
Abstract
Background
Robotic-assisted Heller myotomy (RAHM) is increasingly utilized for the surgical treatment of achalasia. While prior studies have suggested potential technical advantages of RAHM over laparoscopic Heller myotomy (LHM), the economic implications remain less well-defined. This study aimed to compare hospitalization costs and clinical outcomes between RAHM and LHM using a nationally representative cohort.
Methods
The 2016-2021 Nationwide Readmission Database was utilized to identify adult patients ((≥18 years) undergoing either LHM or RAHM for achalasia. Entropy balancing on key variables followed by multivariable linear regression analysis was used to elucidate the association between LHM and RHM on outcomes, including mortality, 30-day readmission, hospitalization costs, and length of stay (LOS).
Results
Among 14 662 patients, 30.5% underwent RAHM. While use of RAHM increased over the study period, LHM remained the most frequently performed approach. There were no significant differences in mortality (0.25% vs 0.19%, P = 0.64), LOS (3.1 vs 3.0 days, P = 0.09), or 30-day readmissions (4.86% vs 4.88%, P = 0.98) between RAHM and LHM. However, index hospitalization costs were higher for RAHM ($19,387 vs $16,317, P < 0.001), and this cost difference persisted after adjustment (β +$3,345, 95% CI $2473–$4,217, P < 0.001).
Conclusion
Robotic-assisted Heller myotomy and LHM demonstrate equivalent short-term clinical outcomes for achalasia. However, RAHM is consistently associated with higher hospitalization costs, warranting further evaluation of its economic impact.
Key Takeaways
• Laparoscopic Heller myotomy remains the most common method of Heller myotomy. • Robotic-assisted Heller myotomy is associated with equivalent mortality and 30-day readmissions compared to LHM. • Robotic-assisted Heller myotomy is associated with increased overall cost by $3345.
Introduction
Minimally invasive surgical techniques, including laparoscopic Heller myotomy (LHM) and robotic-assisted Heller myotomy (RAHM), are central to the management of primary idiopathic achalasia, a rare esophageal motility disorder characterized by impaired relaxation of the lower esophageal sphincter and absent peristalsis. 1 Since the first reported case of RAHM in 2001, the use of robotic platforms in foregut surgery has grown steadily. 1 Previous meta-analyses have highlighted RAHM’s potential advantages, including reduced esophageal perforations, decreased length of stay, and reduced complication rates compared to laparoscopic Heller myotomy (LHM).2,3 However, these benefits have often come at the expense of prolonged operative times and increased costs.4–7
Despite the increasing adoption of RAHM, its comparative value relative to LHM remains uncertain, particularly when considering short-term outcomes and economic impact. Prior studies have been limited by small sample sizes, heterogeneous reporting of outcomes, and institutional bias. Additionally, the cost-effectiveness of robotic surgery in the setting of achalasia has not been well characterized using large-scale national data.
To address these knowledge gaps, we used the Nationwide Readmissions Database (NRD), a large, all-payer resource encompassing 59% of all U.S. hospitalizations, to compare clinical and economic outcomes of RAHM vs LHM from 2016 to 2021. 8 The NRD links inpatient hospitalizations annually, allowing for the capture and tracking of readmissions. It also enables the analysis of relatively rare procedures like Heller myotomy at a national scale, across diverse hospital settings, and allows for robust adjustment of confounding factors. Importantly, the NRD captures total hospitalization costs using standardized cost-to-charge ratios and tracks 30-day readmissions, making it well-suited for cost and outcome comparisons. Using this powerful resource, we aimed to evaluate trends in utilization and determine differences in mortality, 30-day readmission, length of stay, and index hospitalization costs.
Methods
This was a retrospective cohort study utilizing the Nationwide Readmissions Database (NRD). This study was exempt from full review by the Institutional Review Board at the University of California, Los Angeles (IRB #17-001112).
