
Abstract
Background
Despite rising rates of contralateral prophylactic mastectomy (CPM), little is known about how surgeons and patients communicate about the procedure. This study is among the first to use real-time audio recordings of CPM discussions, link conversations to treatment choice, and include multiple institutions. We assessed surgeon-patient discussions, focusing on how often CPM was addressed, who initiated it, and how decisions were made.
Methods
We recruited surgeons and patients from three academic centers and audio-recorded the first surgical consultation for patients with (1) early-stage unilateral breast cancer or ductal carcinoma in situ and (2) no strong family history or BRCA mutation. Transcripts were analyzed using an inductive, qualitative approach to generate themes and detect patterns.
Results
Twenty-seven patients and eight surgeons participated. In 14 cases, neither patient nor surgeon mentioned CPM. In the remaining 13, surgeons initiated the topic in 10, typically while introducing surgical options. Of the four patients who received CPM, each had a strong initial preference for CPM and was undeterred by the surgeon’s cautionary statements against it. When patients lacked strong preferences for CPM, they generally followed surgeon recommendations to forego CPM or to delay the decision until tests (eg, genetics and MRI) were complete.
Discussion
Surgeons, not patients, most commonly initiated CPM discussions. Initial patient preference strongly influenced surgical decisions. Surgeon recommendations to wait for additional information shaped decision making only when patients were initially undecided. Future research should explore how patients form preferences prior to consultation and how best to address them during clinical conversations.
Keywords
Key Takeaways
• Surgeons, not patients, most often initiated discussions about contralateral prophylactic mastectomy (CPM) during initial consultations. • Patients with strong preexisting preferences for CPM chose surgery despite surgeon recommendations to defer or avoid it. • Surgeon recommendations influenced decision making primarily when patients were initially undecided.
Introduction
Rates of contralateral prophylactic mastectomy (CPM) have risen markedly among women with early-stage breast cancer.1-6 Although clinical guidelines recommend CPM for patients at elevated risk—such as those with BRCA mutations or strong family histories—most individuals electing this procedure are at average risk.1,7-10 The processes underlying CPM decision making, particularly the communication between patients and providers, remain insufficiently characterized.
A key step in the decision-making process for early-stage breast cancer treatment is the surgical consultation. Many patients opt for CPM even after being informed that unilateral mastectomy or breast-conservation therapy provides equivalent survival.11-15 Fear of recurrence and anxiety are frequently cited motivators, with some surgeons reporting that they defer to patient preferences.16-19 Surgeon-patient interactions, including who initiates the topic, how information is framed (ie, clinical vs emotional domains), and whether the surgeon makes a recommendation, may significantly influence decision making.
Surgeons have stated that patients are the ones to initiate the topic of CPM and that surgeons generally refrain from recommending CPM or discourage it in the absence of a clinical indication.3,20-22 However, how these decisions unfold—and how communication shapes treatment choice—remains poorly understood. Prior research has relied on retrospective recall by patients and surgeons, observed consultations only in a single institution, or not linked conversations to treatment choices.18,22,23 This study examined how CPM is discussed, focusing on who initiates it, how it is framed, and how the conversation influences decision making surrounding CPM.24,25
Methods
Design Overview
This study was approved by the Institutional Review Board at the lead institution (Protocol #14-1476), with reliance agreements at participating sites. This was an observational, multi-site cohort study, using content analysis of audio recordings of the initial encounter between patients with early-stage breast cancer and surgeons.
Eligibility and Enrollment
The study was conducted at three academic medical centers in the United States. Eligible participants were adult women with stages I-III unilateral breast cancer or ductal carcinoma in situ (DCIS), with no known BRCA mutation and no strong family history of breast cancer. 26 Patients were enrolled at their first surgical oncology visit, before seeing the surgeon, over a two-month period in 2016.
Participants and accompanying family/friends gave consent for audio recording. We sought a sample of 15 patients per site, an acceptable number for qualitative analysis. 27 Surgeons gave consent for audio recording once before patient enrollment began.
Data Collection
Recording started before or when the surgeon entered the room and stopped when the surgeon left. Recordings were transcribed verbatim and de-identified.
