
Abstract
Background
Unplanned ICU admission (UP-ICU), a benchmark of the ACS Trauma Quality Improvement Program, is linked to increased mortality and is used to accredit trauma centers. However, it is unclear whether this reflects a causal relationship or confounding by patient physiology. We hypothesized that UP-ICU, when adjusted for patient and injury factors, would not be independently associated with higher mortality.
Methods
We conducted a retrospective case-control study of adult trauma patients admitted to a level 1 trauma center (2016-2020) with hospital length of stay (LOS) > 24 hours. Controls were selected using 1:1 propensity score matching based on injury severity (RTS, GCS, BMI, base deficit) and medical comorbidities (vascular, cardiac, respiratory, renal, and substance use disorders). The primary outcome was in-hospital mortality. The secondary outcomes included discharge to rehabilitation and LOS.
Results
Among 7618 patients, the UP-ICU rate was 3.3% (254 patients). In the unmatched cohort, UP-ICU was associated with higher mortality than non-UP-ICU (8.6% vs 2.3%, P < 0.001). However, in the matched cohort, mortality was similar between groups (8.6% vs 7.4%, P = 0.745). Common reasons for UP-ICU included delayed intracranial hemorrhage, cardiac arrhythmia or ischemia, and respiratory distress.
Discussion
In a matched cohort, UP-ICU was not independently associated with mortality after adjustment for patient physiology, injury severity, and comorbidities. As such, UP-ICU is a quality metric that may have a role in reducing failure to rescue, as early escalation of care may allow patients to survive acute deterioration.
Key Takeaways
• We assessed the utility of the quality and safety metric, unplanned ICU admission (UP-ICU) in trauma patients and found that, when adjusting for patient physiology, traumatic injury, and comorbidity factors, UP-ICU was no longer associated with patient mortality. • Thus, our findings suggest that UP-ICU may have a role in reducing failure-rescue as early escalation of care may allow patients to survive acute deterioration.
Introduction
Unplanned intensive care unit admission (UP-ICU) has long been considered an important quality metric in the American College of Surgeons’ Trauma Quality Improvement Program (ACS-TQIP) evaluation of trauma centers. 1 This stems from past studies that have shown that UP-ICU is associated with increased morbidity, hospital length of stay (LOS), rates of surgery, and need for mechanical ventilation.2-4 These studies also demonstrated that patients undergoing UP-ICU were older, had more medical comorbidities, and suffered more severe injuries. 3
The isolated metric of UP-ICUs tallies all events, independent of the reason for or appropriateness of the UP-ICU. 3 Escalation to ICU level of care allows for close monitoring and early intervention in deterioriating patients. UP-ICU is designed to prevent failure to rescue (FTR), but without context regarding the level of care prior to UP-ICU and the reason for UP-ICU, a high UP-ICU rate may not be indicative of suboptimal quality of care. Furthermore, the link between overall UP-ICU and associated mortality may be overestimated, as the reasons for UP-ICU, which impact associated mortality, may vary by institution and over time, even in a system with stable overall numbers of UP-ICU.
In this study, we investigated the association of UP-ICU with mortality using a propensity-score matched analysis to control for patient and injury related factors at the time of admission including underlying medical comorbidities and injury severity. We hypothesized that patients who had an UP-ICU event would not have a significantly higher mortality rate relative to a normalized comparator group with equivalent mortality risk at the time of admission.
Methods
This study was approved by the Institutional Review Board of the University of California San Diego Human Research Protection Program (IRB: 151 611). A waiver of informed consent was granted. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed.
Cohort Selection
We retrospectively identified patients admitted to a single Level I trauma center with length of stay (LOS) greater than 24 h from January 1, 2016, to December 31, 2020 using a local trauma registry. Patients were excluded if they were under 18 years of age, if their length of stay was less than 24 h, or multiple missing data points from the electronic health record. The trauma center has 3 levels of care: ICU, stepdown, and ward, with a dedicated and closed trauma/surgical ICU. The completed checklist for the manuscript is available in Supplemental Data Table 1.
