
Abstract
Introduction
Verification by the American College of Surgeons and state designation of trauma centers improve outcomes in trauma care. In regions where participation in trauma systems is optional, legislation requiring inclusion may need evidence of outcome differences. Given the distinct populations treated at trauma centers vs non-trauma centers, validated risk adjustment is essential for fair comparison. The International Classification of Diseases, 10th Revision injury severity score (ICISS) has been validated for such assessments.
Methods
With institutional review board approval, data from the state Healthcare Cost and Utilization Project from 2018 to 2020 was analyzed. Using ICISS for risk adjustment, outcomes were compared across overall, age-specific, and diagnosis-specific groups.
Results
Among 3,316,016 discharges, 245,404 (7.4 percent) included at least one injury diagnosis. After excluding transfers out, 151,855 cases remained. Patients at trauma centers had lower risk-adjusted mortality and fewer occurrences of acute kidney injury and pulmonary embolism but higher rates of ventilator-associated pneumonia and surgical site infections. Subgroup analyses revealed that pediatric patients and those with traumatic brain injuries or shock were predominantly treated at trauma centers. Increased age, higher injury severity, male gender, and non-trauma center treatment were associated with lower survival rates. Among geriatric patients with proximal femur fractures, 63 percent were treated at non-trauma centers, with no observed mortality benefit from trauma center care.
Conclusions
Trauma center care is associated with improved outcomes supporting the development of more inclusive trauma systems.
Introduction
The American College of Surgeons(ACS) verification process and state regulatory designation of trauma centers are tools utilized to evaluate and optimize outcomes in the care of injured patients. The ACS offers an outside evaluation process for state performance in caring for injured patients. Many states evaluate individual hospital performance as part of their statewide quality assessment. Hospital participation in organized statewide trauma systems is variable, with some states encouraging voluntary participation and others mandating involvement as part of hospital licensure requirements. Inclusive trauma systems, where an integrated model of care is deployed in a region with broad and regulated hospital participation at the level of their capabilities, have evidence supporting better performance than non-inclusive systems. 1 Performance at non-trauma facilities is variable. The transition to an inclusive system has improved regional outcomes except in older patients.1-12 We describe our state’s trauma system in Appendix A. Evaluation and comparison of outcomes on a regional basis can be used to inform regulatory agencies on the need for system redesign if outcomes from hospitals participating in organized injury care can be superior. Trauma registries and participation in national quality improvement activities serve as a source of data for comparing trauma centers but often exclude non-trauma centers. The State Inpatient Database(SID), from the family of Healthcare Cost and Utilization Project(HCUP) databases, a federal-state-industry partnership sponsored by the Agency for Healthcare Research and Quality(AHRQ), collects ICD-10 discharge codes, procedure codes, patient demographics, and length of stay from all licensed facilities in participating states. 13 An ICD-10-based injury severity score(ICISS) utilizing a multiplicative approach has been previously validated. 14 In addition, improvement in the predictive value of ICISS with the incorporation of diagnosis codes for comorbidities has been explored.15,16 Based on available evidence, ICISS can reasonably be used for risk adjustment to compare hospital performance between pooled patients treated at trauma centers and non-trauma centers.
This study is part of a statewide push to assess the quality of care provided in our trauma system. Because non-trauma centers are not required to submit data to the State Trauma Registry or the National Trauma Databank, we aimed to compare risk-adjusted morbidity and mortality between trauma centers and non-trauma centers in our state using our SID and AHRQ-HCUP. We hypothesized that patients treated at trauma centers would have improved morbidity and mortality outcomes compared to those at non-trauma centers after appropriate risk adjustment.
Methods
A local Institutional Review Board approved this retrospective study. We included patients with at least one injury diagnosis, complete survival information, and discharge from a state-licensed facility between January 2018 and December 2020. All patient discharge data were retrieved from the SID and HCUP from the AHRQ. Hospital ID was used to designate each facility as a trauma center(TC) or non-trauma center(NTC). Patient and facility identifiers were removed and not included in the analysis.
Data Collection
The SID for the study period contained 3,316,016 records, of which 245,404(7.4%) had at least one ICD-10 code with the prefix S00-T19 and were selected for this study. Of selected patients, 59.5% were from TC and 40.5% from NTC. The variables of interest for this study included demographic information, diagnosis codes, complications, and hospital disposition. Patient demographics included age, gender, and race. Two ICISS-based scores were used as an alternative to ISS to address injury severity. For our calculations of ICISS-based scores, we first created a data set with survival risk ratios(SRR) for each ICD-10 code from S00 to T19 and then, utilizing a multiplicative approach, calculated an individual patient score as a product of all the patients’ ICD-10 based SSRs which we designated “ICISS-t” indicating the exclusive use of trauma-related ICD-10 codes.
