
Abstract
Introduction
A component of trauma-informed care (TIC) is providing opportunities for patients to share their stories and access healing resources. We introduced a “Trauma Survivor Rounds” (TSR) initiative to provide trauma patients an opportunity to discuss and receive individualized assistance. We evaluated whether they reported improved Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey scores, hypothesizing increased hospital recommendation rates following TSR implementation.
Methods
A single-center retrospective (2021-2023) analysis of admitted trauma patients with HCAHPS survey responses was conducted. The HCAHPS survey measures patient experience, satisfaction, and health care quality. Pre-TSR (1/1/2021-12/31/2021) (PRE) and post-TSR (1/1/2022-12/31/2023) (POST) cohorts were compared. In TSR, a medical student discussed trauma and assisted patients obtain resources. The primary outcome was whether patients recommended the hospital on the HCAHPS survey.
Results
Of 348 patients, 133 (38.2%) were in the POST cohort. Hospital recommendation rates were statistically similar: “definitely yes” (POST: 82.9% vs PRE: 78.3%), “probably yes” (POST: 15.4% vs PRE: 14.0%), “probably no” (POST: 1.7% vs PRE: 4.3%), and “definitely no” (POST: 0% vs PRE: 3.4%) (P = 0.12). No significant difference was found in the overall hospital ratings. Notably, more POST patients reported receiving help “as soon as wanted” (61.4% vs 54.7%, P < 0.001).
Conclusions
Implementation of a TIC-based TSR program showed no statistically significant difference in hospital recommendations or ratings; however, it was associated with more patients reporting receiving help “as soon as wanted.” Larger sample size studies are needed to determine whether this approach improves HCAHPS scores or other quality metrics.
• TSR programs may improve patient responsiveness and experience, even without significant changes in overall hospital ratings. • Effective trauma-informed care requires systemic support, including leadership and staff training, to impact patient satisfaction.Key Takeaways
Introduction
Trauma patients experience both physical and psychosocial injuries, often requiring a comprehensive approach to care that addresses their complex needs. 1 Trauma-informed care (TIC) focuses on recognizing and responding to the effects of trauma by creating environments that promote healing, safety, and patient empowerment. One key element of TIC is enabling patients to share their experiences and facilitating access to resources to support recovery. 2 Despite growing recognition of TIC principles, its direct impact on patient-reported outcomes, such as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey scores, remains unknown.3,4
These scores are crucial not only for assessing the quality of care but also for influencing health care funding and reputation. 5 While trauma care traditionally prioritizes physical recovery, limited attention has been given to interventions that improve patient satisfaction and psychosocial outcomes.6,7 To address these gaps, we implemented “Trauma Survivor Rounds” (TSR), an initiative designed to provide trauma patients with opportunities to share their experiences and receive personalized support. Previous studies have found improved patient-reported outcomes with similar psychosocial interventions.2,8 However, it is unclear how this affects HCAHPS survey results.
Therefore, this study aimed to investigate the impact of TSR on HCAHPS survey results by comparing scores before and after its implementation. We hypothesized that TSR would enhance patient experiences, leading to improved satisfaction scores and a greater likelihood of patients recommending the hospital.
Methods
This study was approved by the Institutional Review Board (IRB), with a waiver of informed consent due to the use of deidentified data. A single-center retrospective analysis was conducted on trauma patients admitted to a single Level-I trauma center between January 2021 and December 2023 who completed the HCAHPS survey. The HCAHPS survey, developed by the Centers for Medicare & Medicaid Services and the Agency for Healthcare Research and Quality in 2006, is a nationally standardized instrument designed to measure adult inpatients’ perceptions of their hospital experience across key domains such as provider communication, responsiveness, discharge information, and overall satisfaction. The HCAHPS survey is distributed to a random sample of discharged patients via mail, telephone, or interactive voice recognition. The survey consists of 29 questions, and responses were collected in a standardized and consistent fashion to ensure data comparability. These patients were grouped into pre-TSR (PRE) (January 1, 2021-December 31, 2021) and post-TSR (POST) (January 1, 2022-December 31, 2023) cohorts. Medical students in their 2nd to 4th year participated in the TSR program on a voluntary basis, separate from their formal trauma surgery rotation. A small, rotating cohort was selected based on availability and interest. Medical students represent a cohort of medically educated and highly engaged health care workers. All participants completed standardized training that included a one-hour didactic session and a small-group workshop covering TIC principles, psychological responses to injury, and motivational interviewing. Students were also introduced to available hospital- and community-based resources, provided contact information for the on-call social worker and trauma team, and received guidance on common patient questions, with support readily available from the trauma team or social worker if they received questions they could not answer. TSR sessions typically occurred twice per week, though frequency varied depending on student availability, and were initiated once patients were deemed stable by the trauma team, who would interact with the students beforehand. Each session began with an introduction and an offer to talk, inviting patients to share their experiences and concerns at their own pace. Students discussed emotional wellbeing, coping, and safety, and offered information about available support services. Nurses and other ancillary staff were informed and involved as needed. The TSR program ran continuously throughout the study period, with trauma attendings and residents assisting with patient identification and supporting student engagement.
