
Abstract
Background
Older adult (OA) abuse affects the health and welfare of people ages 65 and older. Although previous research has shown that OA abuse impacts their well-being, there is limited understanding of the injury profiles and outcomes for OAs with or without reported abuse. This study compared OAs who reported abuse ((+)RA) to those who did not ((−)RA), hypothesizing OAs with (+)RA have increased mortality.
Methods
The 2017-2019 Trauma Quality Improvement Program (TQIP) was queried for all OAs ages 65 and older. The primary outcome was mortality. Bivariate analyses were performed to compare OAs with (+)RA and (−)RA. Separate multivariable analyses were performed to determine if (+)RA was associated with risk of complications or mortality.
Results
Out of 937 465 OAs, 1552 (0.2%) had (+)RA. OAs with (+)RA had increased rates of gunshot wounds (5.7% vs 0.7%, P < .001) and stab wounds (1.9% vs 0.4%, P < .001) compared to (−)RA patients. (+)RA patients also had increased mortality (6.7% vs 4.2%, P < .001), hospital LOS (5 vs 5, P < .001), and more often underwent surgical interventions (19.0% vs 14.3%, P < .001). On multivariable analysis, OAs with (+)RA had an increased associated risk of complications (OR 1.41, CI 1.16-1.71, P < .001) and mortality (OR 1.35, CI 1.06-1.70, P = .012) compared to OAs with (−)RA.
Discussion
This national analysis demonstrated that OAs with (+)RA had increased rates of penetrating trauma, surgical interventions, ventilator days, and death compared to (−)RA patients. Future prospective studies are needed to ascertain if primary prevention efforts can mitigate the increased morbidity and mortality seen in this vulnerable population.
Keywords
Key Takeaways
• Older adult abuse is a major public health concern and was reported in over 1500 patients in this study. • Interestingly, these patients had an increased rate of penetrating trauma, as well as longer hospital stays and increased mortality.
Introduction
Older adult abuse is a major public health concern, with prior estimates of more than 5.5 million annual unreported cases in the United States alone. 1 Some estimate only 1 out of 14 incidents of elder abuse are reported to relevant authorities.1,2 Older adults may suffer from different types of neglect and abuse, including physical, emotional, or financial. 3 Variables such as education level and functional impairment may play a role in the severity and type of abuse endured by older adults. 1 It is important to note that an older adult who experiences abuse has a three-fold greater likelihood of being hospitalized compared to one not suffering abuse. 4 In addition, elder abuse leads to high utilization of health care services such as Emergency Room visits and potentially prolongs hospital stays due to increased complexity of social issues and unique injury patterns. 5 This not only worsens the health conditions of the victims but also places a significant burden on the overall health care system. 3
Previous studies have mostly looked at heterogeneous older adult medical populations without considering if they had RA or not, resulting in a lack of detailed understanding of how reporting status correlates with clinical outcomes, especially for trauma patients.3,5 Although the increased awareness of reporting status has led to a recent similar study, 6 there is still a paucity of research available to explore disparities in the health outcomes between older adult trauma patients who had RA and those who did not. 6 Therefore, this study aimed to focus on the injury profiles and outcomes of OAs with and without reported elder abuse to further investigate their impact on this vulnerable population and help generate sub-populations who may most benefit from primary prevention. We hypothesize that OAs who reported abuse ((+)RA) have increased rates of mortality and hospital length of stay (LOS) compared to OAs without reported abuse ((−)RA).
Methods
This study was deemed exempt by our Institutional Review Board, and written informed consent was waived as this study used a national deidentified database. The 2017-2019 Trauma Quality Improvement Program (TQIP) was queried for older adult trauma patients 65 years of age and older with (+)RA and (−)RA upon admission. Patients with missing information regarding abuse reports were excluded from our analysis.