All elective adult (≥18 years) procedures for Heller myotomy were tabulated from the 2016 to 2021 Nationwide Readmissions Database (NRD) using International Classification of Diseases, 10th Revision codes (ICD-10) (OD844ZZ, OD843ZZ, 8E0W0CZ, 8E0W3CZ, 8E0W4CZ, 8E0W7CZ, 8E0W8CZ, and 8E0WXCZ). Patients with a history of achalasia (K220) were identified. Patients with a history of gastric band (K95.09), esophageal, or gastric cancer (C15, C16, D13.0, D13.1, and C49.A1) or missing data (age, sex, hospital LOS, discharge disposition, and costs) were excluded to enhance cohort homogeneity (exclusion data 8.4%).
Patient and hospital characteristics including age, gender, primary insurer, income quartile, hospital size, and teaching status were tabulated using the Healthcare Cost and Utilization Project data dictionary. 9 The Elixhauser Comorbidity Index was used to quantify the burden of chronic conditions. Costs were calculated by using hospital-specific cost-to-charge ratios to overall hospitalization costs and adjusted for inflation using the 2021 Medical Expenditure Survey Personal Healthcare Price Index. 10
The primary outcomes of interest were in-hospital mortality, length of stay, and costs during the index hospitalization. Secondary outcomes included major adverse events (neurologic, thromboembolic, cardiac, respiratory, infectious, and renal complications) and non-elective 30-day readmissions.
Continuous variables are reported as means and standard deviations (SDs) if normally distributed or as medians and interquartile ranges (IQRs) if non-normally distributed. Categorical variables are presented as proportions (%). Patient and hospital characteristics were compared using the Mann-Whitney U, adjusted Wald, or Pearson’s chi-square tests. Temporal trends were assessed using Cuzick’s 11 nonparametric test (nptrend). To adjust for differences in characteristics between cohorts, we applied entropy balancing which uses pseudo propensity scores to balance the distribution of covariates, as previously described. 