Services for post-traumatic stress disorder and depression screening, peer mentoring, and food or housing were also provided. The PRE cohort was compared to the POST cohort. Only patients who did not respond to HCAHPS surveys were excluded from the analysis. In the PRE cohort, 215 of 699 surveyed patients returned the HCAHPS survey (30.8% response rate), and in the POST cohort, 133 of 473 surveyed patients returned the survey (28.1% response rate).
The primary outcome was the rate of patients recommending the hospital on the HCAHPS survey. Secondary outcomes included the overall hospital rating and scores for specific care aspects such as receiving help “as soon as wanted.” Demographic variables collected included race, ethnicity, the highest school degree completed, and the language mainly spoken at home, as these are available in the HCAHPS survey. Additional variables collected in the survey include admission through the emergency room (ER), the unit from which the patient was discharged (ie, intensive care unit (ICU), step down/telemetry, or floor), and whether patients were given medications not taken before.
Bivariate statistical analyses included Mann-Whitney U tests for continuous variables and Pearson’s chi-squared tests for categorical variables. Continuous variables were reported as medians with interquartile ranges, and categorical variables as frequencies. For the primary outcome (“definitely yes” hospital recommendation), we also performed a post-hoc power analysis using realized sample sizes to calculate achieved power, the minimum detectable effect, and the sample size required to detect a clinically meaningful difference. Power calculations used two-sample z tests for proportions with normal-approximation methods (α = 0.05, two-sided).
With realized denominators (PRE 162/207 [78.3%], POST 97/117 [82.9%]), the absolute difference was +4.6 percentage points (95% CI −4.4 to +13.6; P = 0.32). Post-hoc achieved power to detect this difference with α = 0.05 (two-sided) was 17%. Given our sample sizes, the minimum detectable effect was 12.3 percentage points at 80% power (14.0 at 90%). For future planning, detecting a 5-point absolute improvement with 80% power would require approximately 975 respondents per cohort (balanced).
All analyses were two-sided and were performed using IBM SPSS Statistics (version 29; IBM Corp., Armonk, NY).
Results
Admission Characteristics and Demographics for the PRE vs POST Cohorts
Discharge Units of the PRE vs POST Cohorts
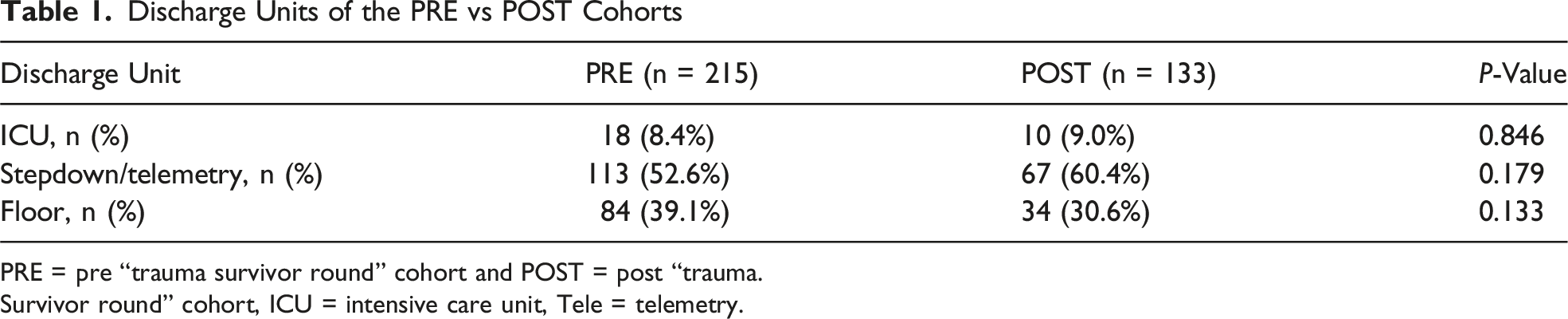
PRE = pre “trauma survivor round” cohort and POST = post “trauma.