OA trauma patients with (+)RA were compared to OA (−)RA patients. The primary outcome was mortality. Secondary outcomes included hospital LOS, intensive care unit (ICU) LOS, ventilator days, and surgical interventions. Demographic variables collected included age, sex, race, ethnicity, and comorbidities including cerebrovascular accident (CVA), congestive heart failure (CHF), diabetes, alcohol use disorder, smoking, vital signs on arrival, and alcohol screening. A modified frailty index (mFI-5) score was calculated based on the comorbidity data available in TQIP, with a categorical variable created to classify patients as having 1, 2, or 3 or more deficits. Injury profile data collected included: mechanisms of injury (eg, falls, motor vehicle collisions (MVCs), pedestrians struck, gunshot wounds, and stab wounds), injury severity score (ISS), and specific injuries to the brain, stomach, colon, rectum, spinal cord, and lower extremity and pelvic fractures. Additional complications and outcomes collected included ventilator-associated pneumonia (VAP) and withdrawal of care.
Bivariate analyses were performed utilizing the Mann-Whitney U test to compare continuous variables and Pearson’s chi-squared analysis to compare categorical variables. Continuous variables were reported as medians with an interquartile range, and categorical variables as frequencies. Multivariable logistic regression models were also used to evaluate the associated risk of complications and mortality between OAs with (+)RA and OAs without after controlling for known predictors of mortality and complications including age ≥ 65, ISS, hypotension on arrival (systolic blood pressure <90mmHg), tachycardia on arrival (heart rate >90 beats per minute), and tachypnea on arrival (respiratory rate >22 breaths per minute). These variables were selected based on author consensus and review of existing literature.3,6 All analyses were two-sided and were performed using IBM SPSS Statistics for Windows (version 29; IBM Corp., Armonk, NY) with a statistical significance set at P < 0.05.