12 Model covariates were selected using the Least Absolute Shrinkage and Selection Operator (LASSO) method which reduces collinearity and model overfitting using a penalized methodology. 13 Additional subgroup analyses were conducted to examine risk-adjusted rates of primary and secondary outcomes. Laparoscopic Heller myotomy and RAHM procedures were assessed by quartiles of annual procedural volume. The highest and lowest volume quartiles were compared. Model outputs are reported as adjusted odds ratios (AORs) or as beta (β) coefficients with 95% confidence intervals (CIs). All statistical analyses were conducted using Stata version 16.0 (StataCorp LLC, College Station, TX); statistical significance was set at a P-value <0.05.
Results
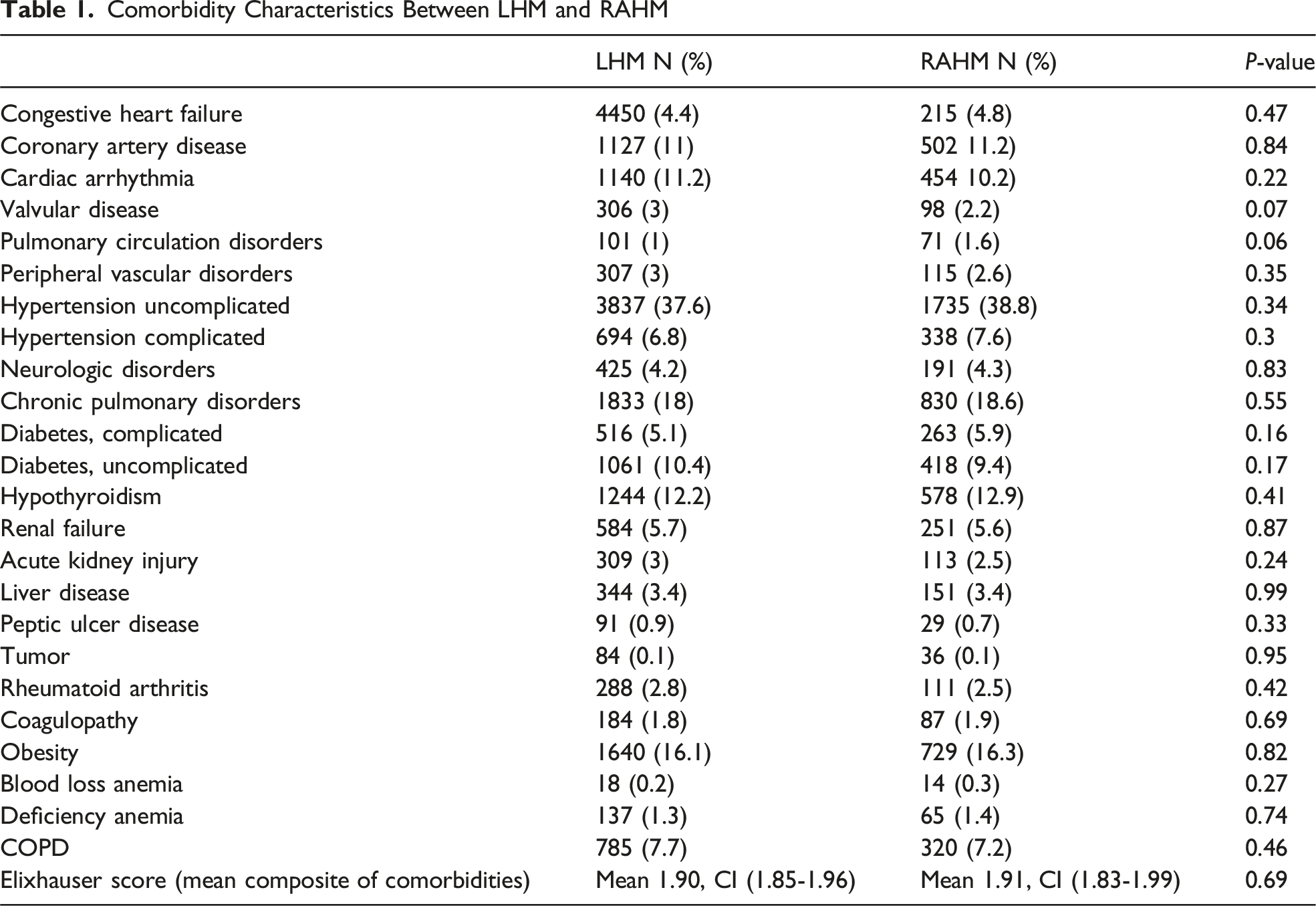
An estimated 14 662 patients were identified during the study period, of whom 30.5% underwent RAHM. The utilization of LHM significantly decreased from 2095 cases in 2016 to 1248 cases in 2021 (nptrend <0.001). Conversely, RAHM utilization demonstrated a significant increase from 640 cases in 2016 to 792 cases in 2021 (nptrend <0.001) (Figure 1). Baseline characteristics were largely comparable between the RAHM and LHM cohorts. Compared to LHM, patients who underwent RAHM were similar in age (56.7 years vs 57.0 years, P = 0.83), proportion of male patients (51.7% vs 49.7%, P = 0.41), and Elixhauser Comorbidity Index score (1.91 vs 1.90, P = 0.52). Comorbidities were similar between the 2 groups (Table 1). Case Volume of Laparoscopic vs Robotic Heller Myotomy From 2016 to 2021 From the NRD Comorbidity Characteristics Between LHM and RAHM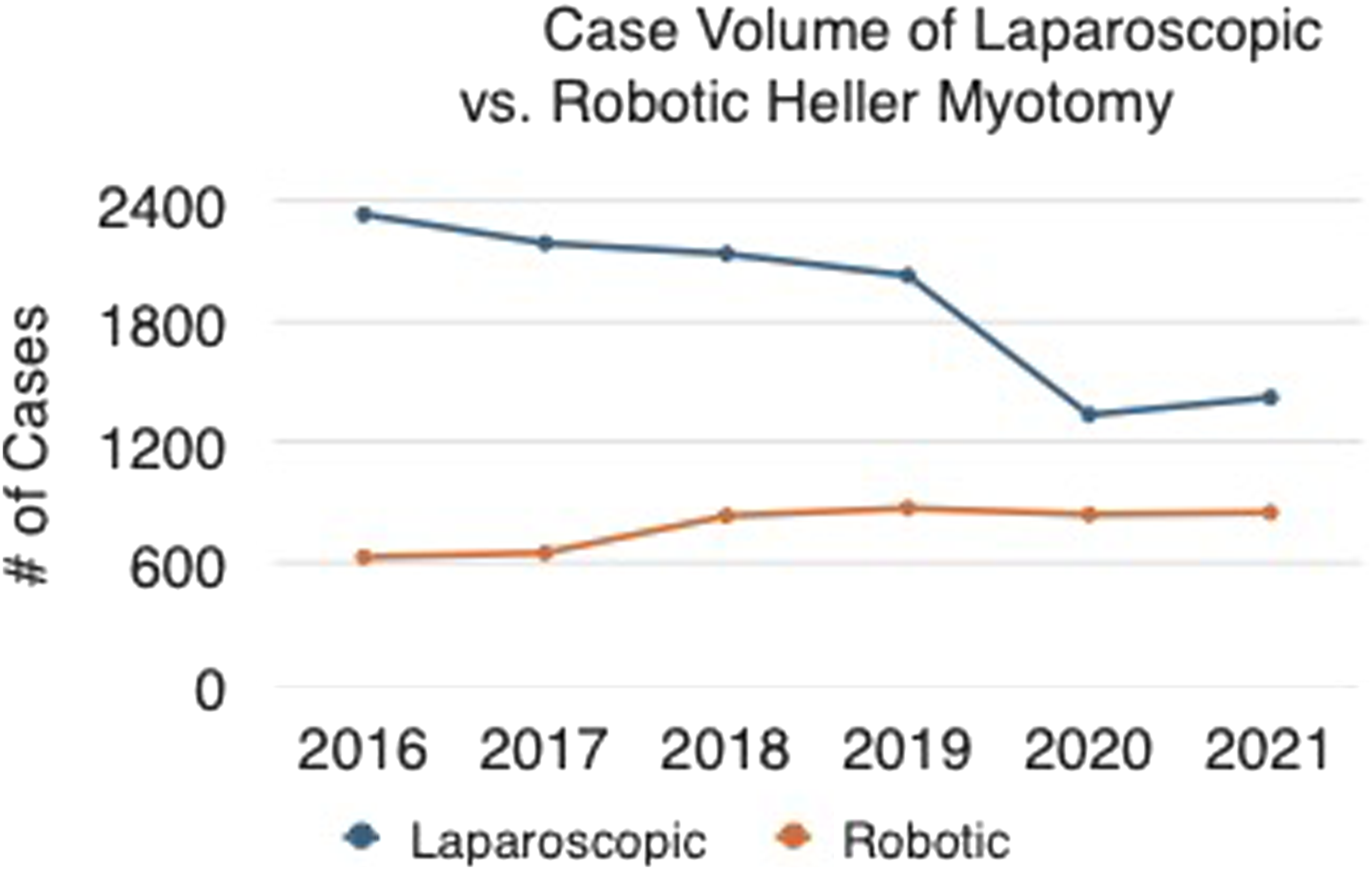