Content Analysis of Recordings
Seven research team members trained in qualitative analysis of physician-patient communication participated. Using selective coding, five team members (VC, AK, VD, CL, and KD) used an inductive method to classify observations, concepts, and themes and brought these to the group for further discussion. We used NVivo software (11.4.0) for analysis. 24
Utilizing codes to classify themes, we compared new and prior codes to form categories. These were then used to develop and refine a codebook, which we applied systematically across the sample to identify surgeon and patient thought patterns and communication behaviors. After coding all transcripts, the team reviewed trends iteratively and generated a final list of themes and quotes. This method yielded themes of interest with thematic saturation.
Results
Participants
Eight out of nine surgeons agreed to have their visits recorded. We approached 45 eligible patients. Thirty consented to audio recording (see Figure 1). Two participants’ recordings were not transcribed because of ineligibility due to a BRCA mutation or strong family history of breast cancer. One participant’s recording was transcribed but excluded due to history of mantle radiation, a guideline-supported indication for CPM.
26
Patient Flow Diagram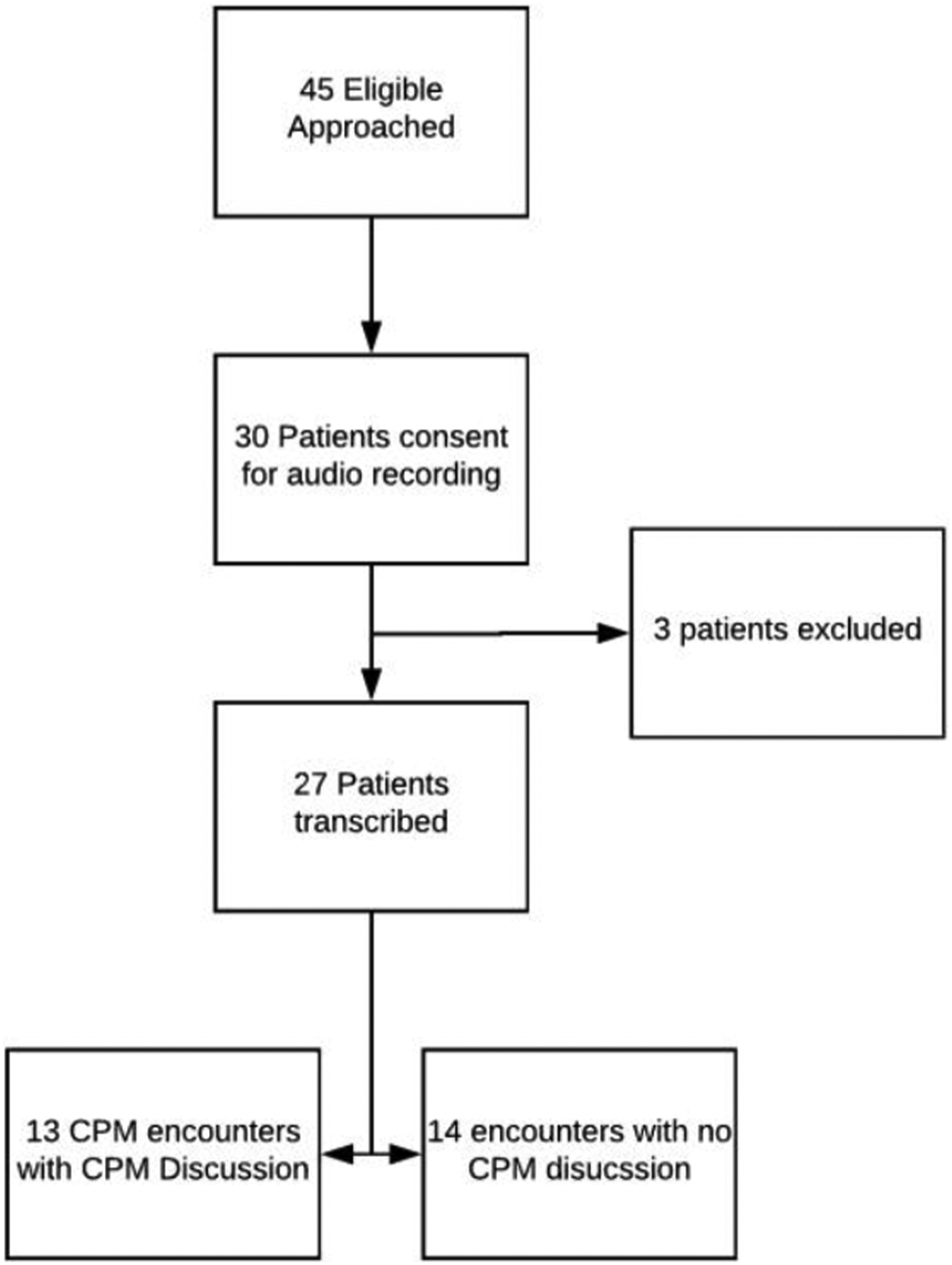
Overview of Discussions About CPM
In 14 of the 27 consultations, neither the surgeon nor patient mentioned contralateral breast surgery. In the remaining thirteen consultations, four elements were important to the decision about CPM—who initiated the discussion, whether the surgeon recommended waiting for more information, discussion of anxiety, and patient preference for CPM. Treatment choices fell into three categories—(1) decision to have CPM (n = 4), (2) decision to discuss CPM again when more data such as genetic testing and imaging were available (n = 7), and (3) decision to forego CPM (n = 2).