Results
Demographics and Comorbidities for the (+)RA Group vs the (−)RA Group
Demographics, Comorbidities, and Vitals for Older Adult Patients With and Without Reported Abuse
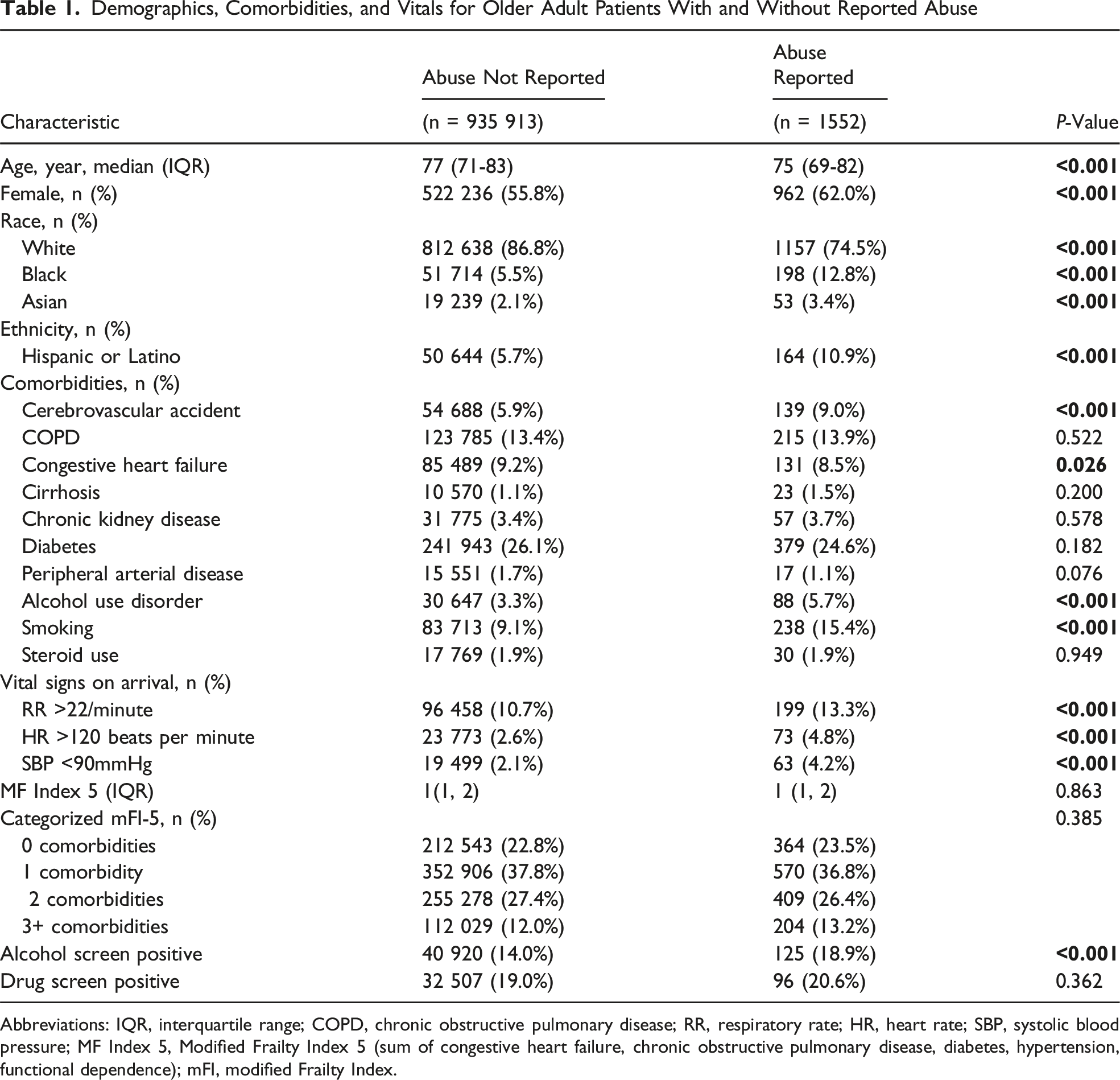
Abbreviations: IQR, interquartile range; COPD, chronic obstructive pulmonary disease; RR, respiratory rate; HR, heart rate; SBP, systolic blood pressure; MF Index 5, Modified Frailty Index 5 (sum of congestive heart failure, chronic obstructive pulmonary disease, diabetes, hypertension, functional dependence); mFI, modified Frailty Index.
Injury Profile for the (+)RA Group vs the (−)RA Group
Injury Profile for Older Adult Patients With and Without Reported Abuse
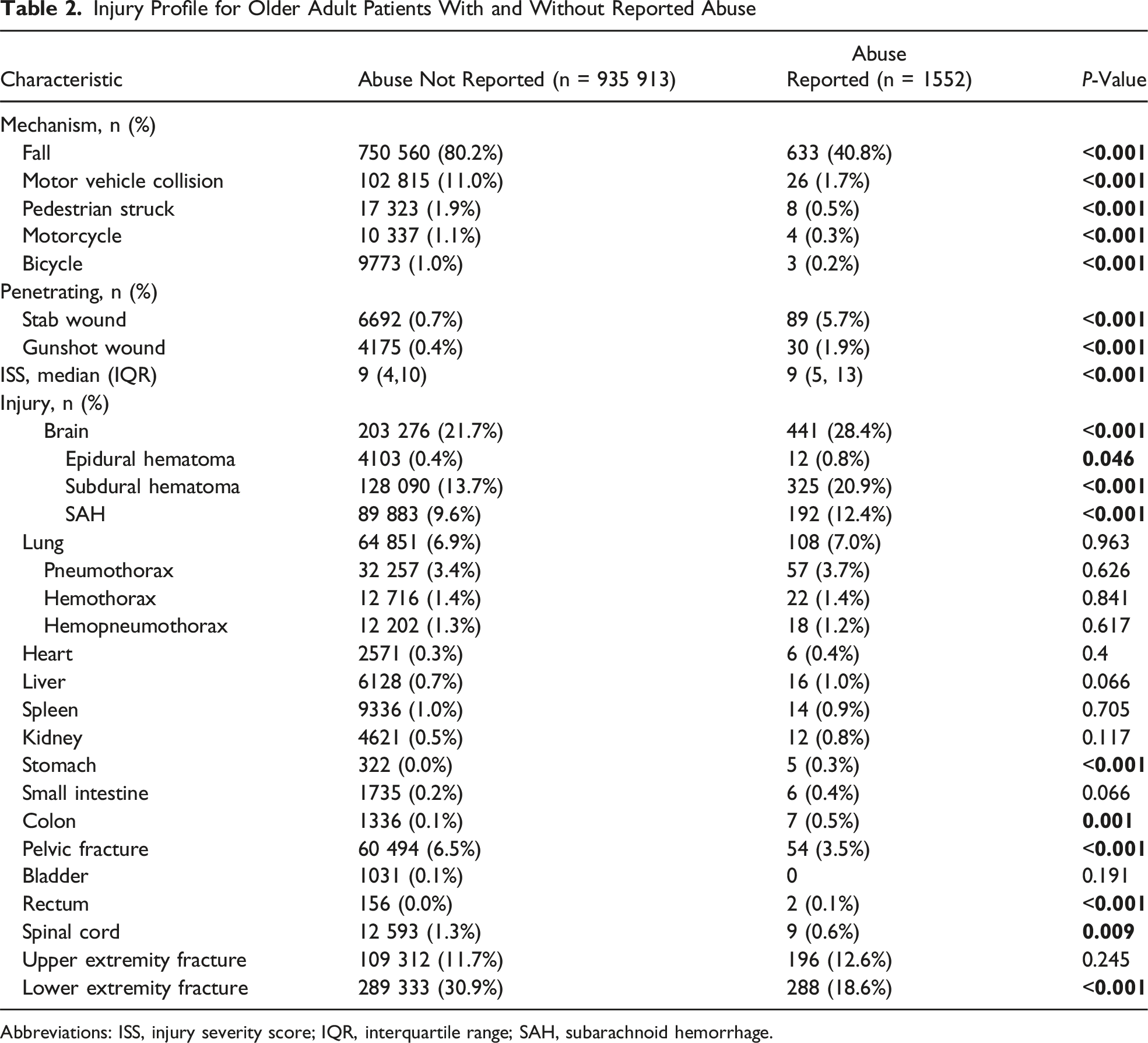
Abbreviations: ISS, injury severity score; IQR, interquartile range; SAH, subarachnoid hemorrhage.
Outcomes and Complications for the (+)RA Group vs the (−)RA Group
