
Abstract
Background
Severe lower extremity injuries in pediatric patients present significant challenges for surgeons deciding between repair and amputation. A novel scoring system, the MangLE score, has been developed to identify adult patients who are unlikely to require amputation after severe lower extremity injury. This study sought to evaluate the predictive ability of the MangLE score in pediatric patients.
Methods
A retrospective analysis was conducted using the 2013-2021 American College of Surgeons Trauma Quality Improvement Program (TQIP) database. Pediatric patients (≤17 years) with mangled lower extremities were included. Patients were stratified into age groups (0-3, 4-9, 10-13, and 14-17 years), and the predictive ability of the MangLE score for lower extremity amputation was assessed based on the area under the receiver operating characteristic curve (AUC), sensitivity, and specificity.
Results
A total of 7959 patients met the inclusion criteria. The MangLE score demonstrated an excellent predictive capability in patients aged 10-13 (AUC (95% CI): 0.87 (0.79-0.94)) and 14-17 (AUC (95% CI): 0.83 (0.79-0.86)). At the cutoff of ≥8, this resulted in an NPV of 99.7% for 10-13-year-olds and 99.4% for 14-17-year-olds. However, the MangLE score was ineffective in discriminating between those who did and did not require a lower extremity amputation in patients between 0 and 9 years old.
Discussion
The MangLE score maintains an excellent predictive ability for identifying those unlikely to require lower extremity amputation in pediatric mangled extremity patients aged 10-17; however, it fails to accurately predict this outcome in younger patients.
Level of Evidence
Level IV.
Key Takeaways
• The MangLE score exhibited excellent predictive capability for identifying pediatric patients aged 10 to 17 years who are unlikely to necessitate lower extremity amputation. • The score demonstrated suboptimal performance in children under 10 years old, underscoring age-related disparities in its clinical applicability. • The findings indicate that although the MangLE score provides advantages for older pediatric patients, alternative or adjusted scoring methods may be necessary for younger children.
Introduction
Severe lower extremity injuries in pediatric patients present significant challenges for surgeons in determining whether to pursue limb salvage or delayed amputation. 1 Mangled lower limbs are characterized by complex fractures, severe soft tissue damage, nerve injury, and impaired vascular integrity. 2 Age greatly impacts trauma outcomes, as younger children have distinct injury patterns and physiologic reserve compared to adults.3,4 As age increases, limb injuries are more prevalent while head injuries are less common. 3 Nevertheless, limb injuries remained the most frequently observed injury type across all pediatric age groups. 3
The Mangled Extremity Severity Score (MESS) has traditionally been employed to evaluate the probability of limb preservation in both adult and pediatric cohorts5-10; however, its application in children is controversial, as the distinct physiological and healing capacities of pediatric patients must be taken into account along with the development of new techniques for limb salvage in the pediatric population.11-14 Children exhibit superior outcomes in nerve repair, better fracture healing rates, and reduced wound infection occurrences, particularly due to advancements in microsurgical salvage employing free tissue transfer for soft tissue defects. Furthermore, their enhanced cortical plasticity enables more effective adaptation to limb injuries.11,15-17
A novel scoring system, the Mangled Lower Extremity (MangLE) score, has been developed to identify patients who are unlikely to require amputation after severe lower extremity injury, enabling the allocation of limb salvage resources to this group. 18 Nonetheless, the prognostic ability of the MangLE score for lower extremity amputation in pediatric trauma patients has not yet been investigated. The efficacy of predictive scoring systems may differ with age, warranting more examination of their clinical utility among pediatric subpopulations. Consequently, this study sought to evaluate the predictive ability of the MangLE score in pediatric patients using data from the American College of Surgeons Trauma Quality Improvement Program database. We hypothesized that the MangLE score can be used to identify pediatric patients who are unlikely to require amputation following a mangled extremity injury.