Variable Selection
Data in the local trauma registry used for this study was documented by trained trauma registrars in accordance with the guidelines set by the National Trauma Data Bank. 5 The following data were collected for each patient: patient demographics including age, sex, body mass index (BMI); medical comorbidities including history of cardiovascular disease, cerebrovascular disease, chronic kidney disease, neurological disease, cirrhosis, diabetes, dementia, congestive heart failure, chronic anticoagulation usage, hypertension, substance abuse, and chronic obstructive pulmonary disease. All comorbidities were treated as binary variables as described in the “Pre-existing conditions” section of the National Trauma Data Bank data dictionary. In addition, admission level of care as well as following admission data: base deficit, need for ventilatory support; presence of traumatic brain injury, New Injury Severity Scale (NISS), revised trauma score (RTS), and Glasgow Coma Scale (GCS) were obtained. In hospital and outcome data obtained included whether patient was ICU status at any point during their hospitalization; UP-ICU status; mortality; LOS; and need for rehabilitation at time of discharge (rehab). For patients who had UP-ICU, chart review was conducted and cause of UP-ICU, need for the following interventions within 24 h were recorded: vasopressors within 24 h of admission to ICU, intubation, cardiopulmonary resuscitation (CPR), invasive procedures, imaging, and blood transfusion. This information was obtained for the first UP-ICU event in patients who had multiple episodes during the hospitalization, and subsequent episodes were not examined to avoid confounding. Patients with more than 3 missing variables were excluded. Variable with greater than 20% of missing values were also excluded from our analysis. Missing values were imputed using multiple imputations by chained equation using the R package MICE as previously described. 6
Propensity Score Matching
For the selection of variables on which to match, we aimed to match on a set of variables that reflected the patient’s initial physiological illness as well as baseline comorbidities as these were non-modifiable factors that are predictive of adverse events post traumatic injury. 7 To that effect, we followed the recommendation put forth by Haider et al in 2012 in which they specified the “basic minimum” set of covariates to adjust for in any trauma study on mortality—age, sex, any type of anatomic severity, any type of physiologic severity, and mechanism or type of injury.7,8 We used revised trauma score (RTS), admission GCS, and admission base deficit as physiological severity measures. However, we retained both GCS and RTS as variables in our analysis given their distinct roles in trauma triaging. We assessed for collinearity and variance inflation factors (which were <2) and there was no significant collinearity identified. The NISS was used as the anatomic severity grading, and penetrating vs blunt injury used to categorize type of injury. In addition, we included admission level of care into our matching algorithm. Lastly, we used a multivariable logistic regression model with backward selection to identify relevant medical comorbidities associated with mortality. Variables that met the P-value threshold <0.20 were included in the propensity-score matching model as this approach has been shown to reduce bias and variance.9,10 Once the final model was selected, we ran a 1:1 optimal matching algorithm without replacement using propensity score to obtain the case and control cohorts. The optimal matching is an extension of the nearest neighbor matching but aiming to optimize absolute distance between pairs to improve balance. 10 Post matching balance assessment was evaluated based on the standardized mean difference (SMD) for each variable. Balance was considered adequate if all variables had to have an SMD ≤0.1.
Outcomes
Our primary outcome of interest was in-hospital mortality. Secondary outcomes of interest were LOS, need for rehabilitation facility on discharge, and causes for UP-ICU admission.
Statistical Analysis
The statistical software R (Version 4.0.5) was used to conduct all analyses. Matching and SMD calculation for balance assessment was done using the R package (MatchIt Version 4.9-11). 11 Two-proportion z-test was used to compare proportional differences in event rates between groups. For groups with small sample sizes (n < 5), Fisher’s exact test was used instead. P-value <0.05 was defined as threshold of statistical significance.