Outcomes and Complications for Older Adult Patients With and Without Reported Abuse
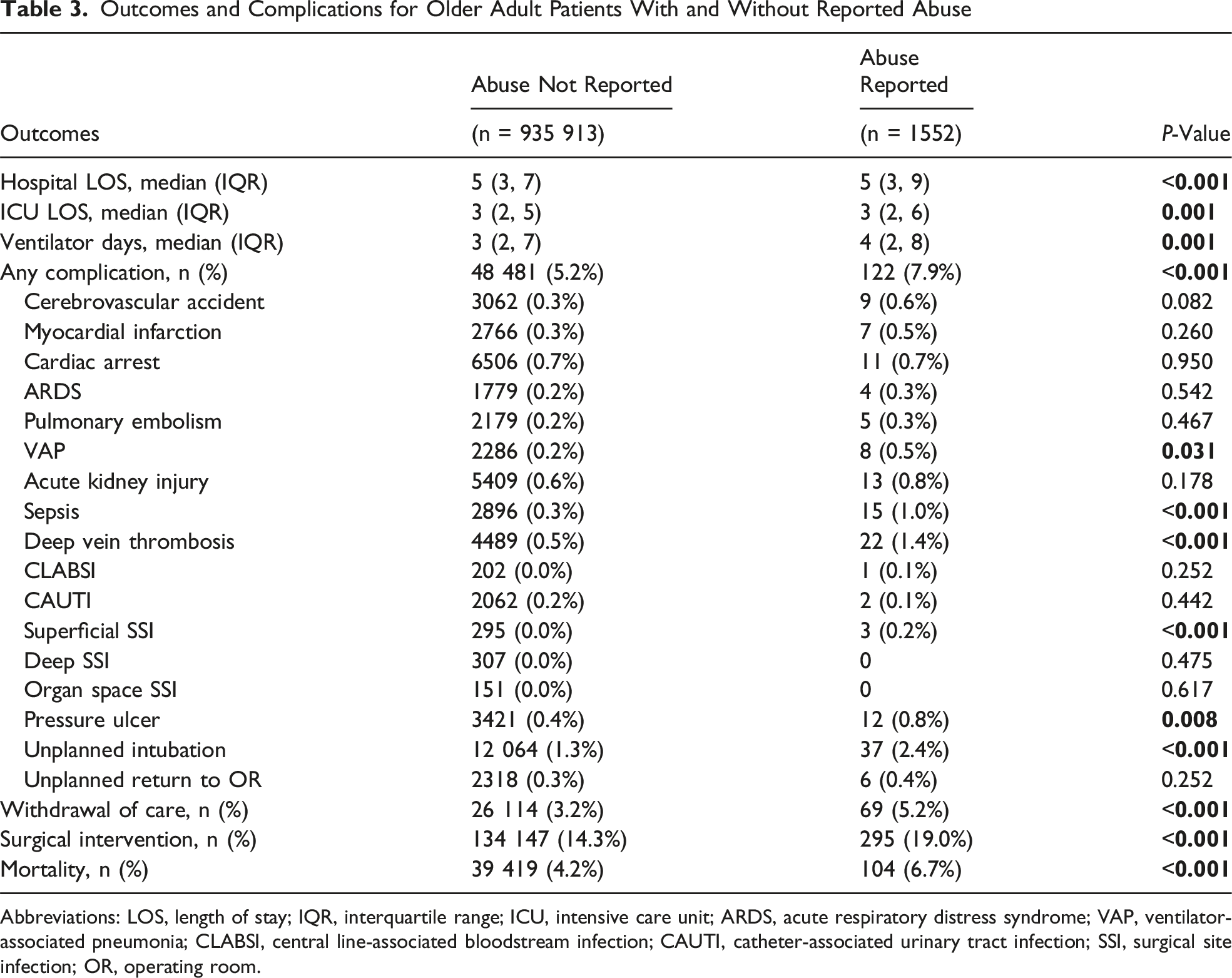
Abbreviations: LOS, length of stay; IQR, interquartile range; ICU, intensive care unit; ARDS, acute respiratory distress syndrome; VAP, ventilator-associated pneumonia; CLABSI, central line-associated bloodstream infection; CAUTI, catheter-associated urinary tract infection; SSI, surgical site infection; OR, operating room.
Multivariable Logistic Regression Analyses for Associated Risk of Complications and Mortality for OA Patients with and Without Reported Abuse
Multivariable Logistic Regression Analysis for Associated Risk of Complications and Mortality of Older Adult Patients With and Without Reported Abuse
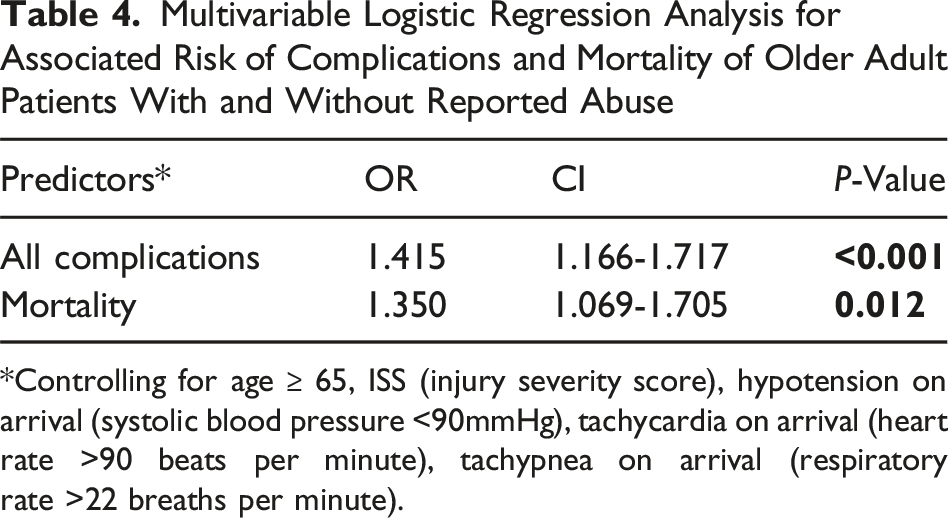
*Controlling for age ≥ 65, ISS (injury severity score), hypotension on arrival (systolic blood pressure <90mmHg), tachycardia on arrival (heart rate >90 beats per minute), tachypnea on arrival (respiratory rate >22 breaths per minute).
