabulation Area (ZCTA) centroids using the USD-mapper crosswalk files. 6 The driving distance between all ZCTA centroids and hospitals in North Carolina was calculated using network analysis in QGIS 3.38.1 and the QNEAT package. 7
We also applied a “difference-in-distance” threshold to our analysis, as has been previously described.3,8,9 Defining bypass as going to a hospital any distance further than the NSH implies that patients making almost equivalent distance decisions (eg, 4 miles vs 5 miles) would be captured as bypass if they chose the (marginally) further-way hospital. This work seeks to capture “bypass” where patients travel substantially further for care, as this extra travel poses economic and physiologic costs. 10 The current analysis utilized the difference-in-distance between the patient-NSH and patient-treating hospital routes, defining cohorts at the 10-, 20-, 30-, 40-, and 50-mile thresholds.
Assessing Geospatial Autocorrelation
Bypass rates were aggregated at the ZCTA level, with the denominator being all patients who required surgery in the ZCTA. Global spatial autocorrelation was evaluated using a Global Moran’s I, and local spatial autocorrelation was analyzed using the Local Indicators of Spatial Association (LISA) test. Neighbor weights were assigned using Queen contiguity and 1st-order neighbors. ZCTAs missing a bypass rate (38%, or 1269 ZCTA-years) were excluded from the geospatial analysis.
Determining the Association Between Workforce Density and Bypass
General surgeon workforce density (WFD) at the county level was determined using North Carolina Health Professions Systems Data from the Cecil G. Sheps Center for Health Services Research, which includes all actively licensed, non-federally employed North Carolina general surgeons. 11
Patient Characteristics
The Social Deprivation Index (SDI) was utilized to capture patient ZCTA-level characteristics, including poverty, education, employment, housing status, household composition, and transportation access. 12 Patient sex, race, ethnicity, and insurance status were also included. Rurality has been previously associated with the probability of bypass. 3 Rural-Urban Commuting Area (RUCA) codes were used to represent rurality, categorized by primary RUCA score: metropolitan (0-3), micropolitan (4-6), small town (7-9), and rural (10). 13 Sensitivity analysis was performed utilizing the Federal Office of Rural Health Policy (FORHP) definition of rurality, which accounts for road conditions and population density within otherwise “metropolitan” counties. 14 Elixhauser comorbidity score was calculated for each observation. 15
Hospital Characteristics
The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores, previously associated with bypass, were included. 16 Hospital bed size, ownership status (for-profit, non-profit, or government-owned), operating margins, hospital rurality, the number of beds, and membership in a larger health system were determined using the Healthcare Cost Report Information System for fiscal year 2019. 17
Analysis
Bivariate analysis of the association between selected variables and bypass was performed using the Wilcoxon Rank-Sum and Chi-square tests, as appropriate. The association between general surgeon workforce density and bypass was estimated with multivariable logistic regression, adjusting for the above-described variables. Age was not statistically significantly associated with bypass in the adjusted model, and was excluded due to high collinearity with other model variables. Standard errors were adjusted for clustering of bypass at the ZCTA level. Sensitivity analysis was performed with iteratively higher difference-in-distance thresholds (10-50 miles).
Geospatial autocorrelation was assessed using the r/geoda package in R 4.5.1. Bivariate association testing and multivariable logistic regression were performed in Stata 17.0 (StataCorp, College Station, Texas). This study was determined to be IRB-exempt by an institutional review board at the University of North Carolina at Chapel Hill.