Results
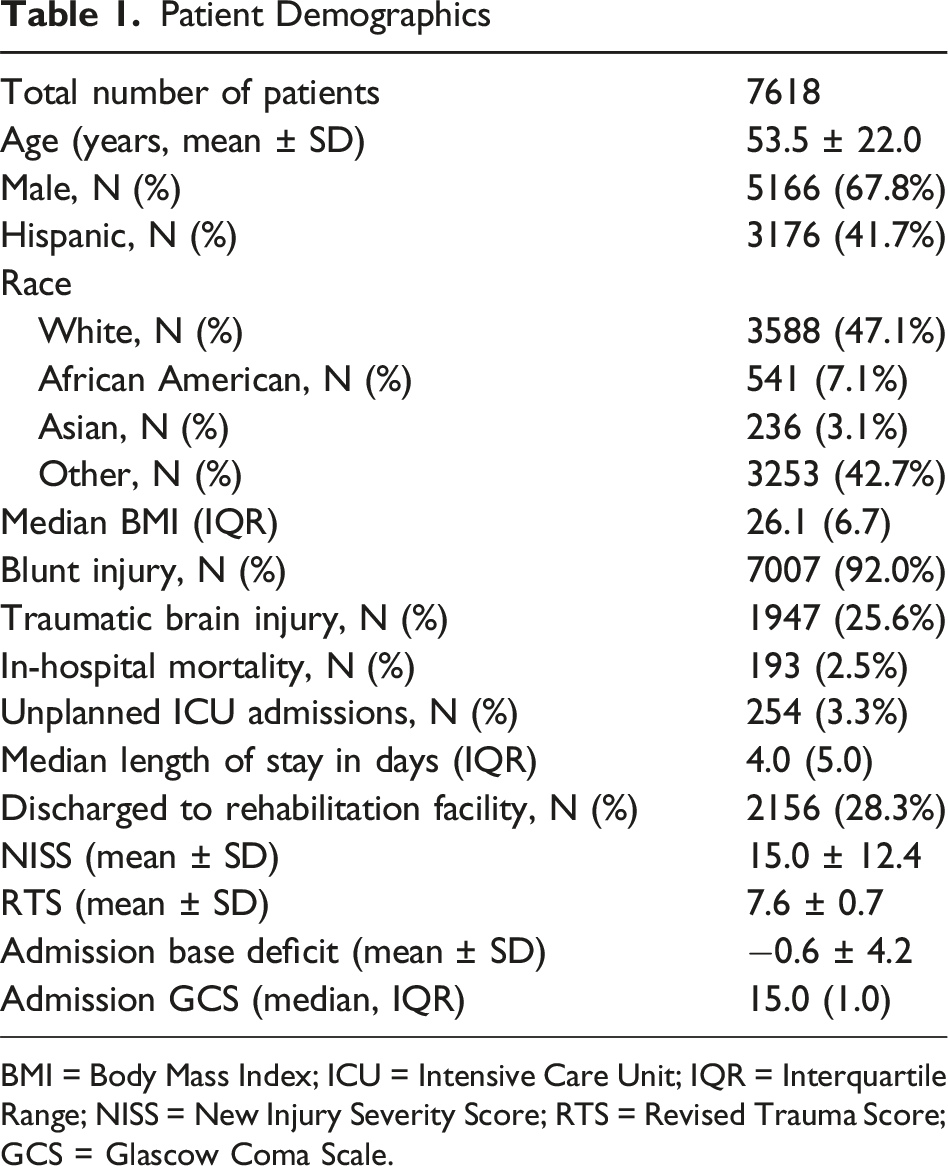
There were 13 010 patients identified in the trauma registry during the 5-year study period, including 7864 patients who met the criterion of LOS >24 hours. 246 patients (3.1%) with missing values for multiple variables and were excluded as they had multiple missing variables. No variables had more than 20% missing values. There were 1222 patients without base deficits (15.5%), 1478 patients with missing BMI (18.8%), and 138 patients with missing revised trauma scores (1.8%). All 3 variables were inputted with MICE R package. The final study cohort comprised 7618 patients, including 254 patients who had UP-ICU. The CONSORT diagram in Figure 1 shows the distribution of patients in this study. The mean age was 53.5 years, and the sample was predominantly male (Table 1). A total of 92.0% patients sustained a blunt injury. The overall in-hospital mortality rate was 2.5%, and UP-ICU rate was 3.3%. CONSORT Diagram of Study Patient Demographics BMI = Body Mass Index; ICU = Intensive Care Unit; IQR = Interquartile Range; NISS = New Injury Severity Score; RTS = Revised Trauma Score; GCS = Glascow Coma Scale.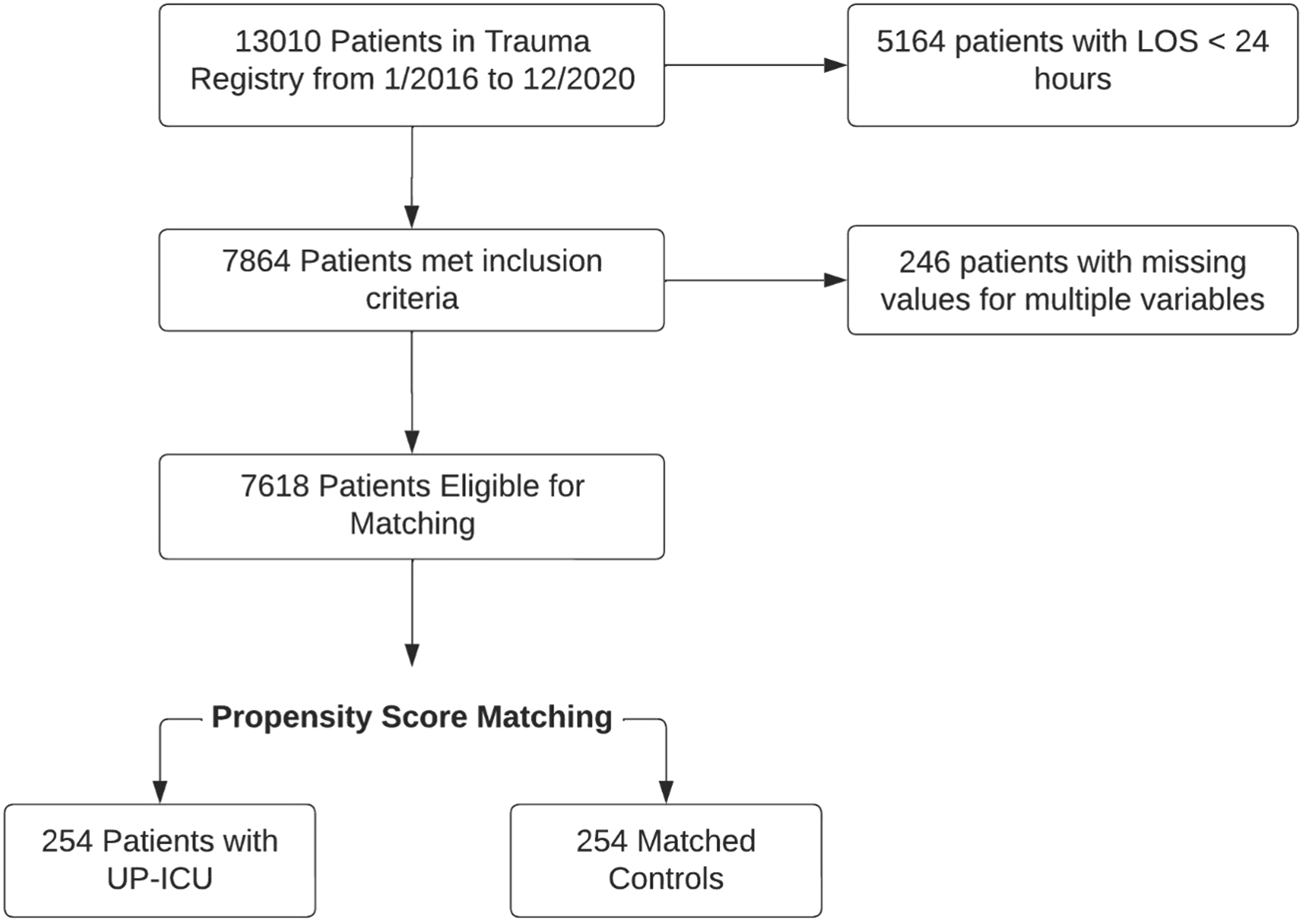
UP-ICU Patients Compared to Unmatched Non-UP-ICU