Survivor round” cohort, ICU = intensive care unit, Tele = telemetry.
Demographics and Characteristics of the PRE vs POST Cohorts
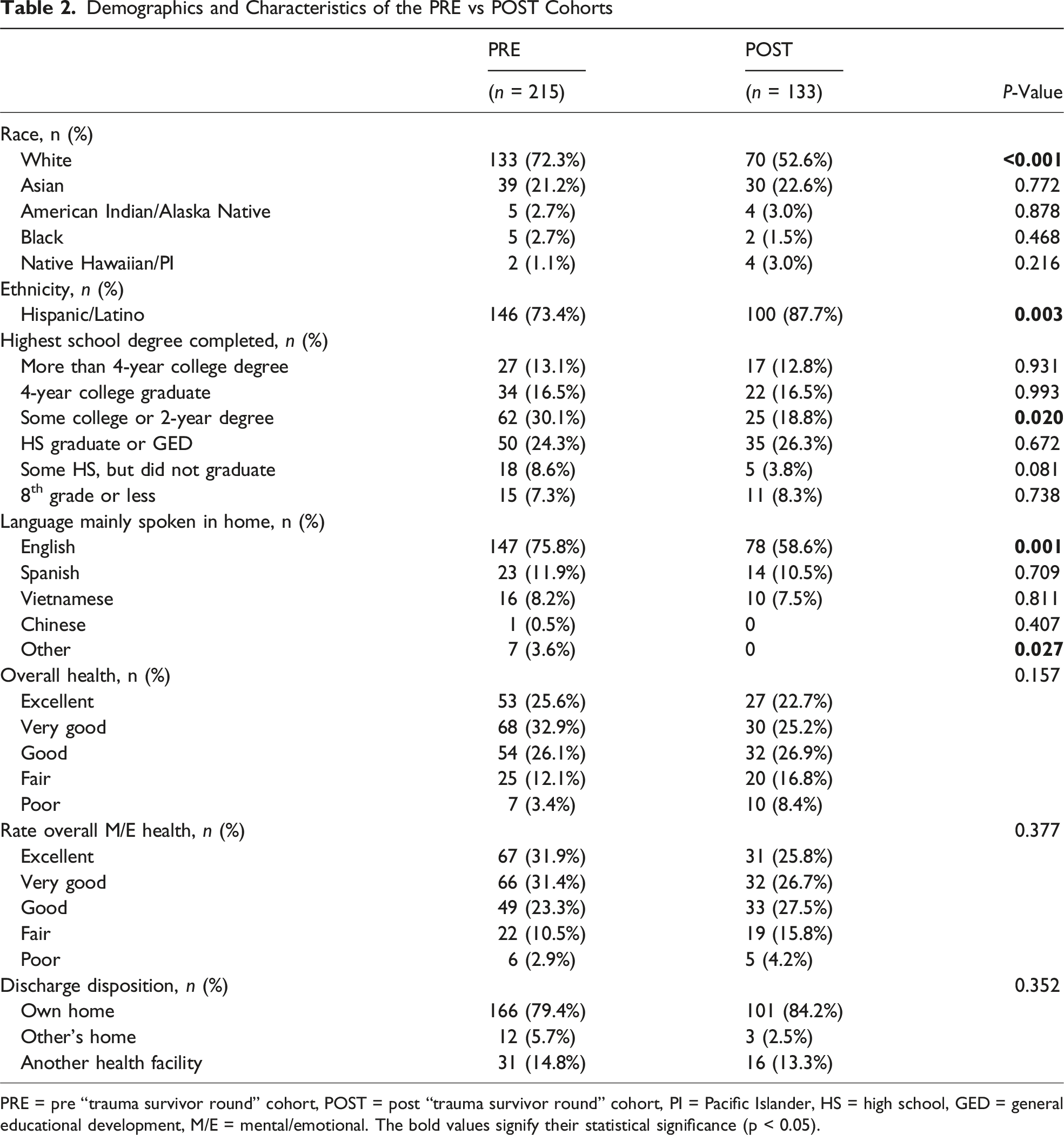
PRE = pre “trauma survivor round” cohort, POST = post “trauma survivor round” cohort, PI = Pacific Islander, HS = high school, GED = general educational development, M/E = mental/emotional. The bold values signify their statistical significance (p < 0.05).