Results
From 2016 to 2019, 43,407 patients were admitted with a diagnosis of interest and underwent related urgent or emergent surgery. Patients were excluded if their NSH closed during the study period (n = 15), were missing HCRIS data (n = 849), or used duplicate HCRIS data from a larger hospital (n = 970), leaving 41,573 patients. The most common procedures were cholecystectomy (46.5%, n = 19,337), followed by appendectomy or drainage (19.1%, n = 7940), abdominal wall hernia repair (14.6%, n = 6075), and large bowel surgery (13.8%, n = 5724). 23.7% of patients (n = 9864) bypassed local surgical care for a hospital at least 10 miles further away, with similar rates across diseases (Supplemental Data 2, Supplemental Data 3). As the difference-in-distance threshold increased, the number of patients classified as bypassing local surgical care decreased (Figure 1). The number of patients classified as bypassing local surgical care based on differing thresholds of the difference-in-distance between local surgical hospitals and treatment hospitals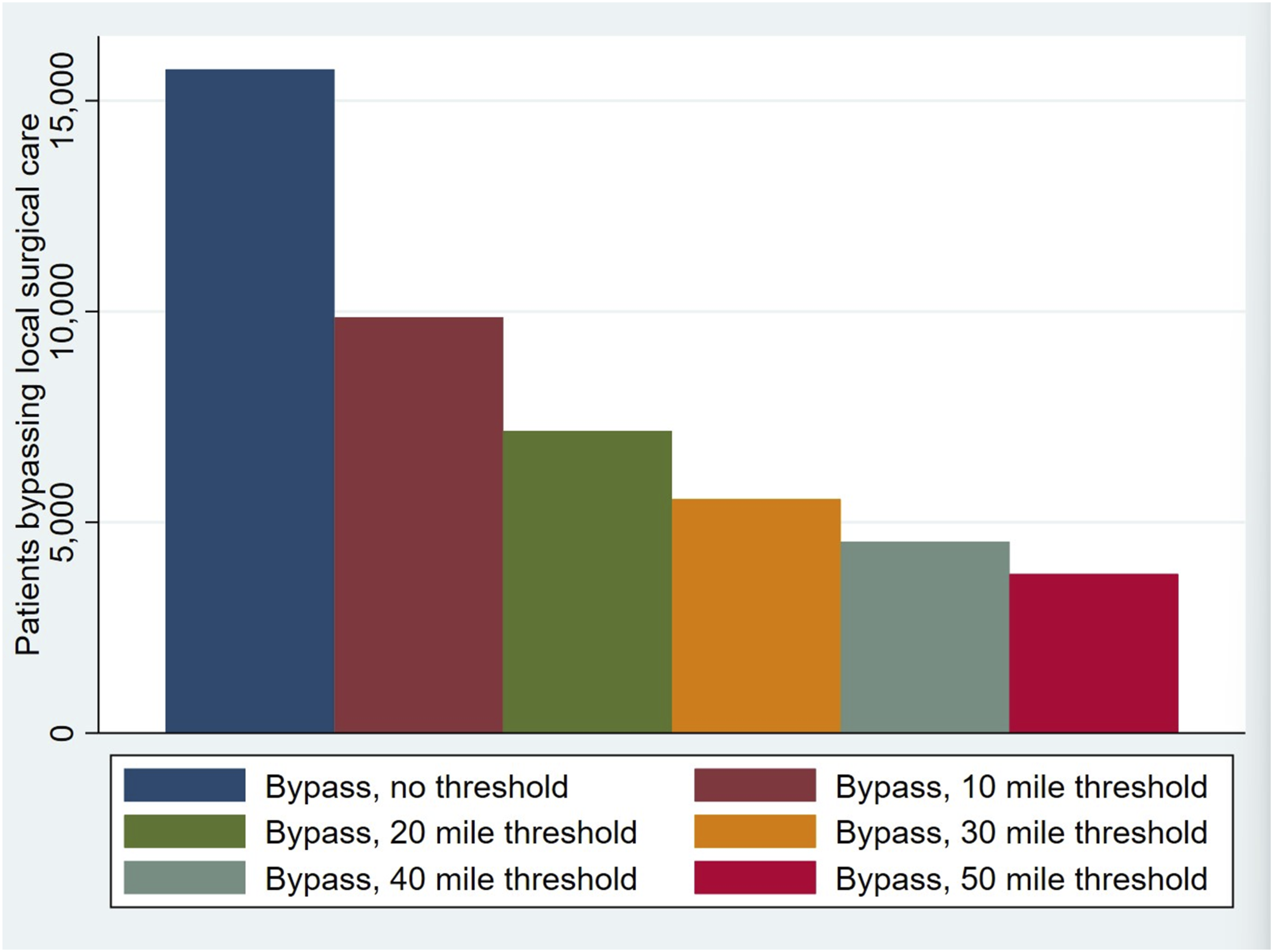
Geospatial Autocorrelation