Differences Between Patients With UP-ICU Event and Unmatched Controls
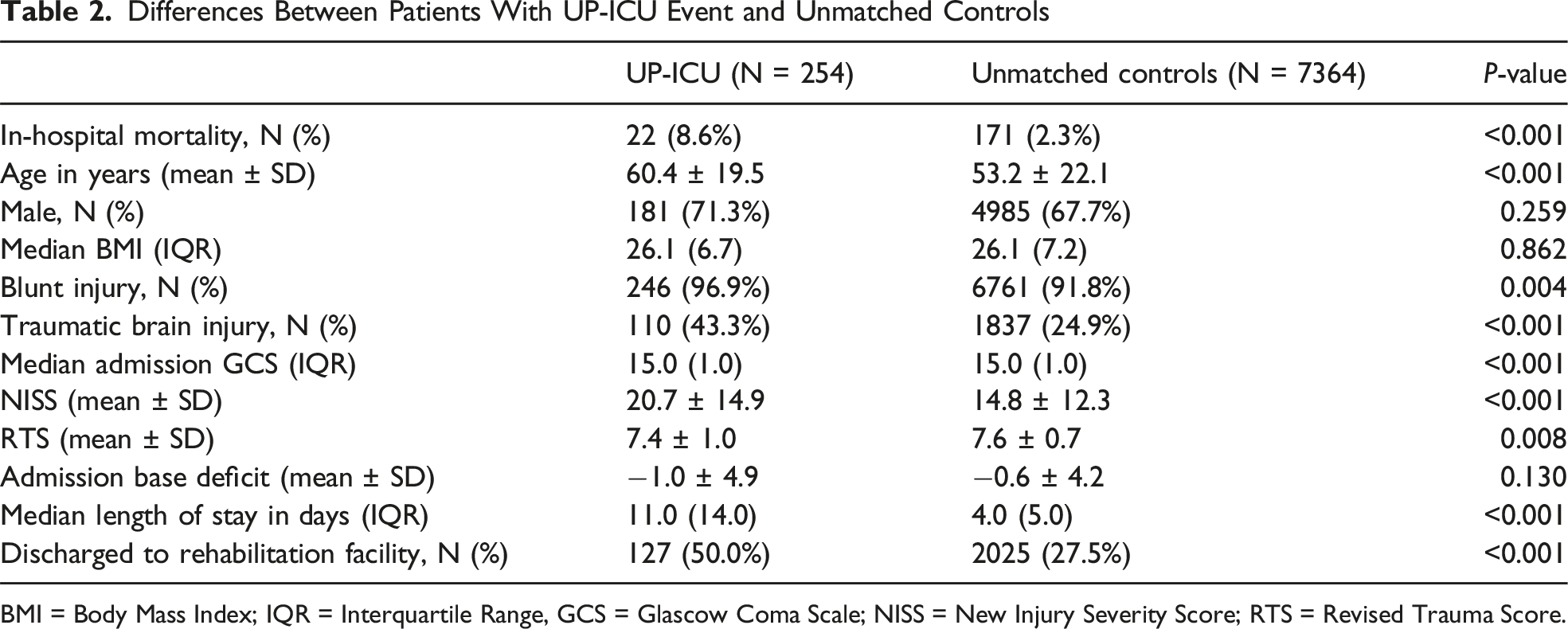
BMI = Body Mass Index; IQR = Interquartile Range, GCS = Glascow Coma Scale; NISS = New Injury Severity Score; RTS = Revised Trauma Score.
Among the 24 medical comorbidities considered, 13 met criteria for inclusion based on P-value threshold of 0.02 in our matching algorithm while the remaining were excluded from further analysis (Supplemental Table 1). Using these variables as well as the age, sex, admission base deficit, GCS, RTS, admission level of care, injury type, and NISS, we matched with our propensity score algorithm all 254 patients who had an UP-ICU event with a control patient in a 1:1 ratio. The exact values of each variable’s SMD along with other balance related assessments are shown in Supplemental Data Table 2.
UP-ICU Patients Compared to Matched Non-UP-ICU Cohort
Comparison of Patients With UP-ICU Event and Propensity Score Matched Controls
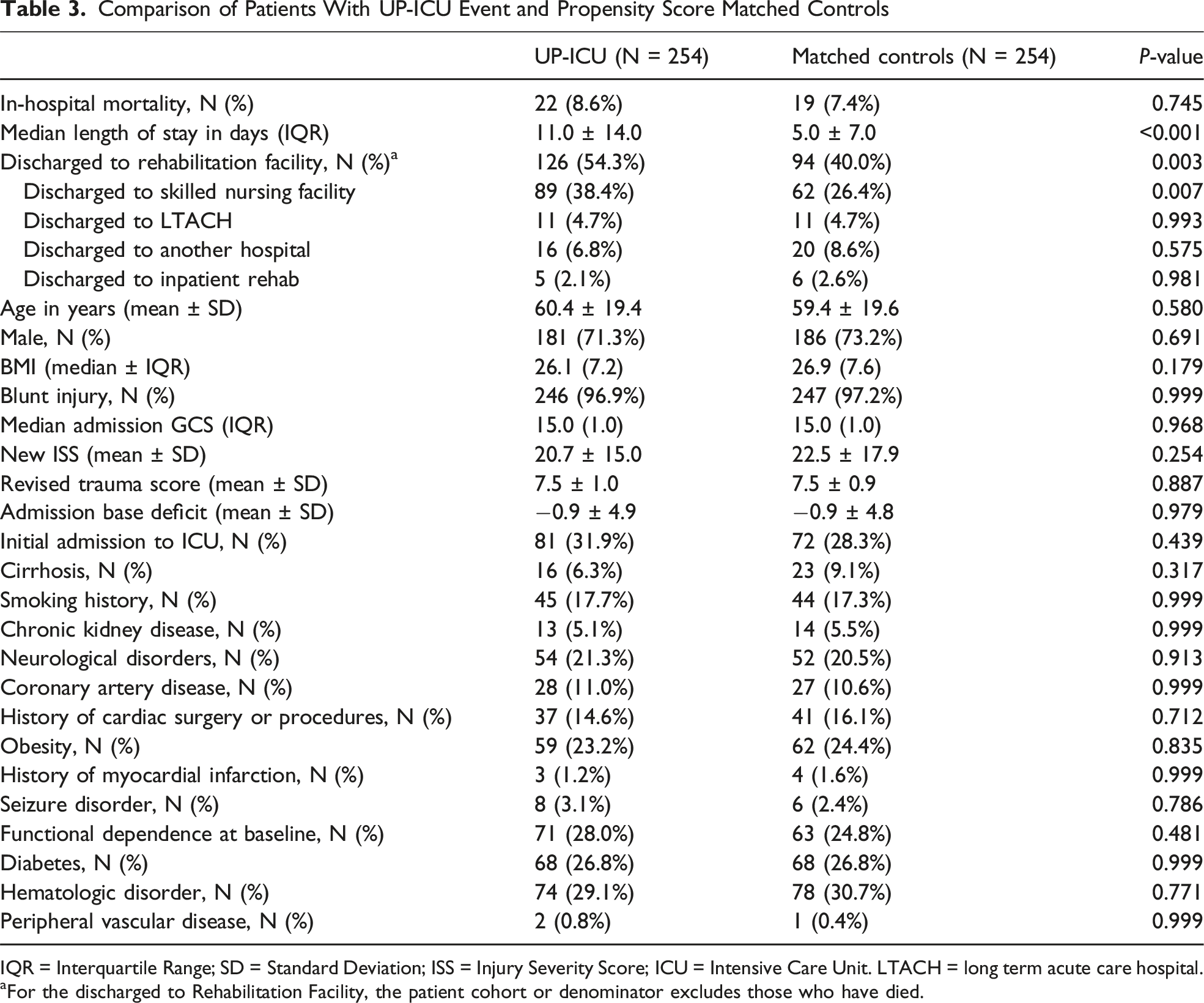
IQR = Interquartile Range; SD = Standard Deviation; ISS = Injury Severity Score; ICU = Intensive Care Unit. LTACH = long term acute care hospital.
aFor the discharged to Rehabilitation Facility, the patient cohort or denominator excludes those who have died.
Mortality After UP-ICU Event by Cause of UP-ICU