HCAHPS Survey Responses for the PRE vs POST Cohorts
HCAHPS Survey Responses of the PRE vs POST Cohorts
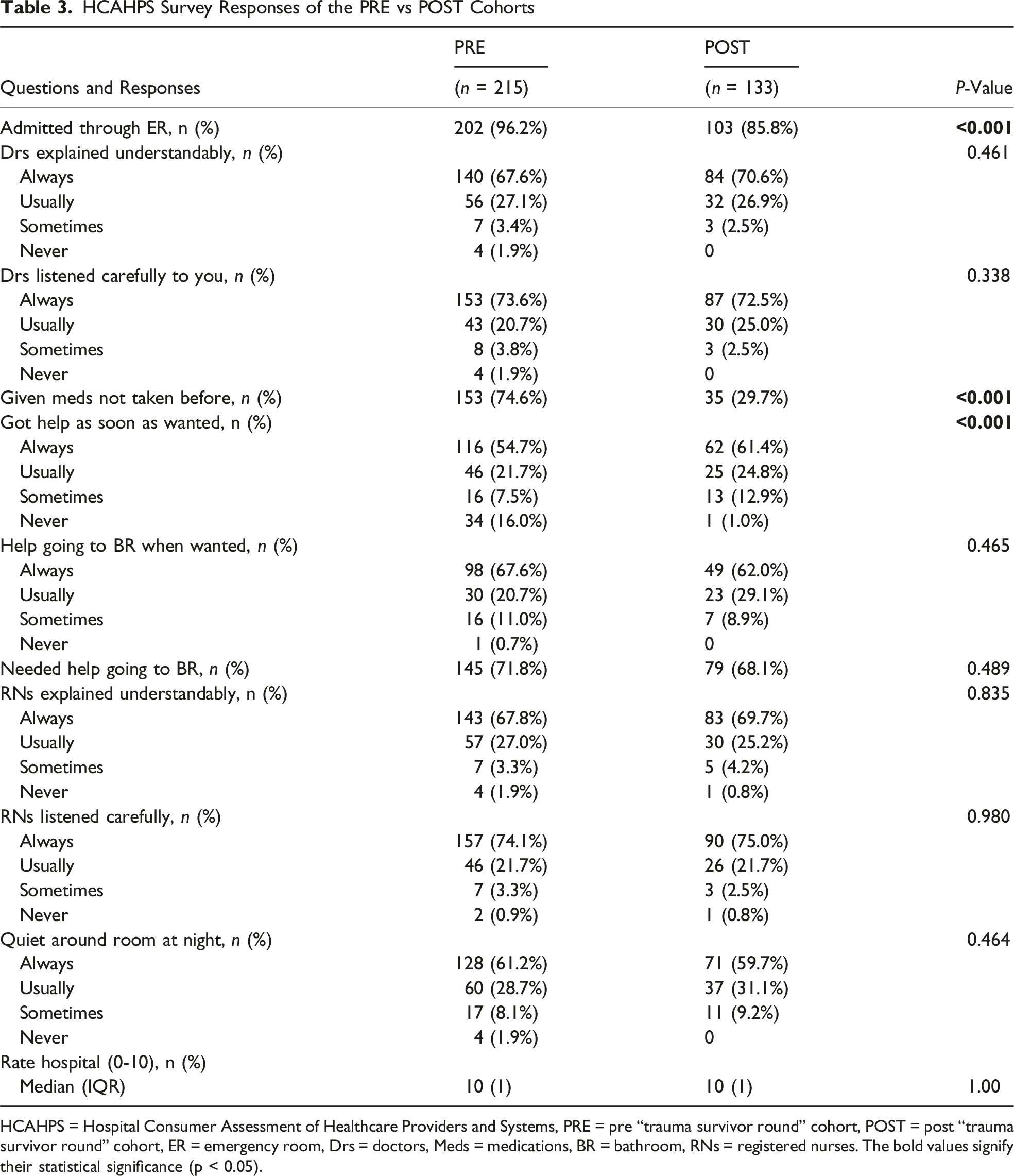
HCAHPS = Hospital Consumer Assessment of Healthcare Providers and Systems, PRE = pre “trauma survivor round” cohort, POST = post “trauma survivor round” cohort, ER = emergency room, Drs = doctors, Meds = medications, BR = bathroom, RNs = registered nurses. The bold values signify their statistical significance (p < 0.05).