Since comorbidities may impact a patient’s prognosis for recovery from an injury, a second ICD-10-based severity score was calculated, including ICD 10 scores for comorbidities, A00-T88, U071, and Z16, designated “ICISS.” This score (ICISS) was calculated using the same methodology as ICISS-t, except we utilized ICD-10 diagnosis codes for comorbidities and injury-based codes. 15 The top 20 trauma and top 20 comorbidity codes and their SRRs used for ICISS calculations are listed in (Appendix B).
Diagnosis codes were also utilized to identify the diagnosis groups for femur fractures, traumatic brain injuries(TBI), shock, and complications. Femur fractures included head/neck, lower end, other, pertrochanteric, shaft, subtrochanteric, and unspecified. Complications included acute kidney injury, ventilator-associated pneumonia, pulmonary embolus, and surgical site infection. Outcomes of interest were hospital length of stay(HLOS) and mortality.
Analyses were performed using the SAS software version 9.4 (SAS Institute, Cary, NC). Study groups were defined dichotomously according to trauma center designation, TC vs NTC. Overall comparisons included age, ICISS, ICISS-t, HLOS, survival, gender, race, and transfer status. X2 tests or Fischer’s exact tests assessed associations among categorical variables. Continuous variables were compared using Student’s t test and Mann-Whitney U test for parametric and nonparametric data, respectively. Mortality rates were compared for TCs vs NTCs overall for a specific diagnosis, fracture types, and complications. Multiple logistic regression was used to evaluate the likelihood of survival overall and complications while considering the influence of factors such as age, ICISS, ICISS-t, gender, race, and trauma center status. Subgroup analyses were performed by age group (pediatric, non-geriatric adult, geriatric) and diagnosis(femur fracture subgroups, TBI) for mortality and complications. Statistical significance was defined as P < 0.05.
Artificial Intelligence (AI) Statement