Methods
Since the present study utilized an anonymized, retrospective data set for all analyses, the pertinent institutional review board exempted the requirement for ethical approval. The study complied with the Declaration of Helsinki and followed the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines. Data were obtained from the 2013-2021 American College of Surgeons Trauma Quality Improvement Program (TQIP) data set. All pediatric patients (≤17 years old) admitted with a mangled lower extremity were included. A mangled lower extremity was defined as a crush injury, or a fracture of the femur or tibia combined with severe soft tissue injury, arterial injury, and/or nerve injury. 18 The same injury codes utilized in the original development and validation study were applied. 18 Patients were excluded if they sustained a traumatic lower extremity amputation, underwent surgical amputation within 24 hours of admission, or died within 24 hours of admission.
Statistical Analysis
Patients were categorized into 4 developmental age groups: infants/toddlers (0-3 years), preschool/young children (4-9 years), preadolescents (10-13 years), and adolescents (14-17 years). Continuous variables were presented as means with standard deviations (SDs) or medians with interquartile ranges (IQRs), depending on the distribution of each variable. Statistical comparisons between cohorts were conducted using the Student’s t-test for normally distributed data and the Mann-Whitney U-test for non-normally distributed data. Categorical variables were summarized as counts and percentages, with significance testing performed using the Chi-squared test or Fisher’s exact test, as appropriate. The primary outcome was lower extremity amputation.
Mangled Lower Extremity (MangLE) Score
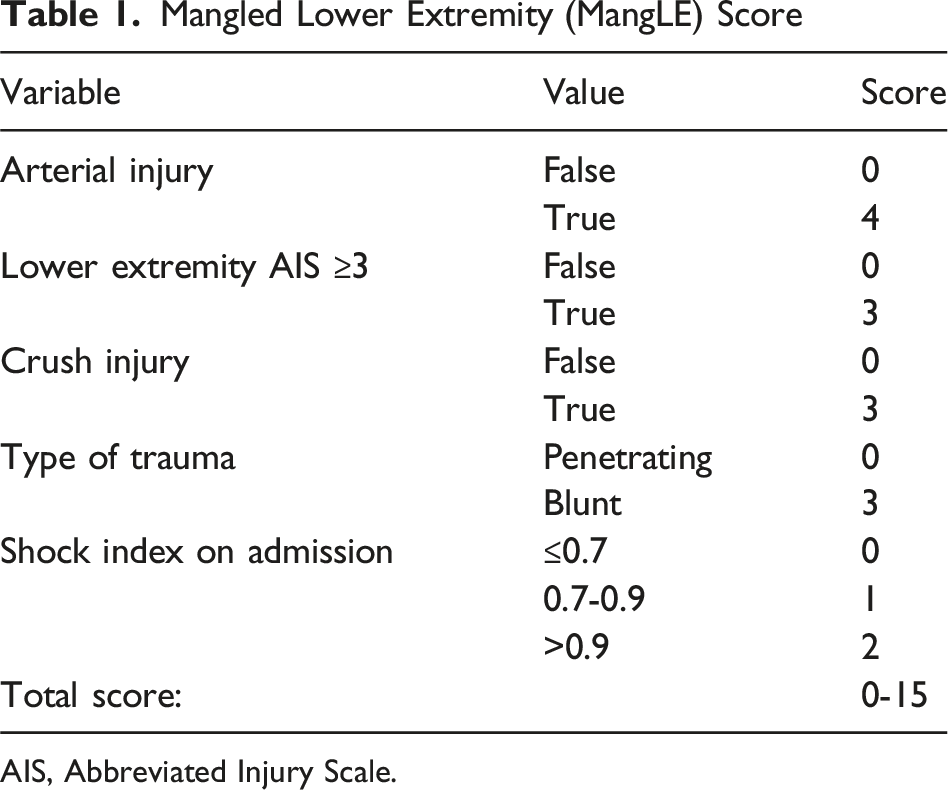
AIS, Abbreviated Injury Scale.