HCAHPS Survey Responses of the PRE vs POST Cohorts
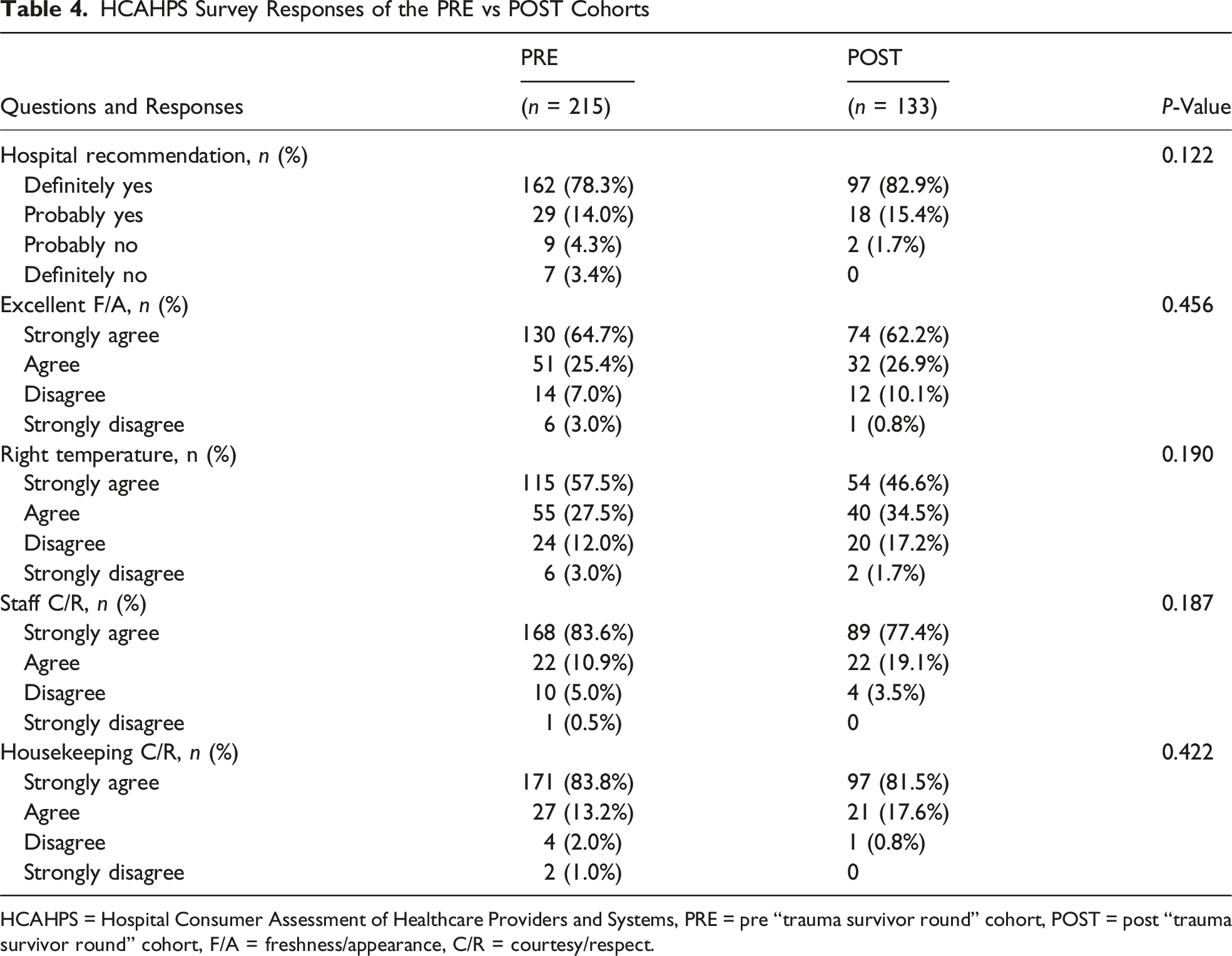
HCAHPS = Hospital Consumer Assessment of Healthcare Providers and Systems, PRE = pre “trauma survivor round” cohort, POST = post “trauma survivor round” cohort, F/A = freshness/appearance, C/R = courtesy/respect.
Discussion
TIC is a growing effort within the trauma community aimed at improving the patient recovery process. 9 This study evaluated the impact of a TSR program, grounded in TIC principles, on patient satisfaction as measured by HCAHPS surveys. Although hospital recommendation rates showed modest improvement after implementation, the differences did not reach statistical significance. However, the POST cohort had a significant increase in patients reporting receiving help “as soon as wanted,” suggesting a potential positive impact of this program. While prior studies have examined peer-support programs and patient navigation as means to improve patient experience, TSR differs by incorporating real-time, structured interactions during hospitalization. In addition to its impact on patient outcomes, TIC has been associated with improvements in staff morale, reductions in burnout, and enhanced team cohesion.2,4 While these outcomes were not directly measured in our study, it is possible that the TSR program contributed to a more supportive care environment. Future studies may explore the system-level and staff-related impacts of such programs to fully capture their value.