We used Chat GPT 4o(OpenAI, San Francisco, CA, USA) solely to assist with proofreading and language editing. We did not use AI tools to collect, create, or analyze data.
Results
There were 3,316,016 discharges identified for the study period, of which 245,404(7.4%) had at least one injury diagnosis code and complete survival information. Records of patients transferred out of the hospital were excluded(due to unknown final disposition), leaving 151,855 to be included in the primary analysis. 93,549 patients were transferred out, and 19,418 patients were transferred in. To avoid duplication, only patients transferred in were subjected to further analysis.
Demographics & Characteristics of Trauma Patients Presenting From the Field (ie, non-Transfers)
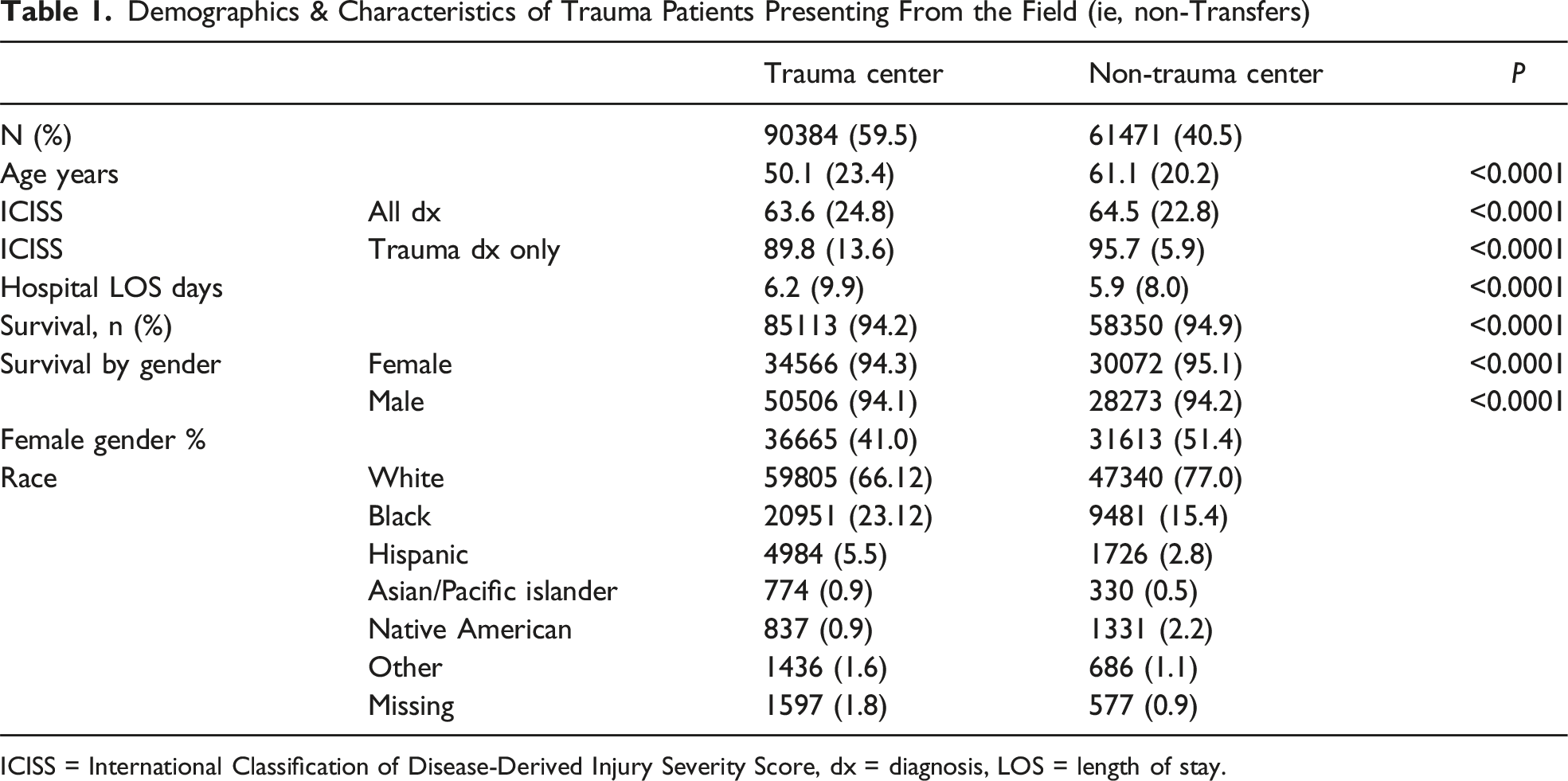
ICISS = International Classification of Disease-Derived Injury Severity Score, dx = diagnosis, LOS = length of stay.
Multiple Logistic Regression
Multiple Logistic Regression of Overall Survival for Trauma Discharges NC 2018-2020 Excluding Transfers out. (n = 149635)
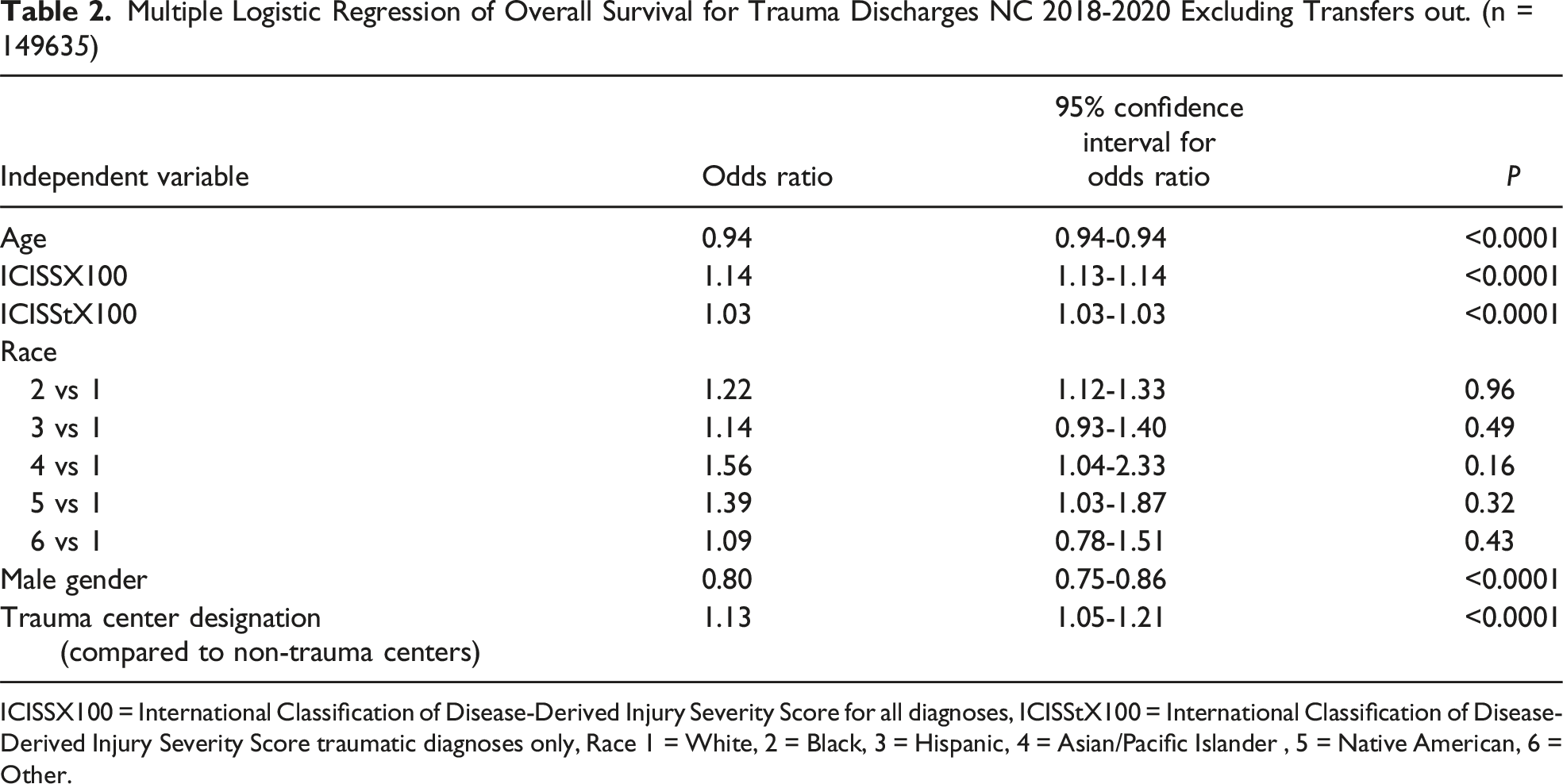