Who Initiates the CPM Discussion?
Surgeons initiated the topic of CPM in 10 of 13 conversations, and patients initiated it in three. In six cases, the surgeon introduced CPM as one of the primary treatment options for early-stage breast cancer.
In two cases, surgeons brought up the topic of CPM while discussing BRCA testing. In one case, the surgeon mentioned CPM when explaining the role of plastic surgery consults. And in another, the surgeon initiated CPM by discussing that some women chose to have CPM due to the anxiety associated with cancer.
Patients initiated the topic of CPM in three conversations. One patient brought up CPM, asking for a clarification about whether the surgeon’s description of mastectomy was referring to unilateral or bilateral:
Another patient initiated the topic by asking the surgeon for recommendations concerning unilateral mastectomy vs CPM:
One patient began a CPM discussion by sharing an anecdote of a friend who had a bilateral mastectomy:
Framing of the CPM Decision—Personal vs Clinical
Patients typically framed decisions about CPM in terms of personal or emotional outcomes.
Surgeons typically framed decisions around clinical outcomes, such as survival and risk (see cases 2 and 5 above for examples). Sometimes they noted the emotional aspects of CPM, referring to how “some people” make decisions.
Impact of Surgeon Recommendations Regarding CPM
Surgeons made a recommendation about CPM in eight of the thirteen CPM discussions. In these cases, surgeons framed the procedure as beneficial for patients with a BRCA mutation and recommended against it otherwise.
All but one patient followed the surgeon’s recommendation to delay the decision about CPM until after BRCA testing. In one conversation, the patient stated she knew she wanted CPM. Although the surgeon recommended against it, the patient chose CPM because (described in the next section).
Patients with a Strong Preference for CPM
Four of the thirteen patients expressed a strong preference for CPM, and all four patients decided to have CPM. Although each interaction was unique, there were commonalities among them. In every case, surgeons explained multiple disadvantages of CPM, including no survival benefit, minimal decrease in contralateral breast cancer incidence, and altered feeling in the breast. In all four cases, however, patients restated their preference for CPM, providing additional reasons, such as being unconcerned about post-surgical appearance and having sought recommendations from others. The surgeons did not explicitly recommend CPM in any of these cases. In one case, the surgeon recommended against CPM. Yet all four patients decided to have CPM.
The patients provided additional reasons for desiring CPM. In three cases, patients referred to friends’ or family members’ experiences with breast cancer as reasons.
Finally, after each of the four patients chose CPM, the surgeon affirmed the patient’s decision:
Discussion
This study offers novel insights into how CPM was discussed during initial surgical consultations at three institutions. Our qualitative analysis of audio-recorded conversations extends previous work based largely on retrospective patient or surgeon report without direct linkage to treatment choices.18,22,23
Among 27 recorded consultations, CPM was discussed in 13. In contrast to prior studies suggesting patients typically initiate these conversations, we found that surgeons introduced the topic in most cases (10 of 13), often presenting it as a treatment option.11,18,23,28,29 While this may reflect surgeons expecting patients’ interests, the absence of CPM discussions in nearly half of the consultations suggests a more selective strategy. A more plausible interpretation is that surgeons selectively introduced CPM based on patient-specific cues such as anxiety, tumor characteristics, or clinical context. 29 Surgeon-level factors, including personal attitudes and institutional culture, likely contributed to variation.29,30
When CPM was addressed, surgeons typically advised against the procedure or recommended deferring the decision pending additional diagnostic information (eg, BRCA testing), basing their recommendations on objective clinical risk. In contrast, patient preferences were more often shaped by emotional factors, including fear of recurrence and desire for peace of mind. This divergence is supported by prior work.31-34 For example, Benedict et al linked cancer-specific worry to increased uptake of more aggressive surgery, while Yao et al found that surgeons discouraged CPM in average-risk patients when guided by evidence-based risk assessment (eg, BRCA status and projected clinical benefits).31,34 These findings underscore the importance of shared decision-making models that integrate both clinical data and patients’ emotional concerns.