Bypass rates were highly geospatially autocorrelated at the ZCTA level across the years of study and bypass definitions, with all P-values of the Moran’s I test < .001 (Supplemental Data 4). Over the four years of study, specific ZCTAs were clustered with persistently higher bypass rates than others in the state (Figure 2). Choropleth map plotting the results of the Local Indicators of Spatial Association (LISA) analysis for each ZCTA over the four years of study, 2016-2019, using the 10-mile “buy-in” cohort. ZCTAs were assigned a 1 for each year their LISA result was high-high and −1 for each year their LISA result was low-low. These values were then summed over the four years of study for each ZCTA, with darker purple indicating a ZCTA with a persistent high-high LISA value from 2016 to 2019 and darker red indicating a ZCTA with a persistent low-low LISA value from 2016 to 2019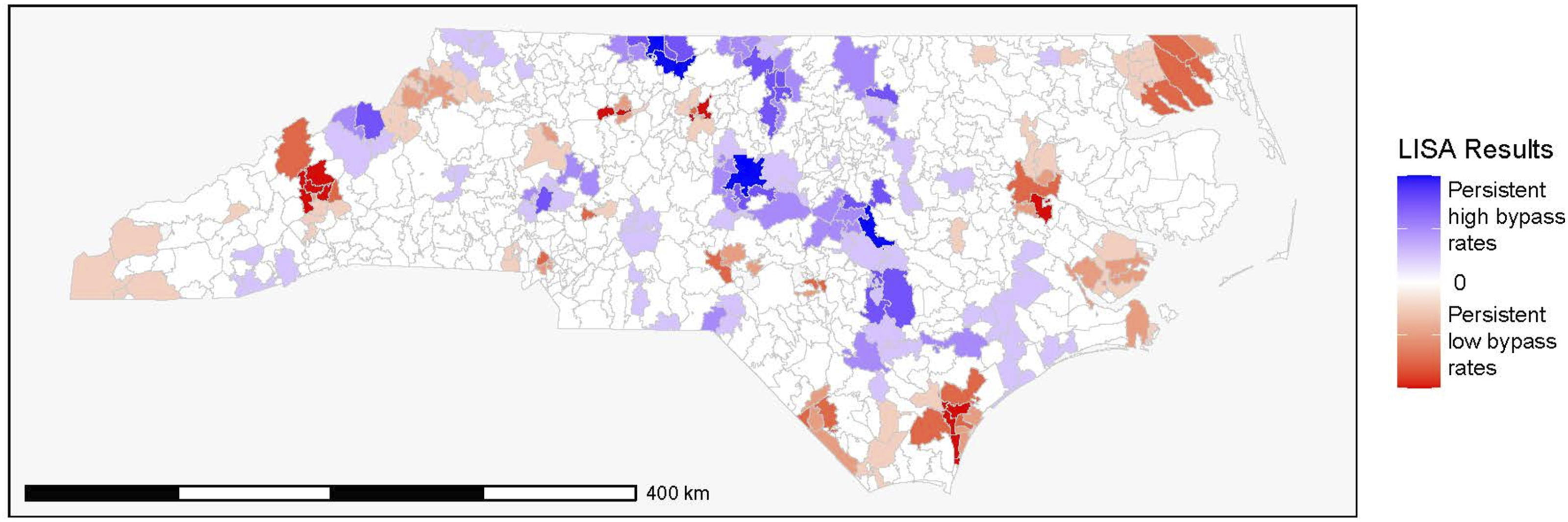
Association of Patient, Hospital, and Workforce Characteristics with Bypass
Characteristics of Patients Who Did and Did Not Bypass Local Surgical Care and the Characteristics of Their Nearest Surgical Hospitals
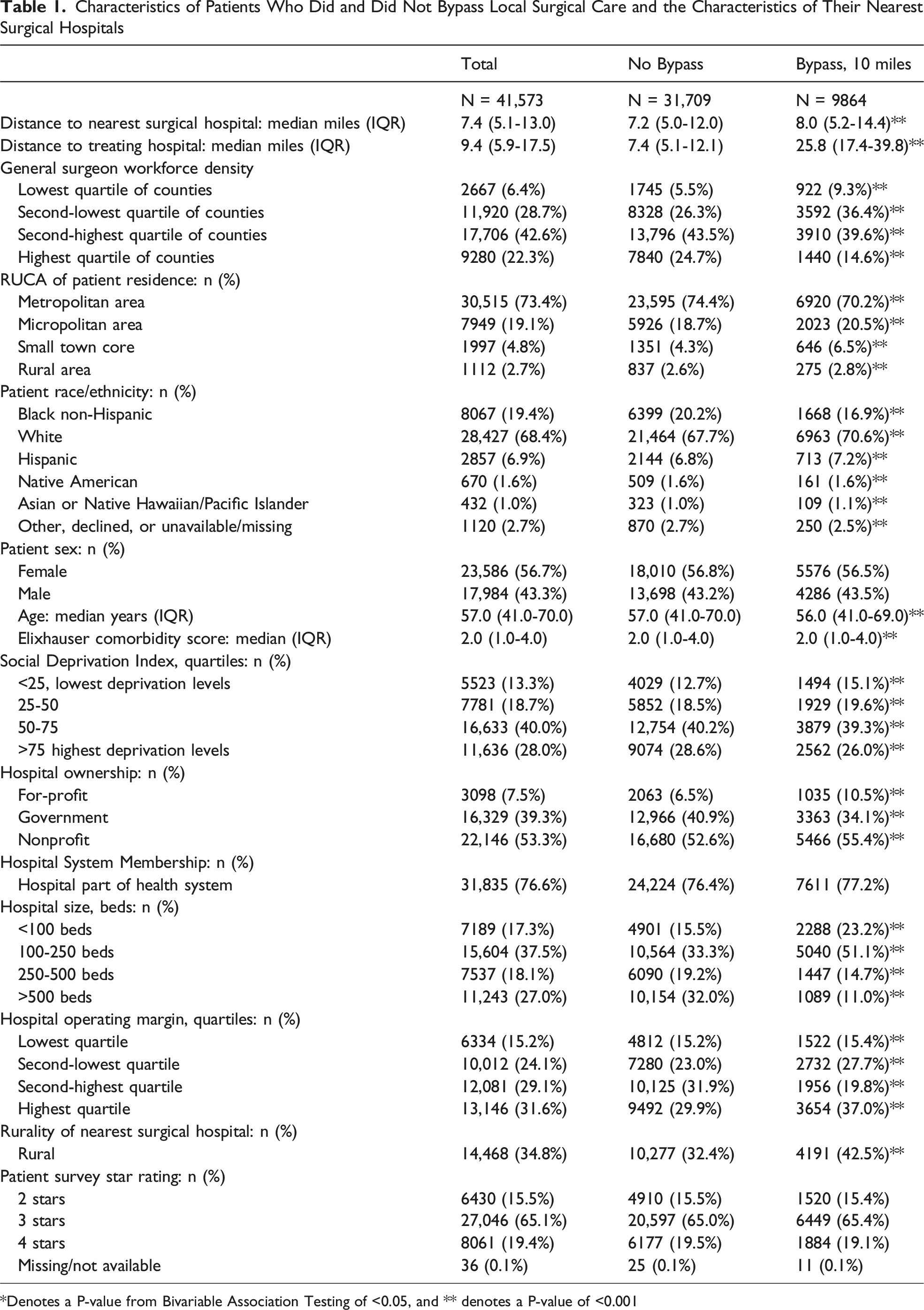