ICISSX100 = International Classification of Disease-Derived Injury Severity Score for all diagnoses, ICISStX100 = International Classification of Disease-Derived Injury Severity Score traumatic diagnoses only, Race 1 = White, 2 = Black, 3 = Hispanic, 4 = Asian/Pacific Islander , 5 = Native American, 6 = Other.
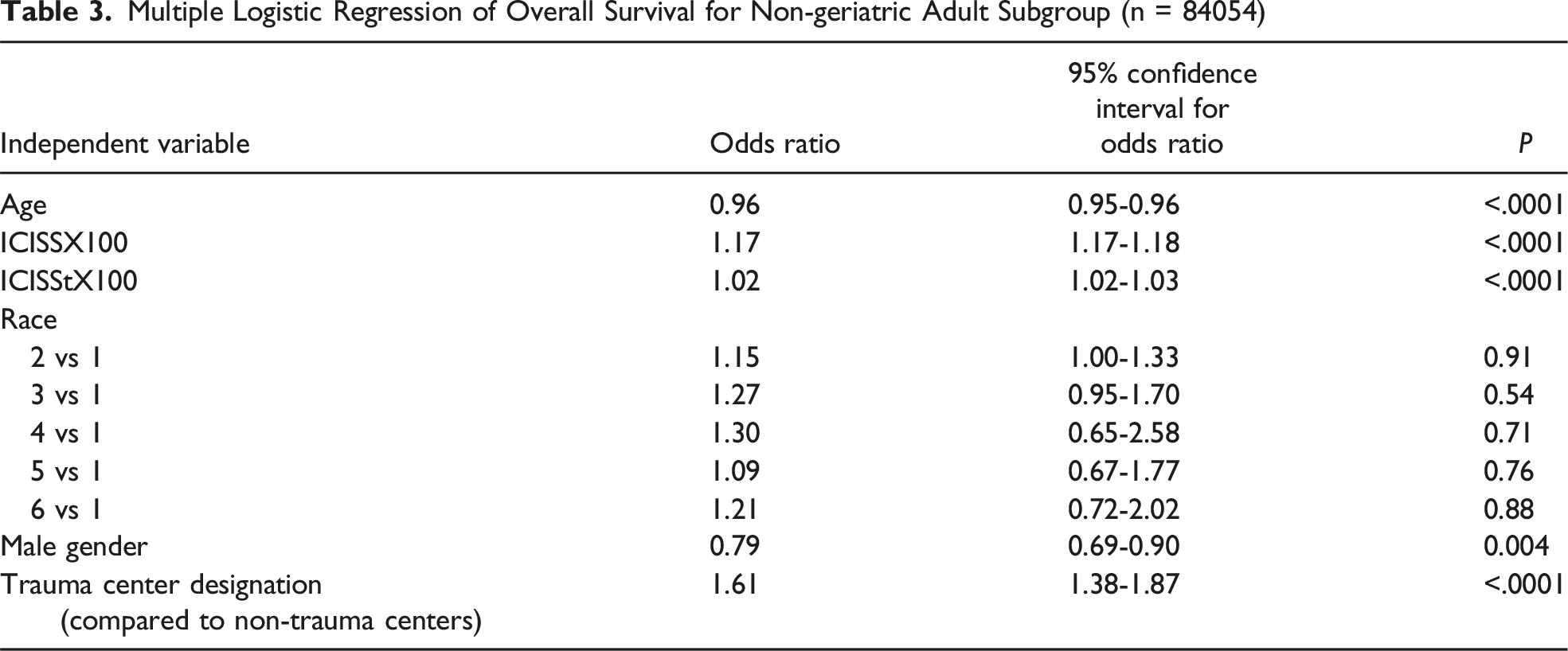
Multiple Logistic Regression of Overall Survival for Non-geriatric Adult Subgroup (n = 84054)
Injuries and Complications by Age Group, Stratified by Trauma Center Status
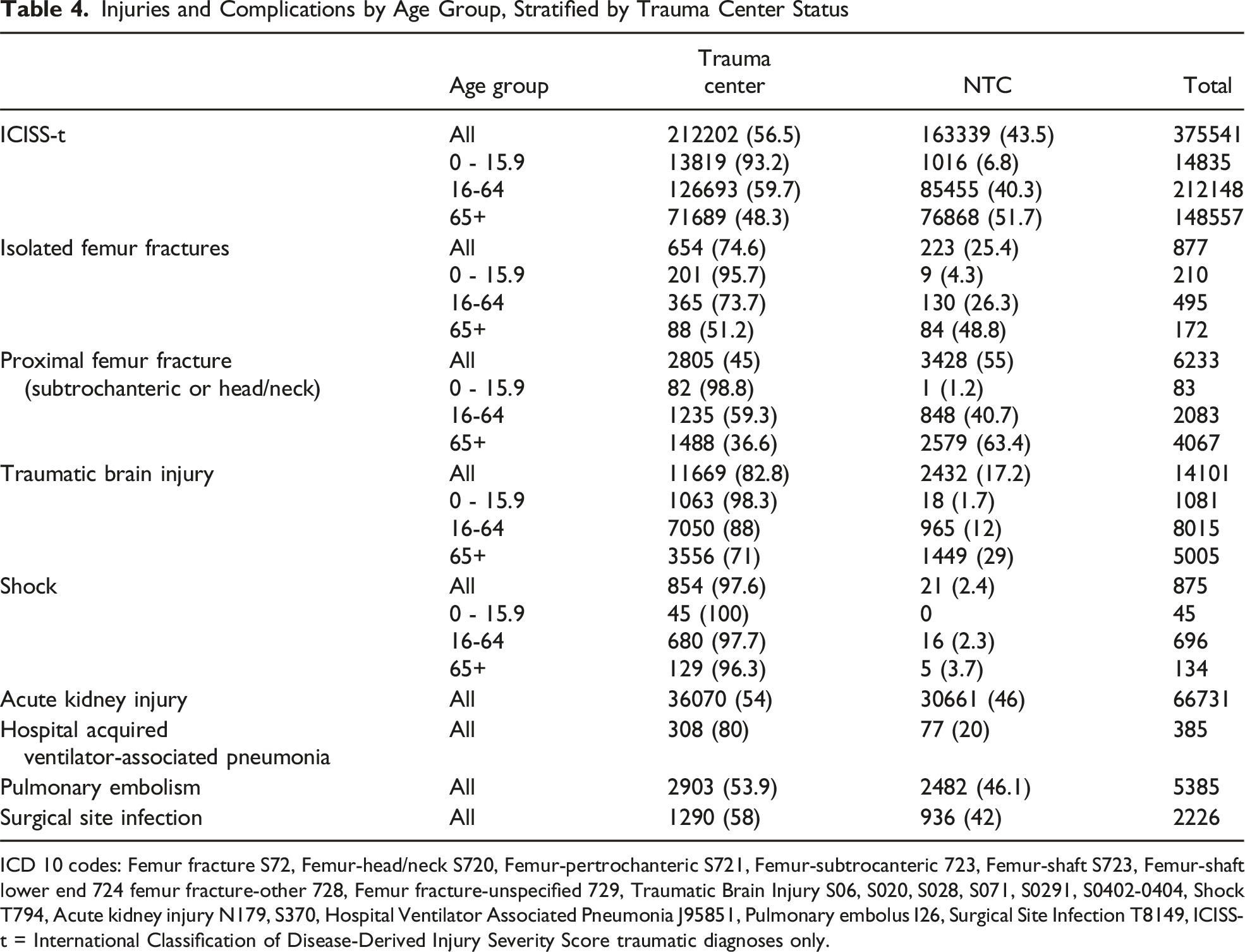
ICD 10 codes: Femur fracture S72, Femur-head/neck S720, Femur-pertrochanteric S721, Femur-subtrocanteric 723, Femur-shaft S723, Femur-shaft lower end 724 femur fracture-other 728, Femur fracture-unspecified 729, Traumatic Brain Injury S06, S020, S028, S071, S0291, S0402-0404, Shock T794, Acute kidney injury N179, S370, Hospital Ventilator Associated Pneumonia J95851, Pulmonary embolus I26, Surgical Site Infection T8149, ICISS-t = International Classification of Disease-Derived Injury Severity Score traumatic diagnoses only.