Four patients in our cohort expressed strong preferences for CPM, and all proceeded with surgery, despite surgeons outlining the limited survival benefit and potential risks. One patient stated, “my mind was made up,” reflecting a decision formed prior to consultation. This observation is consistent with the literature showing that increased patient involvement is associated with higher rates of mastectomy.35-38 It also aligns with D’Agostino et al, who found that patients with firmly held views entering consultations were not swayed by clinical recommendations. 22 This limited influence of surgeon recommendation likely reflects the aforementioned divergence in framing—patients prioritizing emotional reassurance, and surgeons emphasizing oncologic risk and survival.
Conversely, surgeons’ recommendations had greater influence on patients who were undecided about CPM. Most of these patients followed their surgeon’s guidance, particularly when advised to delay the decision or consider less extensive surgery. Similar patterns were noted by Padamsee et al, who found that patients without strong preexisting preferences were more receptive to clinical recommendations. 23 This is consistent with findings from prostate cancer consultations, where surgeon recommendations had the greatest influence on treatment and often superseded patients’ initial preferences. 39 These results suggest that decision-support interventions may be most effective if implemented earlier—ideally at the time of diagnosis—before preferences are firmly established.
This study has some limitations. The participants were English-speaking and received care at academic medical centers, which may limit generalizability. Only the initial consultation was analyzed, so we may not have captured evolving preferences or decisions shaped by subsequent clinical interactions. The data were collected in 2016, and evolving clinical practices or patient perspectives since then may not be fully reflected. Finally, our patient sample size was relatively small, limiting the ability to generalize findings or assess the frequency of CPM discussions across broader clinical populations.
The study has several strengths. Its prospective, multi-institutional design and the use of direct audio recordings provide rare and valuable insights into surgeon-patient communication about CPM. Few studies have captured primary data on how CPM is discussed during clinical encounters. This qualitative approach enabled the identification of unexpected patterns, such as surgeon-initiated CPM discussions and the decisive influence of patient initial preference on surgery choice.
Conclusions
Surgeons more frequently initiated CPM discussions than patients, though typically not to advocate for the procedure. Patients with strong preexisting preferences for CPM proceeded with surgery despite surgeon concerns. In contrast, patients without firm preferences were more likely to follow clinical recommendations to defer or avoid CPM. These findings highlight the complex interplay between medical guidance and patient values. They underscore the importance of communication strategies that balance evidence-based recommendations with emotional and psychological considerations.
Footnotes
Author Note
This study was presented at the Annual Meeting of the Society for Medical Decision Making (SMDM) October 26th, 2017, in Pittsburgh, Pennsylvania.
Acknowledgments
The authors thank Vanessa Dickerman and Michael Sabel for their contributions to this study and manuscript.
Ethical Approval
This study was approved by the Institutional Review Board at the study site (reference number 14-1476).
Consent to Participate
All participants and surgeons provided written informed consent for audio recording and participation prior to enrollment.
Author Contributions
Grace Anne Longfellow, BS: Writing—original draft; writing—review and editing.
Vinay Choksi, BS: Formal analysis; writing—review and editing; data curation.
Peter A. Ubel, MD: Writing—review and editing; supervision; resources.
Allison Kratka, BA: Formal analysis; writing—review and editing.
Mara Buchbinder, PhD: Methodology; writing—review and editing.
Christine Kirby, MA: Writing—original draft; formal analysis.
Kelly Davis, BA: Data curation; project administration.
Sarah Hawley, MD: Conceptualization; writing—review and editing.
Karen Sepucha, MD: Conceptualization; writing—review and editing.
Michelle Specht, MD: Conceptualization; writing—review and editing.
Clara Lee, MD: Conceptualization; methodology; resources; writing—original draft; writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a UNC Lineberger Comprehensive Cancer Center Population Sciences Award and NIH/NCI K07CA154850-01A1 and Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill (Population Sciences Award).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Sepucha received salary support from the Informed Medical Decisions Foundation, which was part of Healthwise, a not-for-profit foundation that develops and distributes patient education and decision support materials.
Data Availability Statement
Data are available from the corresponding author on reasonable request.