*Denotes a P-value from Bivariable Association Testing of <0.05, and ** denotes a P-value of <0.001
Results of Adjusted Multivariable Logistic Regression Evaluating the Association Between General Surgeon Workforce Density and the Odds of a Patient Bypassing Their Nearest Available Surgical Care for Management of Urgent/Emergent General Surgery Conditions. Variables Are Reported With Their Referent Category, Where Appropriate
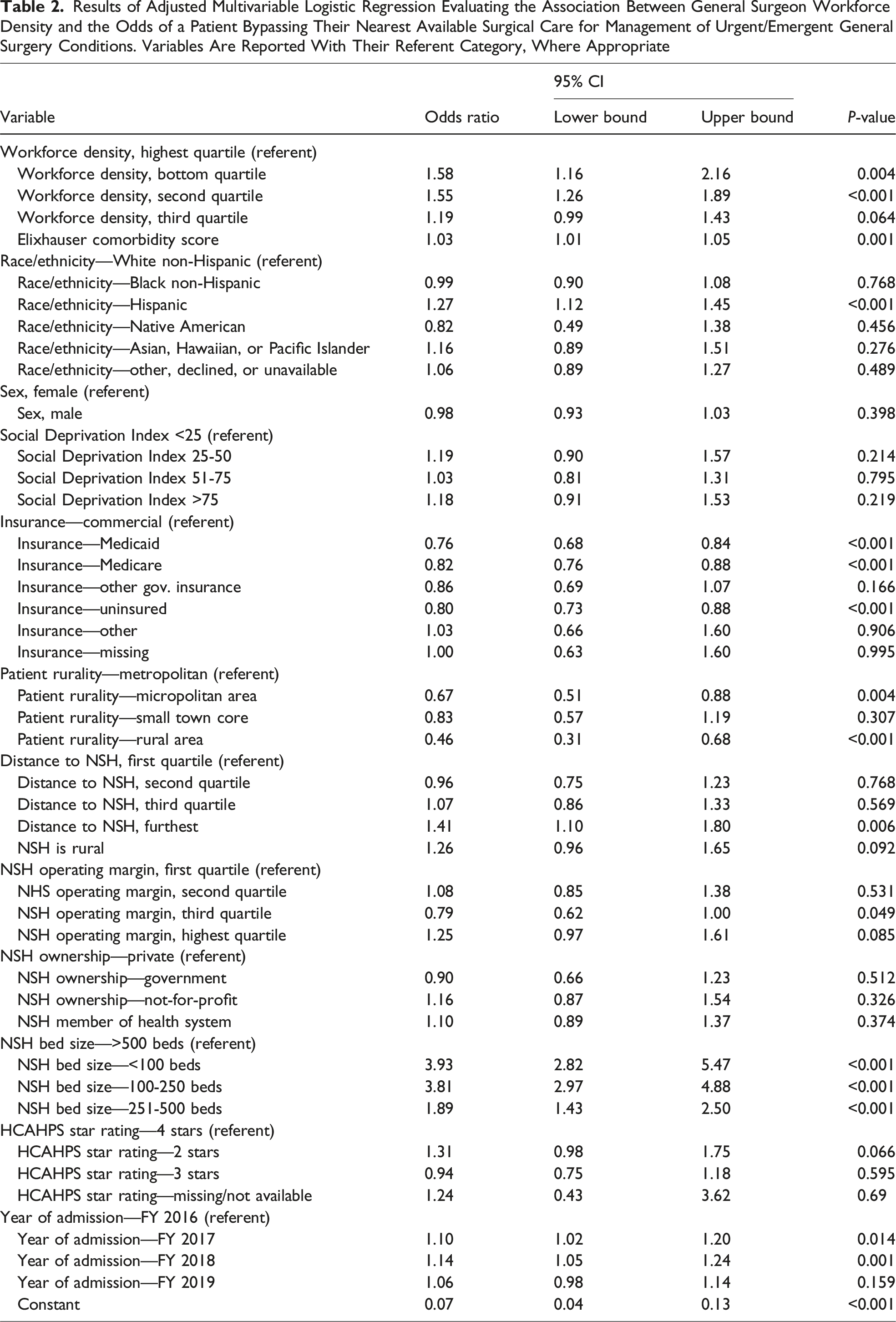
Hospitals with fewer than 100 beds (aOR: 3.92, 95% CI: 2.82, 5.47; P < .001), 100-250 beds (aOR: 3.81, 95% CI: 2.97, 4.89; P < .001), and 251-500 beds (aOR: 1.89, 95% CI: 1.43,2.50; P < .001) were all more likely to be bypassed than hospitals with more than 500 beds.
When defining bypass as at least 20 miles of additional driving, patients insured through Medicaid (aOR: 0.80, 95% CI: 0.72,0.88; P < .001) or Medicare (aOR: 0.85, 95%: CI 0.78,0.92; P < .001) and uninsured patients (aOR: 0.83, 95% CI: 0.75,0.92; P < .001), who were Black (aOR: 0.87, 95% CI: 0.80, 0.96; P = .004) or Native American (aOR: 0.63, 95% CI: 0.44,0.90; P = .012) or lived rurally (aOR: 0.59, 95% CI: 0.41,0.85; P = .004) were less likely to bypass local surgical care. Rural