The patients diagnosed with shock did not fare significantly better at trauma centers, although few patients in this category were treated at a non-trauma center. We found no significant difference in mortality when comparing White patients to other minorities.
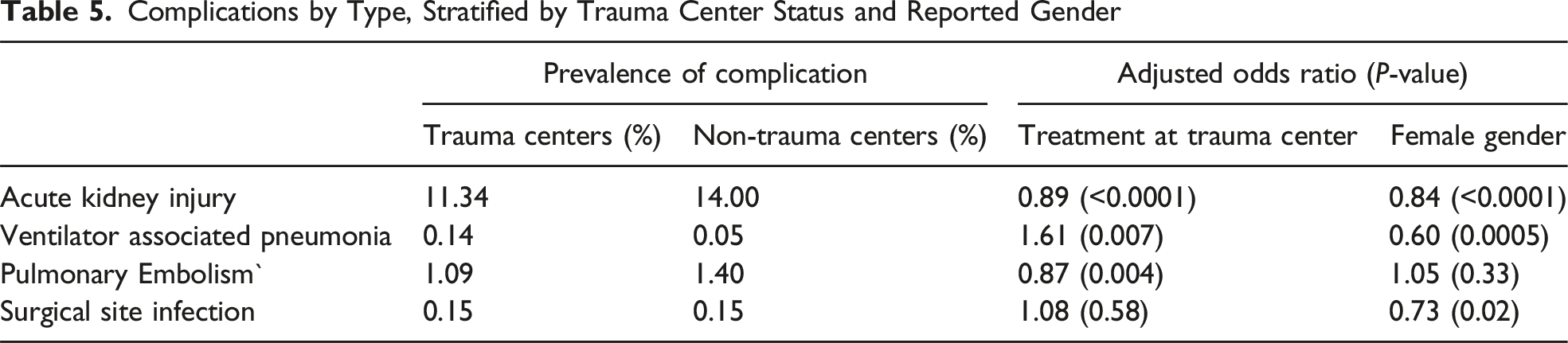
Complications
Complications by Type, Stratified by Trauma Center Status and Reported Gender
Transferred Patients
Secondary Analysis for Survival in Patients Transferred From Another Hospital. N = 19418 Multiple Logistic Regression for Mortality Among Patients Transferred Into Trauma Centers
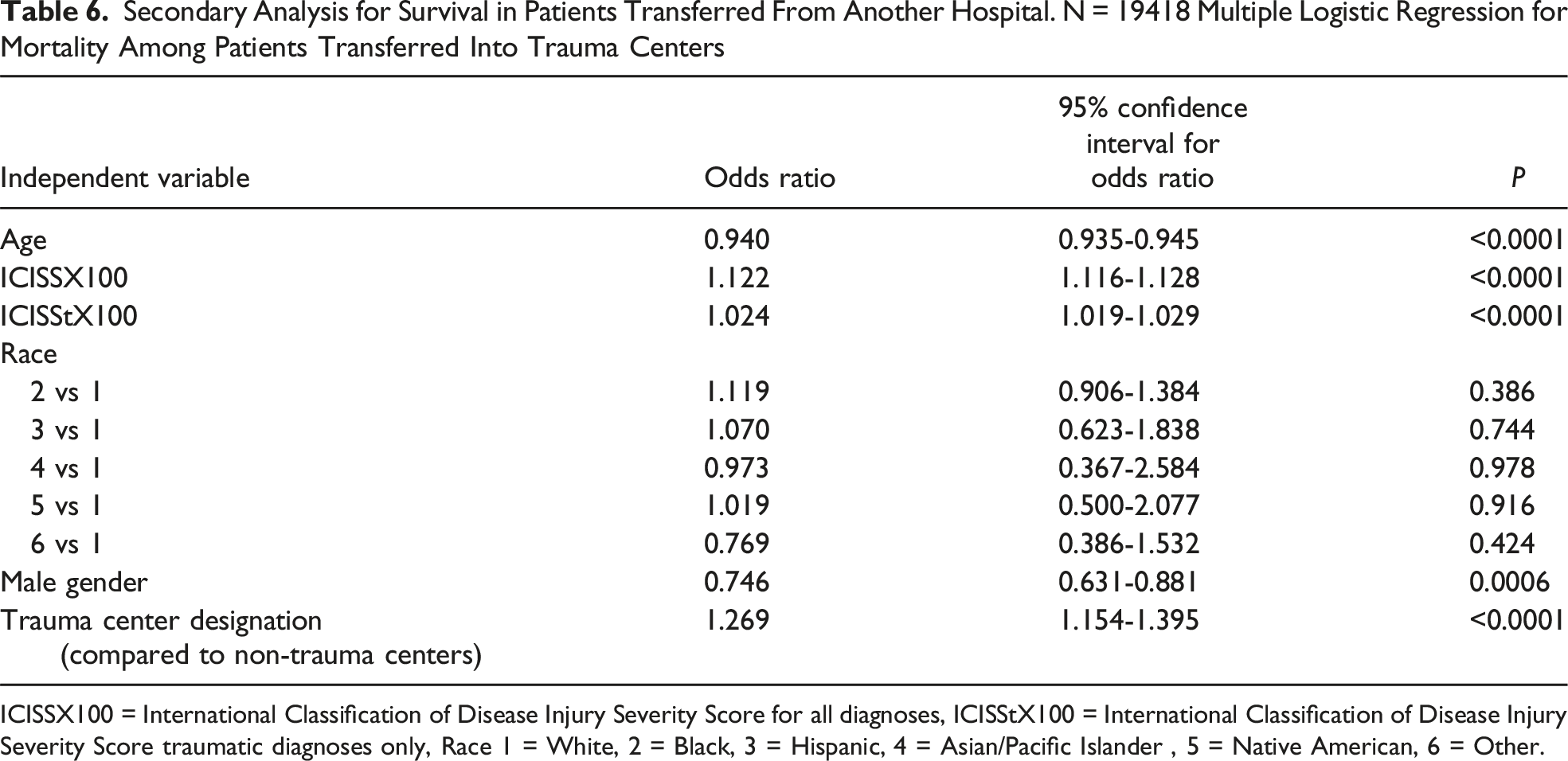
ICISSX100 = International Classification of Disease Injury Severity Score for all diagnoses, ICISStX100 = International Classification of Disease Injury Severity Score traumatic diagnoses only, Race 1 = White, 2 = Black, 3 = Hispanic, 4 = Asian/Pacific Islander , 5 = Native American, 6 = Other.
Discussion
Our study was prompted by a state initiative to evaluate and enhance a trauma system established over 40 years ago on a voluntary basis. Participating institutions submit standard data to the State Trauma Registry, while ACS-verified trauma centers provide similar data to the National Trauma Data Bank and ACS-TQIP. However, there is no requirement for non-trauma centers to collect and analyze injury-specific information.
Under the Medical Care Data Act, all licensed hospitals must submit a limited data set to a statewide database within 60 days after each quarter. This data includes demographic information, third-party coverage, diagnoses, procedures, length of stay, cost data, and hospital identifiers. It forms the basis for state HCUP data, which may vary between institutions, depending on coding and data quality practices.
Given the links between coding accuracy, reimbursement, and quality penalties, healthcare institutions strive for data precision. 17
Diagnosis, procedure, and complication codes follow ICD-10-CM and ICD-10-PCS standards. The ICISS, derived from ICD-10-CM, enables risk-adjusted outcome comparisons. This project uses ICISS to evaluate pooled outcomes between state-designated trauma centers and other licensed hospitals, identifying care gaps for potential improvements in the statewide trauma system. The initiative also explores the feasibility of linking data from prehospital care to rehabilitation, with expanded requirements for physiological data.