Statistical significance was defined as a two-sided P-value <0.05. Missing data were handled using multiple imputation by chained equations. All analyses were conducted in R (R Foundation for Statistical Computing, Vienna, Austria) utilizing the tidyverse, parallel, pROC, and mice packages.
Results
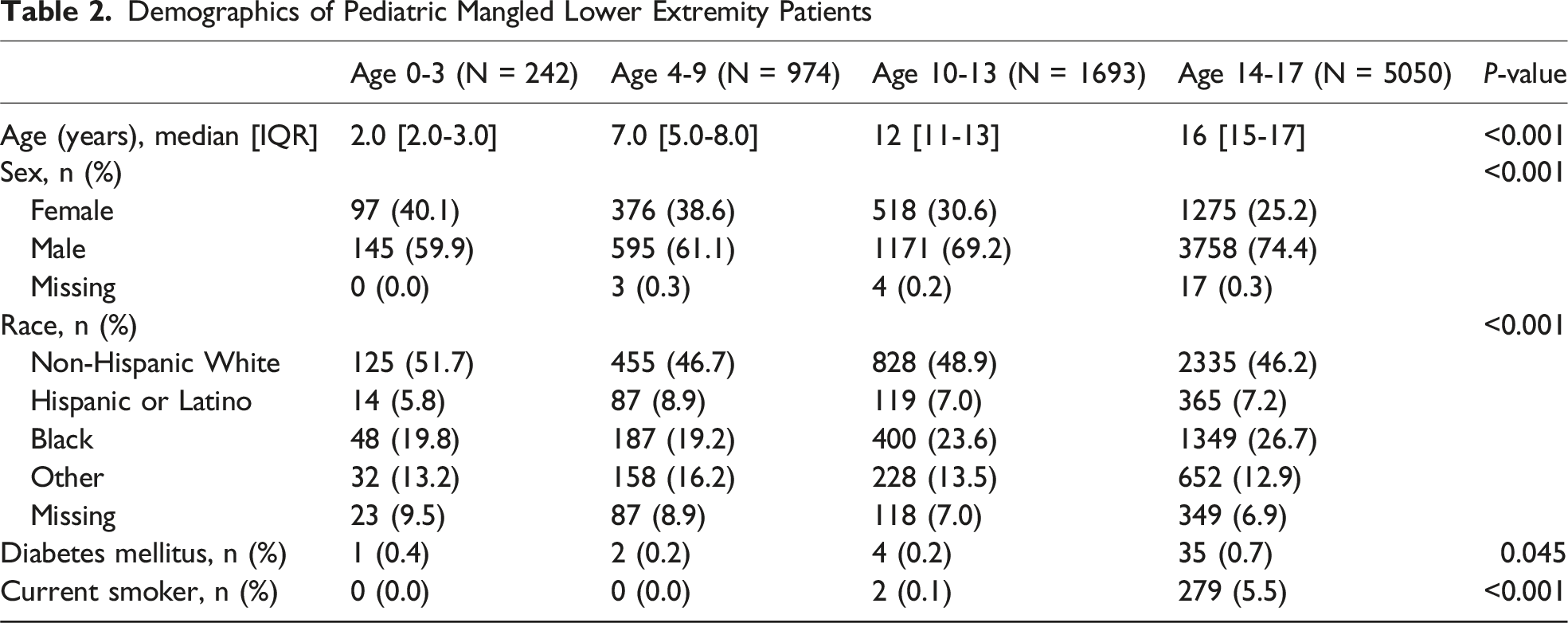
Demographics of Pediatric Mangled Lower Extremity Patients
Clinical Characteristics of Pediatric Mangled Lower Extremity Patients
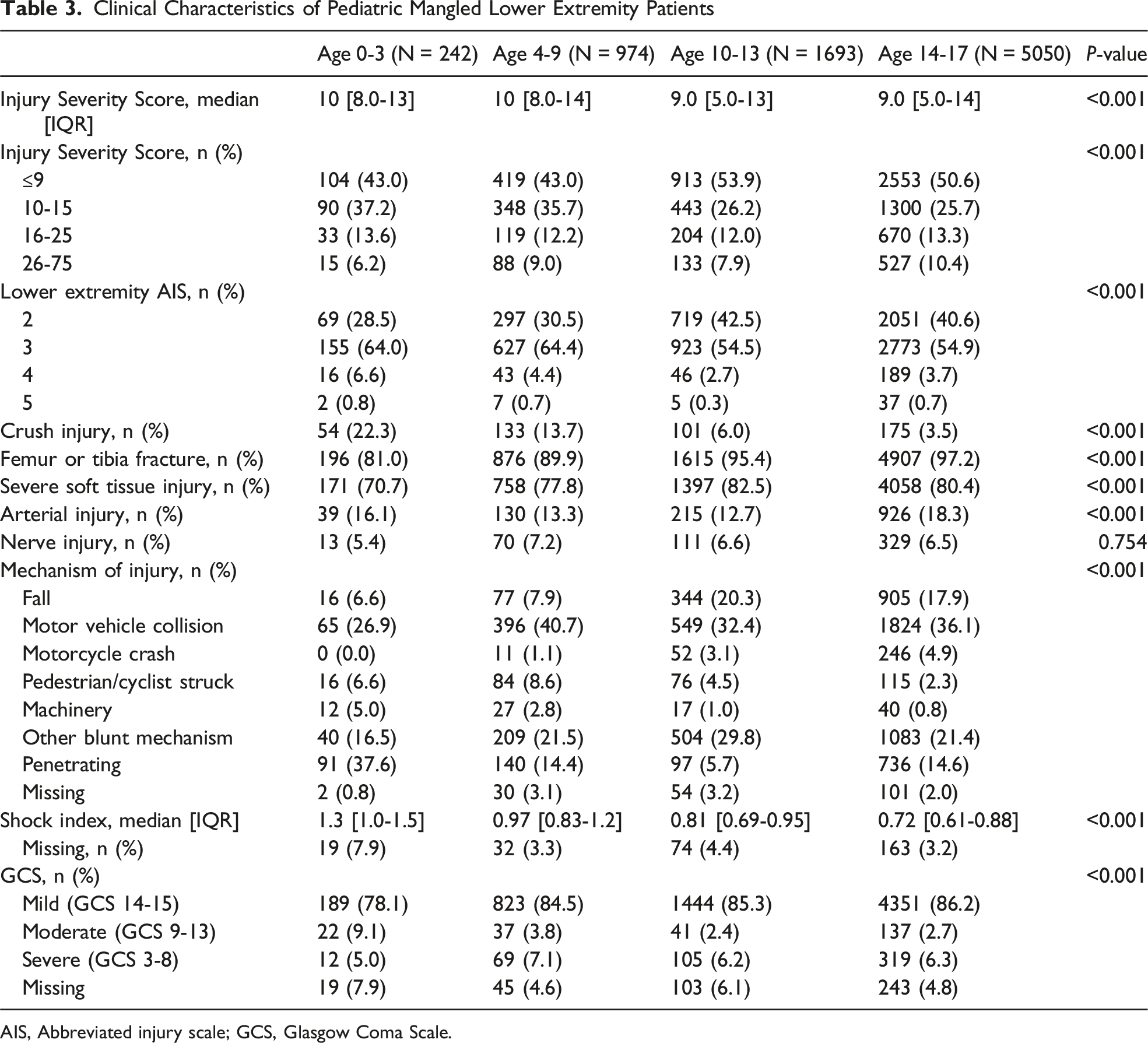
AIS, Abbreviated injury scale; GCS, Glasgow Coma Scale.