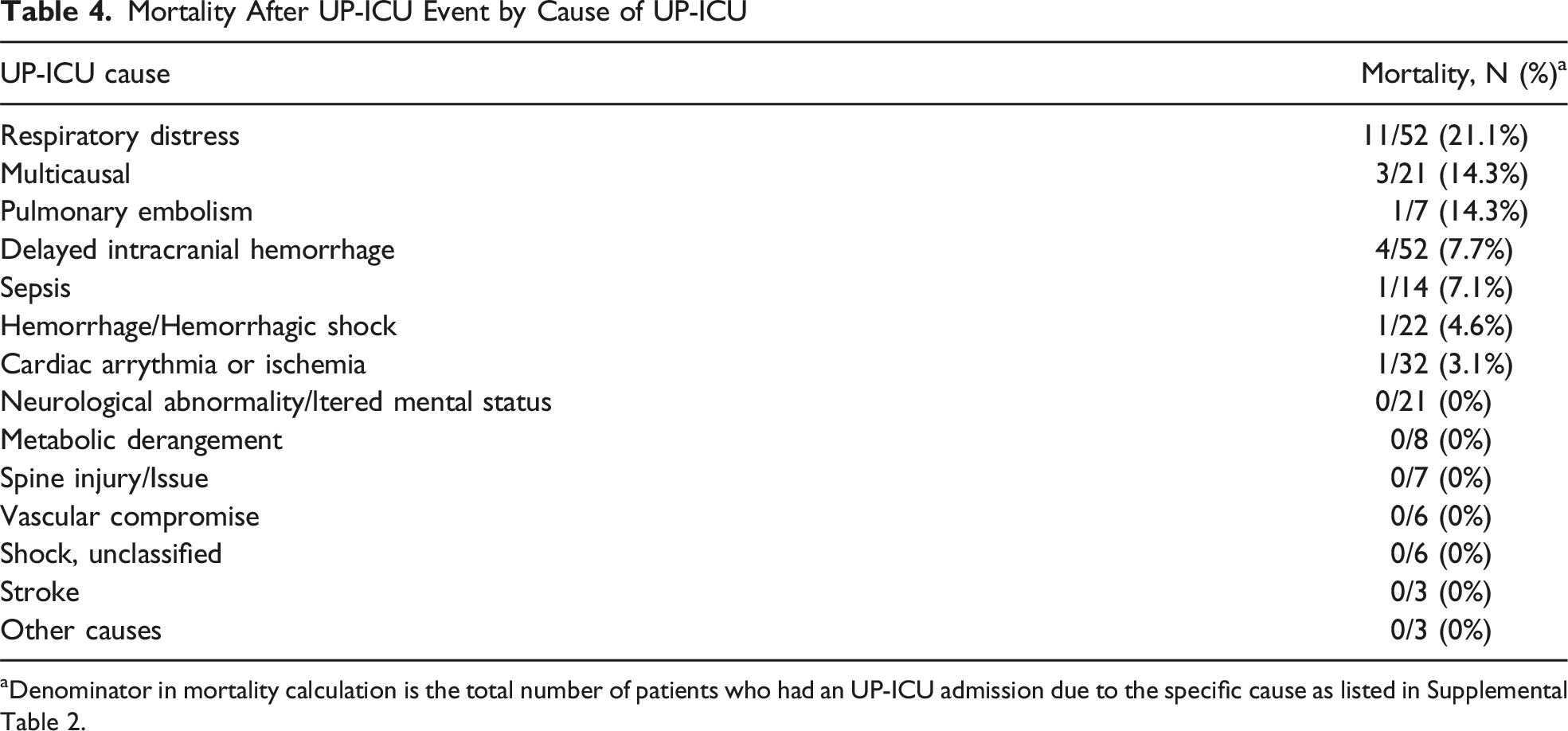
aDenominator in mortality calculation is the total number of patients who had an UP-ICU admission due to the specific cause as listed in Supplemental Table 2.
Discussion
In this study we call into question the concept that UP-ICU in trauma patients is associated with increased in-hospital mortality. After matching on the basis of patients’ baseline health and physiology on admission, which are unmodifiable factors, we demonstrated that there was no significant increase in mortality in the UP-ICU group compared to matched controls. Therefore, although mortality was similar between groups, UP-ICU may play an important role in reducing failure to rescue by facilitating earlier access to ICU level monitoring, resources, and interventions that enable patients to better survive acute deterioration.
UP-ICU is one of the many quality indicators adopted by ACS-TQIP to benchmark quality of care for trauma patients across health systems.1,5 These metrics were designed to help centers identify areas of improvement, and to allow for standardized evaluation of trauma programs by the ACS. 1 However, not all quality indicators effectively identify poor quality care. 12 While many TQIP indicators have been validated, the validity and applicability of some have been called into question.13,14