hospitals (aOR: 1.51, 95% CI: 1.13, 2.01; P = .005) and hospitals with lower patient survey star ratings (aOR: 1.59, 95% CI: 1.22, 2.06; P < .001) were more likely to be bypassed (Supplemental Data 6).
Discussion
In this analysis of inpatient admissions for operative management of urgent and emergent general surgical diseases in North Carolina, we demonstrate that patients living in counties with lower surgeon workforce densities were more likely to bypass their nearest available surgical care to a further away hospital and that rates of bypass were geospatially autocorrelated at the ZCTA level. We also found a persistent association between non-commercial insurance and a lower likelihood of bypassing local surgical care. Finally, we noted that smaller, rural hospitals were more likely to be bypassed. Some of our findings were sensitive to the definition of bypass used, reinforcing previous analyses that incorporated multiple definitions of bypass.3,8 Our study highlights that a priori definitions of bypass should be structured to support the question of interest and facilitate appropriate interpretation of findings.
Comparison to Previous Research
Previous analysis of bypass among EGS patients in California demonstrated bypass rates ranging from 11% to 58%, depending on cohort characteristics. In contrast, analysis of a multistate sample of rural patients found that 64.5% bypassed for elective surgeries.2,3 The bypass rate of nearly 25% reported in the current study is, as expected, lower than the bypass rate for elective surgery and sits within previously reported bypass rates for emergent general surgery procedures.
Workforce Density
Prior work evaluating EGS patient bypass found that patients living in areas with lower spatial access (incorporating procedural volume as a proxy for hospital capacity) were more likely to bypass local care. 3 The present study extends this work, demonstrating an inverse association with workforce density. Patients with access to surgical care were still bypassing local care in counties with low surgeon workforce, suggesting that the presence of surgeons is necessary but not sufficient to retain care locally. Prior work has indicated that improving local surgeon density strengthens the ability of existing practices to retain patients. 18 Whether this is true for EGS patients is unknown.