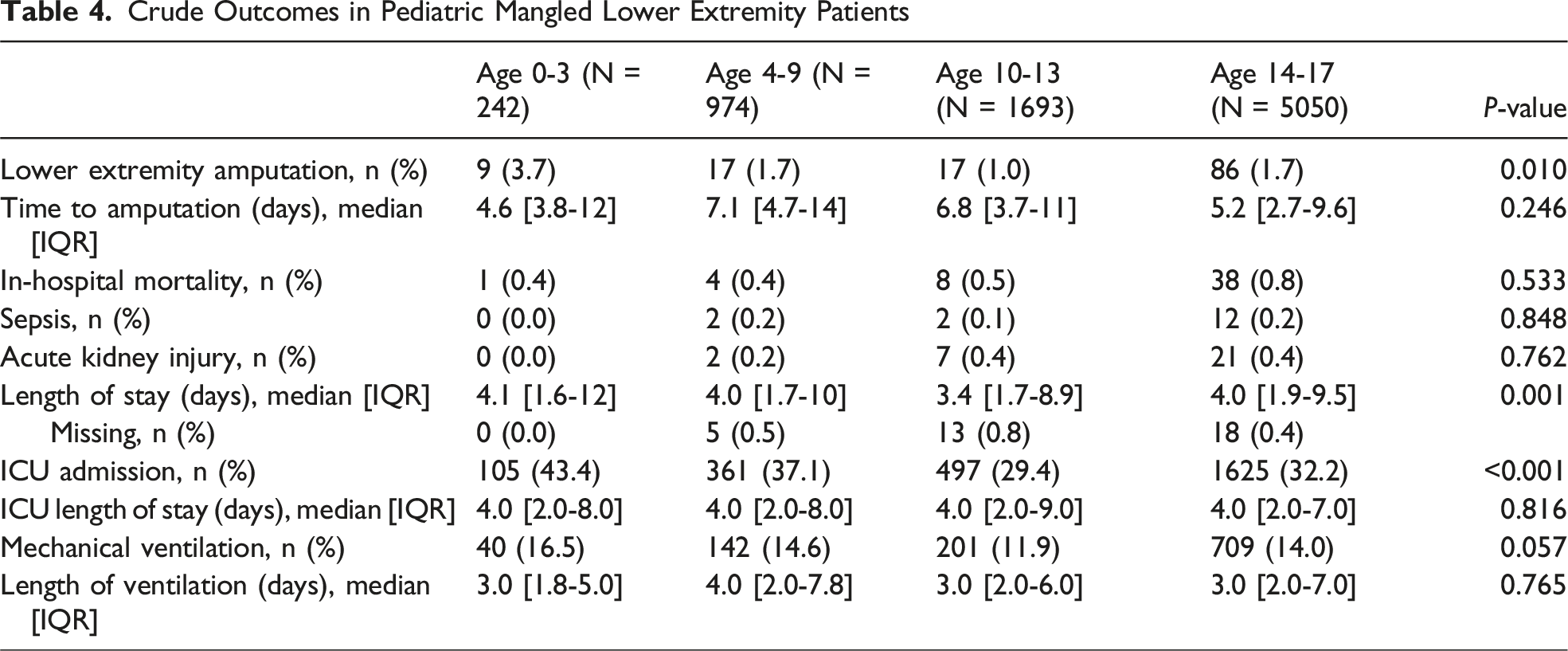
Crude Outcomes in Pediatric Mangled Lower Extremity Patients
Predictive Ability of the MangLE Score for Pediatric Lower Extremity Amputation
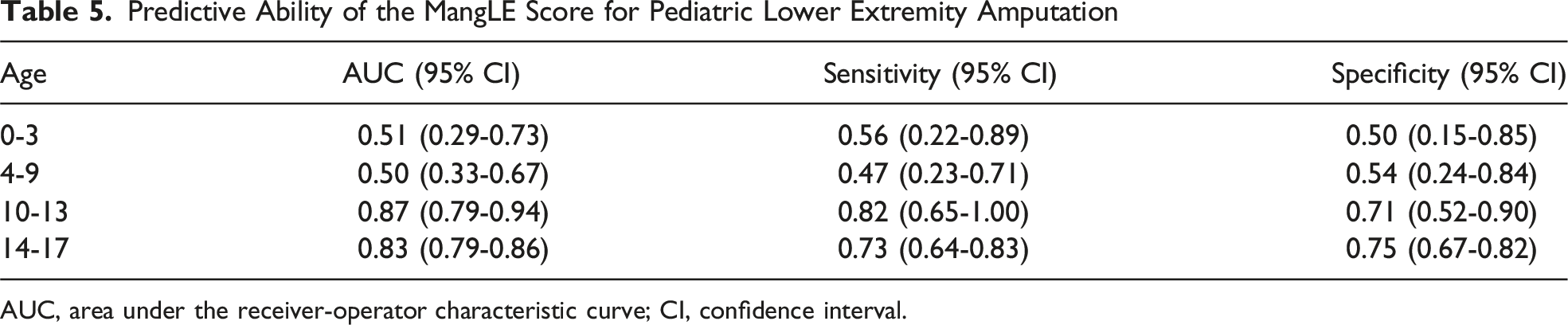
AUC, area under the receiver-operator characteristic curve; CI, confidence interval.
Discussion
The current investigation of 7959 pediatric patients with mangled lower extremities indicated significant age-related differences in injury patterns, comorbidities, and outcomes. Patients aged 0-3 years demonstrated more severe lower extremity injuries (AIS ≥3), with increased incidences of crush injuries, ICU admissions, and penetrating trauma. Conversely, older patients (14-17 years old) exhibited a higher incidence of tibia and femur fractures, serious soft tissue injuries, and were more frequently injured in falls or motor vehicle accidents. The MangLE score was able to achieve an excellent predictive ability for discerning patients unlikely to require lower extremity amputation among those aged 10-17; however, it struggled when attempting to predict lower extremity amputation in the young cohorts. 19