The UP-ICU metric was largely derived from the medical and surgical ICU literature demonstrating increased mortality associated with this occurrence.4,14 This has led some to accept that UP-ICU is a complication in trauma and by extension an indicator of quality. 15 Death after this event is then considered a failure to rescue (FTR) and a reflection of poor care as it is thought that high quality systems would minimize these events.15,16 However, the relationship between UP-ICU and mortality has been called in question for several reasons. First, it has been observed that for certain populations such as the elderly, more liberal parameters for upgrading to the ICU were associated with improved mortality. 17 In fact, hospitals that utilize rapid response algorithms with low thresholds for upgrading to the ICU for close monitoring have seen significant decreases in mortality and FTR, despite the higher UP-ICU admissions.18,19 Our study’s results are consistent with this as we found that most patients who had UP-ICU did not require any significant interventions including emergent operations, invasive procedures, vasopressor initiation, or intubations. Another criticism of the UP-ICU as a marker of FTR is that the event reflects the patient’s poor baseline physiology or underlying disease refractory to treatment rather than lack of quality care. 20 A recent study by Sangji et al (2022) showed equivalent UP-ICU rates among all mortality tiers of trauma centers, raising the question of whether UP-ICU is actually associated with mortality and FTR. 15
In trauma patients, the risk factors for UP-ICU identified in prior studies are unmodifiable and present on admission such as age, severe kidney, heart, and liver disease as well as injury severity, which are also noted risk factors for higher mortality. 3 UP-ICU and subsequent death in these high-risk patients may be based on these risk factors rather than the quality of care provided. Our results support this assertion as we found no significant difference in mortality after accounting for these risk factors. In addition, over 50% of patients who had an UP-ICU event did not require any invasive interventions such mechanical ventilation, vasopressor initiation, or emergency surgery within the first 24 hours. Therefore, our results suggest that UP-ICU is not independently associated with increased mortality and may even play a role in reducing FTR by facilitating early access to ICU-level monitoring and interventions.