Patient Sociodemographic Characteristics
Similar to the current study, previous work has reported a positive association between private insurance and risk of bypass.2,3 However, the current analysis does not account for hospitals’ in-network status. Additionally, black patients were less likely to bypass local surgical care; this has likewise been noted in prior studies.2,3 Our results suggest that white, commercially insured patients enjoy improved mobility in care selection. Our findings that patients are more likely to bypass care in regions with lower surgical availability indicate that Black patients may face greater barriers to participating in this patient-directed mitigation of surgeon shortage.
Patient Rurality
Our findings that rural patients were less likely to bypass local surgical care, even when defining rurality using FORHP criteria, differ from prior findings of a positive association between bypass and rurality. 3 However, we found that rural patients were more likely to bypass care at the 30-, 40-, and 50-mile cohorts, suggesting that the definition of bypass influences this relationship with patient rurality. The proportion of bypassing patients classified as rural, small town, or micropolitan residents increased with each successively higher difference-in-distance definition, indicating that changes in the relationship between patient rurality and odds of bypass in the adjusted model likely reflect differences across bypass classifications.
Patient Comorbidities
As in the current study, previous work investigating bypass of local care among septic patients found that patient Elixhauser comorbidity was associated with increased odds of bypass. 9 An important consideration is that some comorbidities may only be managed at higher-volume centers, so these patients may bypass local care due to existing non-surgical clinical relationships at larger institutions.
Hospital Characteristics
Previous work 2 aligns with our findings, showing that smaller hospitals and rural hospitals were more likely to be bypassed. The effect of bypassing surgical care on small hospitals can be substantial and has been suggested as a contributing factor to rural hospital closures. 2
Limitations
This work is limited to data from North Carolina and, therefore, is not nationally representative. Another potential limitation is the accuracy of clinical coding in administrative data. There is no consensus on how to define bypass, and variations in definition can alter the size and characteristics of the bypass cohort. We included patients who underwent surgery within 7 days of admission to account for heterogeneity in operative timing across disease conditions, including small and large bowel obstruction; however, the 7-day time cut-off may include cholecystectomy or hernia patients whose care was complicated, which may confound the model results. This study utilizes 2016-2019 data and so does not account for potential changes in care patterns after the COVID-19 pandemic, which was accompanied by numerous hospital closures. 19 We cannot fully identify general surgery coverage at hospitals we designated as an NSH. Substantial barriers to providing 24/7 general surgery coverage exist for many hospitals, and thus some hospitals designated as an NSH may not have had a staff surgeon available at all times. 20 In these cases, a patient selecting a hospital other than their NSH would be incorrectly labeled as bypass (under our definition). Similarly, the data used in this analysis cannot account for other structural factors, such as ICU availability, which could shape bypass patterns. The data also cannot identify whether patients presented by personal vehicle or Emergency Medical Services (EMS). While prior work has demonstrated high rates of bypass among stroke patients transported by EMS in North Carolina, little is known about transport patterns and bypass for general surgery patients. 21 Finally, patient age was highly collinear with other variables in our model and was therefore excluded from the final model.
Conclusions
Nearly 25% of patients who underwent urgent or emergent operative intervention for common general surgical diseases bypassed locally available general surgical care for further care. Bypass rates demonstrated geospatial autocorrelation at the ZCTA level and were associated with private insurance and smaller, poorly rated hospitals. The effects of bypassing on both hospital and patient finances merit additional study, as do patient perspectives on the decision to bypass local care.
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Supplemental Material
Supplemental Material - Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization
Supplemental Material for Bypass of Local Surgical Care in North Carolina: Patient-Directed Care Destination and Utilization by Mustafa Abid, Tyler Malone, Mark Holmes, and Anthony Charles in The American Surgeon™
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by a National Research Service Award Postdoctoral Traineeship from the Agency for Healthcare Research and Quality sponsored by The Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, Grant No. T32 HS000032.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental Material for this article is available online.