Discussion
Recently, the management and outcomes for older adult trauma patients have increasingly become focal points for health research. 2 This national analysis demonstrated that older adult trauma patients with (+)RA experienced higher rates of mortality and increased hospital LOS compared to the (−)RA patients. Additionally, (+)RA patients had higher incidences of penetrating trauma (gunshot and stab wounds). Interestingly, our analysis also demonstrated that despite a clinically similar ISS between cohorts, the (+)RA group had increased rates of complications and surgical interventions.
Mortality is a truly objective and important measure of outcomes for OAs. Dong et al previously found that (+)RA was linked to an increased risk of mortality (hazard ratio = 1.39) among elders in a community setting. 4 Even after the first year, the mortality risk remained elevated for the (+)RA group (hazard ratio = 1.88), highlighting a continued impact of abuse on mortality. 4 Our study of trauma patients similarly found an increased rate of mortality for the (+)RA patients when compared to other older adults. In addition, a systematic review of 19 observational studies previously reported that elder abuse and neglect were associated with risk of death. 7 Several reasons could explain the underlying mechanisms that connect (+)RA to increased mortality. One theory could be that the physiological stress responses induced by abuse can exacerbate existing health conditions and weaken the immune system, making the OAs more susceptible to infections and other health complications. A study by Lachs and Pillemer posited that the chronic stress resulting from abuse triggers a cascade of physiological changes—including elevated levels of stress hormones like cortisol—which may have detrimental effects on the cardiovascular, immune, and endocrine systems, thereby increasing the risk of mortality. 8 Another pivotal aspect worth discussing involves the psychological impact of abuse, which can lead to depression, anxiety, and social withdrawal. 9 Older adult individuals who experience abuse are more likely to exhibit decreased resilience, not only physically but also emotionally and socially, which can further contribute to their mortality risk. 10 In totality, this suggests the need for heightened awareness and screening for elder abuse, as it is a marker of a significant risk of dying within a trauma population as well.
In addition to mortality, due to the increase in elder abuse rates during the COVID-19 pandemic compared to non-pandemic times, 11 as well as increasing trauma volumes and limited space during this difficult time, LOS has become an increasingly important quality metric, especially for vulnerable populations like the (+)RA group. Previous studies on generalized populations suffering from (+)RA have found different variables that may affect hospital LOS among (+)RA patients, including age, comorbidities, and ISS.7,8 Other populations suffering non-accidental trauma (eg, pediatrics) have also demonstrated increased LOS.12,13 These findings may be partly explained by the increased complications and surgical interventions these populations have suffered, which were similar to what the (+)RA population underwent in our cohort. A similar increase in complications and LOS was also found at non-rehab facilities such as skilled nursing facilities. 14 This builds upon prior work by El-Qawaqzeh et al, who noted disparities related to gender, ethnicity, and socioeconomic status of older adult trauma patients with reported abuse. 6 Overall, this highlights the importance of early intervention from social services and case management to facilitate discharge planning for this vulnerable population who suffers from increased morbidity.