Compared to LHM, RAHM was associated with similar rates of mortality (0.25% vs 0.19%, P = 0.64), major adverse events (8.6% vs 8.2%, P = 0.60), and non-elective 30-day readmissions (4.86% vs 4.88%, P = 0.98). In addition, patients had similar LOS (RAHM 3.1 vs 3.0 days, P = 0.09), but mean index hospitalization costs were significantly higher in the RAHM group compared to LHM ($19,387 vs $16,317, P < 0.001). After adjustment for baseline differences using entropy balancing and multivariable regression, RAHM remained independently associated with increased costs (β +$3,345, 95% CI $2473–$4,217, P < 0.001), indicating that the higher cost persisted even after accounting for potential confounders. This cost differential was persistent across every age demographic (Figure 2). After entropy balancing and multivariable adjustment, there were no significant differences in adjusted odds of mortality (AOR 1.20, P = 0.77), major adverse events (AOR 1.09, P = 0.36), or 30-day readmissions (AOR 1.03, P = 0.83) between RAHM and LHM. Additionally, there was no statistically significant difference in length of stay (LOS) (β + 0.26 days, 95% CI −0.35: +0.88 days, P = 0.40). Cost Differential Between Laparoscopic vs Robotic Heller Myotomy Across Ages 40-80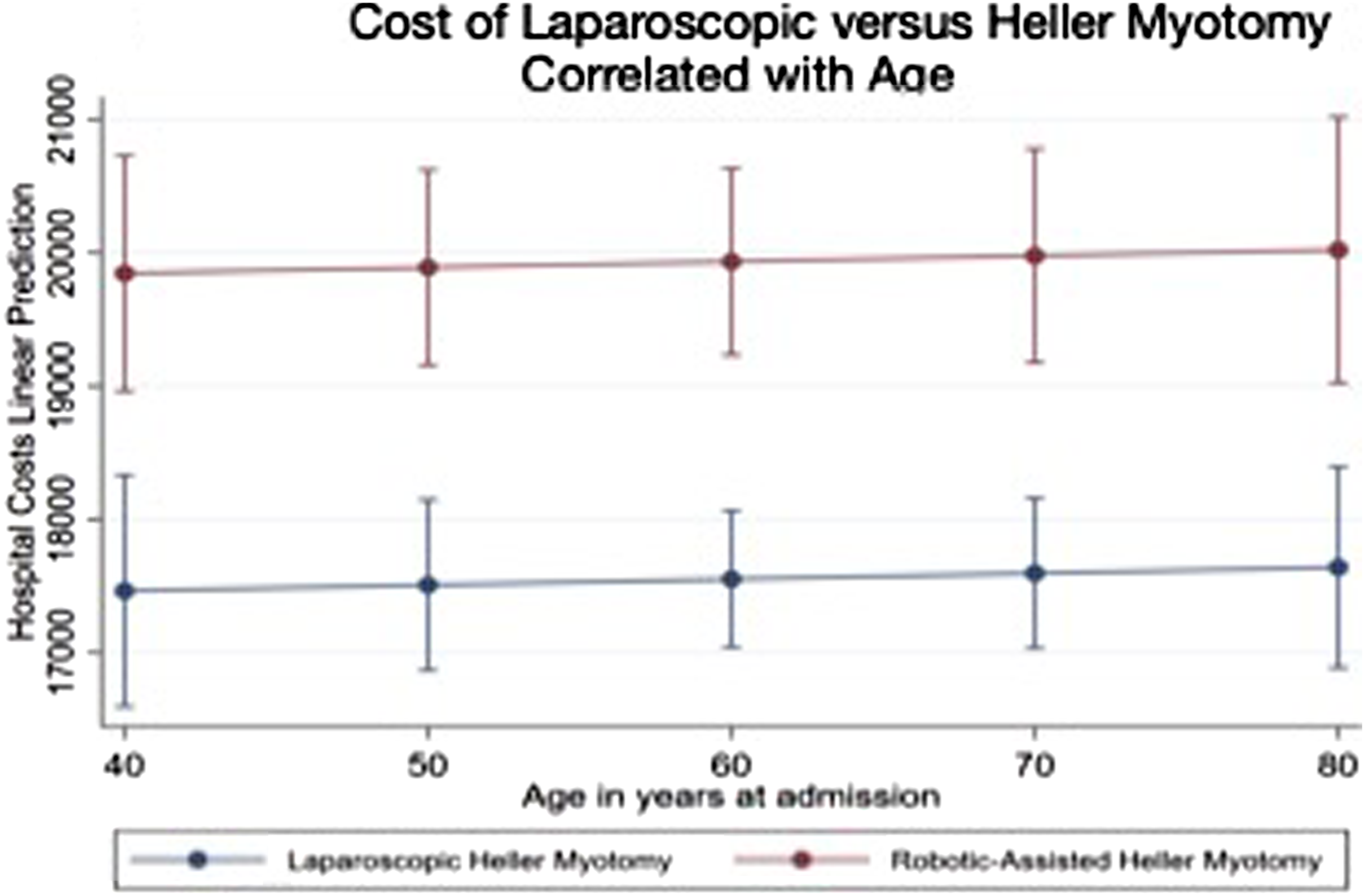
To further evaluate the impact of LHM or RAHM volume on primary outcomes, a subgroup analysis was conducted. After adjusting for LHM volume, there was no difference in mortality (AOR 0.80, 95% CI: 0.08-7.18), length of stay (β −0.20 days, 95% CI: −0.58: 0.19), hospitalization costs (β −$2.25 K, 95% CI: −$3.65 : −$0.86 K), major