Hospital ratings remain an industry-wide recognized metric of quality, 10 and some evidence suggests that HCAHPS scores correlate with patient outcomes as well. 11 Regardless of this association, patient experience and patient-reported outcomes (PROs) align with TIC principles and are increasingly evaluated in health care. Prior research indicates that TIC implementation requires systemic integration and sustained effort to achieve meaningful outcomes.12,13 Huo et al noted that organizational readiness, staff training, and leadership are critical enablers for TIC success, and their absence can limit the impact of interventions. 14 Similarly, Greenwald et al emphasized the need for cohesive strategies encompassing direct care, administrative practices, and environmental adjustments to enhance patient experiences. 15 While our study failed to show a statistically significant improvement in hospital recommendation rates, this may be due to the presence of a Type II error from a lack of power. There did appear to potentially be a trend for improvement, and unlike scientific research, any increase in patient satisfaction is desirable for the hospital, as small differences in scores may alter hospital rankings/ratings. 16 Future larger prospective multicenter studies are needed to definitively evaluate the efficacy of a TSR program in terms of its effect on HCAHPS.
Responsiveness to patients is increasingly challenging in an electronic medical record dominated health care system. 17 In addition, providers are task saturated with non-clinical efforts, including clinical documentation integrity and billing. 18 Thus, the significant improvement in responsiveness demonstrated in this study may reflect the additional resource of a skilled and helpful person (the medical student) being at bedside to help patients address global concerns, non-immediate health questions, and/or provide information for available outpatient resources. Alternatively, this could reflect increased institutional awareness or other efforts, although there were no major ongoing programs within our hospital specifically related to this during the study period. Fernández et al previously reported that targeted TIC-based interventions frequently yield localized improvements in service delivery, even when overall satisfaction scores remain unchanged. 19 The observed improvement in our study suggests that structured, patient-centered engagement programs such as TSR may serve as a low-cost, scalable intervention to enhance patient experience. Given that responsiveness is a key HCAHPS metric, hospitals may consider incorporating similar programs to improve quality scores, although future qualitative research is needed to confirm the exact reason for our findings.
Limitations
This study has several limitations inherent to its retrospective single-center design, including potential missing data and reliance on self-reported HCAHPS survey responses, which may introduce bias and inaccuracies. The small sample size, particularly in the POST cohort, limits statistical power and generalizability, especially given the known challenges in achieving robust response rates in trauma populations. In addition, HCAHPS does not capture important aspects of TIC such as psychological safety and trust between patients and their care team. Future research may benefit from the development and incorporation of other tools to measure these important outcomes. As a single-center study, findings may not be generalizable to other institutions with differing patient demographics or trauma care practices. The reliance on standardized survey data also lacks granularity to assess the nuanced impact of TSR on individual trauma recovery. Additionally, HCAHPS survey responses could not be linked to the trauma registry, limiting our ability to analyze patient demographics, injury characteristics, or clinical outcomes for the surveyed cohort. As such, key clinical variables known to influence satisfaction, including trauma severity, length of stay, and ICU admission, were not adjusted for in our analysis and merits future prospective research. Furthermore, the retrospective nature of the study prevents causal inference, as unmeasured factors or concurrent initiatives may have influenced results. Finally, the demographic differences between cohorts and lack of data on social determinants of health, known to affect both satisfaction and recovery, 20 should be noted.
Conclusion
This study evaluated the impact of a TSR program on HCAHPS at a single Level-I trauma center. There was no significant difference in hospital ratings in the POST cohort compared to the PRE cohort; however, in terms of hospital recommendation rates, the POST cohort had an increased rate of patients responding, “definitely yes” and “probably yes,” and fewer responding “probably no” or “definitely no,” though this was not statistically significant. Future prospective multicenter studies are needed to determine whether more comprehensive, system-wide TIC approaches can improve HCAHPS survey results.
Footnotes
Ethical Considerations
This study was deemed exempt by our Institutional Review Board.
Consent to Participate
Written informed consent was waived as this study used a national deidentified database.
Author Contributions
The authors contributed to this work as follows:
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.