Penetrating trauma remains a pervasive mechanism of injury among U.S. patients, including older adults. 15 In our national analysis, older adults with (+)RA presented with gunshot wounds at a rate over eight times that of the (−)RA patients. Similarly, in a study by Rosen et al, (+)RA patients with penetrating injuries had an increased risk of in-hospital death compared to patients with blunt injuries. 16 Penetrating trauma may be associated with additional long-term health consequences such as chronic pain and post-traumatic stress disorder. 15 This association could be due to the prevalence of PTSD among older adults experiencing abuse, which in turn leads to emotional distress and thus escalates to suicidal attempts with firearms. 17 Current U.S. screening practices for elder abuse often focus predominantly on physical and emotional signs, overlooking situational markers such as access to firearms or contextual risk factors, which might prevent recognizing potential abuse scenarios. 18 Enhanced screening protocols that encompass mental health assessments and discussions about firearm access may help mitigate the risk of suicide in this vulnerable population. 19 These discussions should include well studied prevention efforts such as gun locks, safe handling education, and enhanced social support. 20 Incorporating these practices could address the intersecting issues of elder abuse, mental health, and the elevated incidence of penetrating injuries, offering a more holistic approach to patient care and prevention strategies.
This study is subject to several limitations inherent to its retrospective database design, including missing data and coding inaccuracies. Although our study included patients ages 65 and older in accordance with many prior studies evaluating older adult trauma patients,6,7 it is important to note that current federal and many state definitions of older adult abuse now encompass individuals ages 60 and older. Another issue includes the small sample size, which may be partly due to the known problem of underreporting elder abuse. This may affect the results of this study, which only included TQIP participating hospitals, thus the results may not be generalizable to non-trauma centers. While statistically significant differences in outcomes such as ICU LOS and ISS may reflect the large sample size within the TQIP database, even small numerical differences may be clinically meaningful given the resource-intensive nature of trauma care and its implications for health care systems. Additionally, as a retrospective analysis, this study cannot evaluate causality. Furthermore, the study predominantly relies on coded data for the classification of RA, which could lack the nuanced details necessary to fully understand the circumstances and severity of each case, as OAs who had certain cognitive, psychological, or developmental disorders are more vulnerable to abuse. 17 Notably, there is also a lack of granular data concerning the timing and type of neglect/abuse and interventions, which might provide deeper insights into the relationship between RA and trauma outcomes. Finally, the study lacks information related to social determinants of health, which are known risk factors for abuse. These limitations emphasize the need for high-quality, prospective, multicenter studies.
Conclusion
This analysis of the TQIP database spanning three years demonstrated that 0.2% of older trauma patients reported abuse, and the (+)RA group was associated with increased rates of penetrating trauma, longer hospitalizations, and increased in-hospital mortality, compared to (−)RA patients. The results of this study call for further research to explore the reasons for the correlation found between documented elder abuse and higher rates of penetrating trauma, extended hospital stays, and increased mortality. The results also emphasize the importance of enhancing screening procedures in health care environments to quickly detect and handle elder abuse, in order to change the treatment trajectory for these individuals. Finally, there should be more studies on primary prevention for this population as well as the unique requirements and obstacles experienced by mistreated older individuals when it comes to accessing and receiving trauma care, guaranteeing that health care systems are prepared to appropriately address the intricacies of elder abuse.
Footnotes
Ethical considerations
This study was deemed exempt by our Institutional Review Board.
Consent to participate
Written informed consent was waived as this study used a national deidentified database.
Author Contributions
The authors contributed to this work as follows: Jiabao Nie: Conceptualization and study design; interpretation of the analysis; initial drafting of the manuscript; critical revisions and final approval. Areg Grigorian: Conceptualization and study design; statistical analysis; interpretation of the analysis; critical revisions and final approval. Negaar Aryan: Conceptualization and study design; interpretation of the analysis; critical revisions and final approval. Nicholas Truong: Conceptualization and study design; interpretation of the analysis; critical revisions and final approval. Catherine Kuza: Conceptualization and study design; interpretation of the analysis; critical revisions and final approval. Sigrid Burrus: Conceptualization and study design; interpretation of the analysis; critical revisions and final approval. Jeffry Nahmias: Conceptualization and study design; interpretation of the analysis; critical revisions and final approval; oversight and supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.