adverse events (AOR 0.70, 95% CI: 0.49-1.00), or 30-day readmissions (AOR 1.30, 95% CI: 0.76-2.23). After adjusting for RAHM volume, there was no difference in mortality (AOR 1.01, 95% CI: 0.26-3.98), length of stay (β −0.73 days, 95% CI: −1.83: 0.38), major adverse events (AOR 0.67, 95% CI: 0.43-1.03), or 30-day readmissions (AOR 0.81, 95% CI: 0.37-1.77). There was a significant difference in hospitalization costs (β −$2.96 K, 95% CI: −$5.68: −0.25 K).
Discussion
In this updated database analysis, RAHM demonstrates comparable efficacy to LHM in terms of acute mortality, 30-day readmission rates, major adverse events, and length of stay. Despite these equivalent clinical outcomes, RAHM was consistently associated with higher hospitalization costs compared to LHM. These findings merit further evaluation and discussion of the clinical and economic value of RAHM in the treatment of achalasia.
Both LHM and RAHM effectively mitigate the debilitating effects of achalasia, demonstrating superior perioperative outcomes compared to open Heller myotomy, including reduced length of stay, lower overall morbidity, and decreased 30-day readmission rates. 14 Additionally, the inclusion of a fundoplication in both techniques helps reduce reflux-related morbidity compared to peroral endoscopic myotomy (POEM). 15 Multiple studies have confirmed the safety and efficacy of RAHM relative to LHM, and our findings further support this paradigm.4–6,16,17 Mortality rates in our study were consistent with those reported in the existing literature, showing no significant difference between the 2 approaches. 