Compared to the adult patients in the study that developed the MangLE score, pediatric mangled lower extremity patients demonstrated similar rates of crush injury (5.8% vs 4.8%), femur or tibia fracture (95.4% vs 96.8%), severe soft tissue injury (80.2% vs 81.6%), arterial injury (16.4% vs 16.1%), and nerve injury (6.6% vs 4.7%). 18 However, pediatric patients were half as likely to undergo lower extremity amputation (1.6% vs 2.5%) and were significantly less likely to die during the hospital stay (0.6% vs 1.8%). In the initial study, the MangLE score displayed an excellent predictive capability with an AUC of 0.81 (95% CI: 0.80-0.82) in the development data set and an AUC of 0.82 (95% CI: 0.81-0.84) in the validation data set. 18 This corresponded to an NPV of 99.2% at a cutoff of ≥8. In the current analysis, the MangLE score demonstrated a similarly excellent predictive ability for lower extremity amputation in older children aged 10-13 years (AUC (95% CI): 0.87 (0.79-0.94)) and 14-17 years old (AUC (95% CI): 0.83 (0.79-0.86)). At the same cutoff of ≥8, this resulted in an NPV of 99.7% for 10-13 year-olds and 99.4% for 14-17 year-olds. The MangLE score consequently appeared to retain its predictive ability in pediatric mangled extremity patients between the ages of 10 and 17. However, it was ineffective in predicting amputations in those between 0 and 9 years old.