Our results also suggest that UP-ICU patients had longer hospital length of stay than matched controls and were more frequently discharged to rehabilitation facilities (54.3% of UP-ICU patients vs 40% of matched controls, P < 0.001). Thus, the longer length of stay in UP-ICU patients likely reflects time required for stabilization and recovery rather than adverse outcomes. Many of these patients were ultimately discharged to rehabilitation facilities rather than long-term care.
Our study does not refute UP-ICU could, but instead in the right context and with cautious analysis may be a useful indicator of quality. We found that UP-ICU was associated increased discharge to rehabilitation facilities (54.3% of UP-ICU patients vs 40% of matched controls, P < 0.001), which may explain the longer length of stay in UP-ICU patients compared to matched controls. Thus, longer length of stay in UP-ICU patients likely reflects time required for stabilization and recovery rather than adverse outcomes. In addition, there is significant observed heterogeneity in causes of mortality among the UP-ICU group in that most death after UP-ICUs due to respiratory distress whereas mortality was much lower after other UP-ICU causes such as stroke or cardiac arrhythmias. Thus, focusing on UP-ICUs due to respiratory distress may yield opportunities for quality improvement as well.
This study should be interpreted with the following limitations in mind. First, our study was single center with a trauma step-down unit, so our results may not be generalizable to hospitals without a trauma step-down unit or with differing ICU admission policies and physician practices. Step-down units with experienced trauma-trained health care professionals may contribute to earlier detection of deterioration in trauma patients and reduce UP-ICU admissions and their associated mortality. Second, this was a retrospective study which limits the ability to discriminate between association and causation. Third, while we controlled for confounders that were available in the trauma registry, there are likely unknown confounders that were not incorporated into our variable selection process and were not accounted for in the matching algorithm. Fourth, due to inherent limitations of the data bank abstraction process, the medical comorbidities were abstracted as binary variables and do not account for severity of each disease or used to compute a composite score such as the Charlson Comorbidity Index. Fifth, because ACS-TQIP calculates benchmarks using rolling 6-month reporting cycles, indidual patients may contribute to multiple reporting cycles. Our study uses single-year registry data, so direct comparison of our results to TQIP rates may have limited comparability. Sixth, while we report rates of discharge to rehabilitation facilities, we were unable to evaluate other destinations such as skilled nursing facilities, LTACH, or hospice due to limited availability of data. Future studies should also stratify and assess early vs late UP-ICU admissions and examine these groups separately for differences in underlying causes and outcomes.
In summary, we demonstrate that mortality is comparable in trauma patients who experienced an UP-ICU event relative to a cohort matched on patient and illness related factors at the time of admission. Our results suggest that UP-ICU may not be associated with increased mortality and its use as a quality metric should be re-evaluated.
Supplemental Material
Supplemental Material - Rethinking the Unplanned ICU Admission Quality Metric in Trauma Patients
Supplemental Material for Rethinking the Unplanned ICU Admission Quality Metric in Trauma Patients by Zongyang Mou, MD, Parisa Oviedo, MD, Louis Perkins, MD, Todd W. Costantini, MD, Thomas O’Keefe, MD , Henry M. Horita, Jay J. Doucet MD, Laura N. Haines, MD, Jarrett E. Santorelli, MD in The American Surgeon™
Footnotes
Acknowledgments
The study authors would like to acknowledge Alan Smith, PhD, for their assistance in obtaining the necessary data for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ZM is supported by the National Library of Medicine Training Grant- NIH grant T15LM011271.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.