17 Similarly, other perioperative outcomes, including 30-day readmission rates, major adverse events, and length of stay (LOS), were equivalent in both the total analysis and volume subgroup analyses. Although Ataya et al 2 reported a reduced LOS in the robotic cohort, their findings were likely influenced by a higher incidence of esophageal perforation and an observed trend toward increased mortality in the LHM cohort. In contrast, our data align with several other studies that found no significant differences in LOS between RAHM and LHM.17,18
Given the similar clinical outcomes between RAHM and LHM, economic considerations become critical. Chacko et al, 7 spanning 2010 to 2015, showed a significant $8600 difference in overall hospital costs ($42,900 for RAHM vs $34,300 for LHM), despite a higher length of stay in the laparoscopic cohort. Similarly in Delgado et al’s analysis of pediatric Heller myotomy, the cost of surgery was higher in the RAHM group ($9670 vs $6130), although total hospitalization costs were seen to be significantly less ($60,360 vs $28,660) due to the higher cost of complications/readmissions in the LHM group. 19 In Shaligram et al’s analysis, the LHM cohort also consistently cost less ($7441 ± 7897 vs $9415 ± 5515). 17 In our study, the overall hospitalization costs for RAHM remained significantly higher ($19,387 vs $16,317) than those for LHM, a finding that aligns with the previously mentioned studies.7,17,19 This discrepancy in cost was not found to be associated with age-related postoperative comorbidities as seen in Figure 2 but consistently remained statically disparate across all age ranges. Additionally, the cost differential between RAHM and LHM remained apparent in the subgroup analyses looking at the hospitals in the top and lowest quartiles by volume, possibly indicating that increased experience and potentially shorter operative times did not make a significant impact on the cost gap.