EMS in our state are organized by county and follow statewide protocols modified by local directors. There is no standardized process for classifying injured patients or transporting them to specialized care, and resources at both the EMS and hospitals determine these decisions. Currently, there is no comprehensive system to audit patient destinations or quality outcomes. The HCUP hospital discharge data is the only consistent source for comparing outcomes across all state hospitals.
Demographics, Injury Subgroups, and Treatment Location
Our study analyzed 151,855 patients with injury diagnoses in a state of approximately 10.7 million over three years, with 59.5% treated at trauma centers (TC). Trauma centers treated younger, more severely injured, and more minority patients, and survival rates were influenced by age, injury severity, gender, and TC treatment. Notably, 88% of pediatric patients were treated at TCs, while only 73.7% of nongeriatric and 51.2% of geriatric adults with isolated femoral shaft fractures were. For traumatic brain injuries(TBI), 88% of nongeriatric adults and 71% of geriatric adults received TC treatment. TC admission significantly improved TBI survival but not for isolated or geriatric proximal femur fractures. With 117 hospitals and 17 TCs in the state, there is insufficient capacity to redirect all patients, and our findings suggest high-risk injuries like TBI and pediatric cases already receive optimal care. Subgroup analyses indicated that factors like time to treatment and severity of shock may affect outcomes, with compliance to care standards potentially explaining the lack of mortality benefits in certain cases.19,21
Comorbidities’ impact on outcomes in geriatric proximal femur fractures is not disputed; mortality is an indeterminate quality measure given the roles that predetermined goals of care and limitations placed on care teams in the context of physical frailty and dementia. Our study did not demonstrate improved outcomes for geriatric patients with proximal hip fractures, the majority of whom were treated at NTC, while showing a reduced risk of death overall in geriatric patients.
Standardized treatment at NTC for retained patients may be comparable to treatment at trauma centers. System under-triage, the delivery of injured patients to a location with less desirable outcomes, may exist in some categories or combinations of diagnoses. While there is no rationale for centralizing the treatment of all injured patients at trauma centers or making all hospitals trauma centers (TC), there is a rationale for collecting more robust outcomes information from NTC to define where system improvements could be sought.
While hospital mortality rates and a few hospital complications may suggest better quality care, they do not provide a complete view. Comprehensive measures, such as 30- or 60-day mortality rates and patient-reported quality of life, are essential. An inclusive system with standardized data requirements—including physiological data and treatment times—would improve performance measurement and enable accurate risk-adjusted outcomes across all acute care facilities.
Our study’s weaknesses include the exclusion of some transfer patients to avoid duplication, as the dataset lacks unique identifiers and treats all discharges as separate events. This exclusion limits the target population and impairs a comprehensive analysis of the state system. Additionally, the HCUP data lacks information on time to treatment, prehospital interventions, and patients’ clinical severity upon arrival, hindering the comparison of patient populations. However, analyzing transferred-in patients indicates an independent benefit from TC treatment.
Concerns regarding multicollinearity were addressed with an estimated correlation matrix demonstrating only a weak correlation(-0.1235) between ICISS and ICISS-t, which have some shared derivation.
Finally, the processes for collecting and entering diagnosis codes into the state inpatient database by non-clinical coders for administrative or billing purposes, with limited clinical validation, can raise accuracy concerns.
Despite these limitations, our findings from the SID and AHRQ-HCUP databases show the value of including NTC when evaluating the care of injured patients within our trauma system. The reality is that a significant portion of injuries are treated at NTC, and developing an inclusive trauma system that encourages system-wide data collection beyond TCs will help identify injury patterns that can be better served at NTC vs those that are better suited for transfer to a TC. Implementing an inclusive system with data requirements allows us to identify disparate outcomes to facilitate the retention or transfer of injured patients (such as in TBI). 22 Regional evidence must be made available through collaborative efforts such as this to ensure quality.
Conclusion
Our study demonstrates the need for uniform information from participating institutions in regional trauma care to assess trauma system performance, and that comparisons in outcomes in subgroups can serve to direct system performance improvement. Not all trauma center (TC) patient subgroups saw improved outcomes, justifying the retention of those patients at non-trauma centers (NTC). Our study justifies developing an inclusive system where non-trauma centers participate in regional data collection, planning, and performance improvement to ensure optimal system triage and improvement initiatives.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SS is partially funded by the North Carolina Office of Emergency Medical Services.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.