The inferior performance of the MangLE score in younger children may in part be attributable to the inclusion of the shock index. Due to physiological differences between pediatric and adult patients, pediatric patients have a naturally higher heart rate and lower blood pressure resulting in an increased shock index. 20 The MangLE score does not account for this, leading to patients with physiologically normal vitals on admission being classified as being at an increased risk of lower extremity amputation. Nonetheless, the elimination of the shock index from the score does not significantly enhance the predictive capability, indicating that other factors also need to be considered. It could also be hypothesized that the key factors predicting lower extremity amputation in adults may have less influence in pediatric patients, as children tend to heal fractures faster, have better outcomes after nerve repair, exhibit lower rates of wound infection, and have greater cortical plasticity. 11
In addition to the MangLE score, other scoring systems have been employed to assess the need for amputation in pediatric patients with severe extremity injuries. One noteworthy example is the Mangled Extremity Severity Score (MESS). Although originally developed for adults, its use has also been evaluated in children. For instance, Behdad et al found in their research involving 200 children with mangled extremities that an MESS threshold of 6.5 could serve as a predictor for amputation in children, with a sensitivity of 73% and specificity of 54%. 21 Additionally, another study which evaluated the prognostic value of the MESS in pediatric patients with traumatic arterial injuries found that an MESS score below 7 was significantly associated with both initial (P < 0.05) and definitive limb salvage (P < 0.001) in lower extremity injuries. 7 However, it’s important to note that some experts caution against lowering the MESS threshold for children, emphasizing that decisions should be individualized and consider the unique physiological and healing capabilities of pediatric patients. 11 Furthermore, several other scoring systems, such as the Injury Severity Score (ISS), Pediatric Trauma Score (PTS), National Advisory Committee for Aeronautics (NACA) score, and Glasgow Coma Scale, are commonly used to assess traumatic injuries in pediatric patients, particularly those with polytrauma. 22 However, there is no previously published score which is designed solely to predict lower extremity amputation in children.
This study possesses several key strengths that enhance the validity and generalizability of its findings. One of its most notable advantages is the use of a large national data set, the TQIP database, which is contributed to by over 900 trauma centers across the United States. 23 The inclusion of data from such a vast and diverse range of institutions allows for a more representative sample, thereby improving the external validity of the results. Nevertheless, some limitations must be acknowledged. One primary limitation is the inherent constraints of the TQIP database and the retrospective nature of the study. The data set does not allow for direct comparisons with other established scoring systems, such as the MESS, PTS, NACA score, or GCS, which may have provided additional insights into patient outcomes. The study is additionally constrained by the inability to encompass all subtleties of lower extremity injuries, as the TQIP database lacks granular data pertaining to the results of neurovascular examination, the severity of crush injuries, the degree of soft tissue damage, discrepancies in care between hospitals, as well as outcomes such as long-term limb functionality, persistent pain, or other issues related to limb salvage. The database also lacks data on individuals who underwent lower extremity amputation at a later date following their initial period of hospitalization, resulting in a potential underestimation of long-term limb loss rates. Ultimately, these limitations underscore the necessity for future prospective investigations to validate the results of the current investigation and determine the true clinical utility of the MangLE score.
In conclusion, the MangLE score maintains an excellent predictive ability for identifying those unlikely to require lower extremity amputation in pediatric mangled extremity patients aged 10-17 years; however, it fails to accurately predict this outcome in the younger cohorts.
Supplemental Material
Supplemental Material - Prediction of Amputation Following Severe Pediatric Lower Extremity Injury: Application of the Mangled Lower Extremity (MangLE) Score in a Pediatric Population
Supplemental Material for Prediction of Amputation Following Severe Pediatric Lower Extremity Injury: Application of the Mangled Lower Extremity (MangLE) Score in a Pediatric Population by Maximilian Peter Forssten, Lovisa Ekestubbe, Bruno Coimbra, Yang Cao, Babak Sarani, and Shahin Mohseni in The American Surgeon™
Footnotes
Ethical Considerations
The relevant institutional review board waived the need for ethical approval.
Author Contributions
Conception and study design: MPF, YC, BS, and SM. Literature review: MPF, LE, and BC. Data acquisition: BS and SM. Data analysis and interpretation: MPF, YC, BS, and SM. Drafting of the manuscript: MPF and LE. Critical revision: All authors critically reviewed and accepted the manuscript submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.