The persistent cost disparity between RAHM and LHM appears to be multifactorial, driven by both equipment-related expenses and longer operative times, neither of which have been conclusively offset by increased experience or institutional volume. The increased costs associated with RAHM may be attributable to the use of disposable robotic instruments (approximately $1866 per procedure) and the lack of competition within the robotic surgery market. 20 The emergence of alternative robotic systems or the development of longer-lasting and reusable equipment could help mitigate this cost disparity. Additionally, the higher overall cost may be partially driven by differences in operative duration, which influence hospital resource utilization and staffing requirements. Numerous studies have reported longer operative times for RAHM compared to LHM. For example, Ataya et al 2 meta-analysis identified an average 23-min increase in operative duration for RAHM. Factors such as surgeon proficiency, robotic docking, reliance on bedside assistants, institutional volume, and resident involvement also contribute to these differences. High-volume centers, as demonstrated by Raja et al, have shown a reduction in operative times for RAHM over the course of their study, with a 21-min shorter operative time compared to their LHM cohort. 16 However, this improvement has yet to be shown in any multi-institutional studies. In 2018, Childers et al showed that each minute of OR time cost $36 with up to $20 of this in direct cost. 21 Until such a time as the average RAHM operative time matches LHM, and robotic instruments are reusable, the cost differential will remain.
Despite higher costs and equivalent short-term outcomes compared to LHM, the adoption of RAHM has continued to rise, prompting ongoing debate about its clinical value and cost-effectiveness (Figure 1). The National Readmissions Database (NRD), encompassing a wide range of both academic and non-academic institutions across the United States, offers a representative assessment of current trends in laparoscopic and robotic foregut surgery. In our study, LHM still remained the most common platform for completing a Heller myotomy throughout the course of the study period (Figure 1). However, there was a significant drop in total number of cases in 2020 and 2021, possibly secondary to the COVID-19 pandemic. With the increase in popularity of RAHM, advocates of robotic surgery cite the improved dexterity and technical facilitation of suturing as potential advantages over LHM. 2 However, with equivalent morbidity, mortality, and LOS and increased cost compared to LHM, the clinical relevance of this is unclear. Over the last 5 years, multiple studies have sought to elucidate the clinical advantages of RAHM. Two recent large meta-analyses showed decreased rates of esophageal perforation within the RAHM cohort but neither showed worsened morbidity for the LHM cohort.2,3 Conversely, Raja et al showed equivalent short-term palliation (Eckardt score <3) in both cohorts but significantly improved long-term functional outcomes at 4 years in their RAHM cohort where only 1.7% of patients had Eckardt scores >3 compared to 10% within the LHM cohort. 16 While early data suggest possible long-term functional advantages of RAHM, these findings remain preliminary and require validation through multi-center studies before justifying its broader adoption based on clinical superiority or cost-effectiveness.
The limitations of this study are consistent with those inherent to large database analyses. The NRD lacks data granularity, such as the inability to track intraoperative data or specific complications, including esophageal perforation, or to evaluate long-term outcomes such as postoperative esophageal emptying or Eckardt scores. Another notable limitation is the inability of the NRD to distinguish between primary and re-operative cases, which could significantly influence the overall cost and mortality rates observed in the RAHM cohort. Furthermore, the study evaluated total hospital costs rather than isolating operative costs or personnel expenses, which may provide more precise insights into the financial implications of RAHM. Operative time, a key factor contributing to increased costs, was not assessed. Given that multiple studies have reported prolonged operative durations for RAHM, incorporating this metric in future research could help clarify the cost differential.
This study represents the largest contemporary series comparing LHM and RAHM. It underscores the accelerating adoption of RAHM as a preferred modality, reflecting a broader trend toward robotic surgical platforms in the management of achalasia. Further research into cost-reduction strategies, such as technological advancements and improvements in efficiency within surgical teams, will be essential to optimizing the value of the robotic-assisted approach.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P. Benharash received fees from AtriCure as a surgical proctor. This manuscript does not discuss any AtriCure products or services. Other authors report no conflicts.