
Abstract
Resuscitative efforts (RE) for patients suffering cardiac arrest following trauma require significant prehospital (PH) and hospital resources. Patients who are transported and undergo immediate termination of resuscitative efforts (ITRE) and declared dead on arrival (DOA) may represent a population for whom improved triage can conserve hospital resources.
• A quarter of all transported patients following traumatic arrest have resuscitative efforts terminated in the emergency department. • Patients who suffer a blunt MOI, are older, and undergo fewer prehospital interventions, are more likely to undergo immediate termination of resuscitative efforts.Key Takeaways
Introduction
Patients who suffer cardiopulmonary arrest following trauma, otherwise referred to as traumatic full arrest (TFA), face a grim prognosis overall and incur significant costs to health care systems and providers. The mortality of patients following TFA has been reported as high as 95%.1,2 While clinical variables such as age, witnessed arrest, initial shockable rhythm and amount of administered epinephrine have been identified as factors associated with a favorable long-term outcome in patients suffering non-TFA, a similar understanding of prehospital (PH) variables that predict successful resuscitation efforts is less well-defined in the trauma literature. 3
Patients who are declared deceased on arrival (DOA) with immediate termination of resuscitative efforts (ITRE) [DOA/ITRE] in the emergency department may represent a population for whom the field termination of resuscitative efforts could conserve hospital resources. Prior work has identified that patients without a respiratory rate or systolic blood pressure and a Glasgow Coma Scale (GCS) of 3 should be declared on-scene and not be transported to a hospital as this would be futile and an overuse of resources.4-6 Controversy exists in the literature as to whether to favor physiologic or time-based factors when determining how to triage patients with TFA; hospital-based algorithms from the Eastern Association for Trauma (EAST) and the Western Trauma Association (WTA) differ with respect to these paradigms.7,8 While both associations discuss the factor of timing since injury and the type of mechanism, WTA suggests a more algorithmic plan towards whom should receive a resuscitative thoracotomy (RT) while EAST relies heavily on the presence or absence of signs of life as well as the mechanism to make more broad recommendations about consideration of RT.7,8 Currently, there are no agreed-upon national PH criteria that can more effectively triage patients with prehospital traumatic full arrest (PH TFA). 9 Current guidelines vary by locality (city, county, or state) and patient triage can be based off vital signs, mechanism of injury, or EMS judgment, though adherence to these guidelines is not well established in the currently published literature.10,11
The aim of this study was to identify PH variables associated with DOA/ITRE following TFA. In addition, we sought to describe our single-center experience with patients arriving in extremis undergoing prehospital CPR (PHCPR) to better understand our current use of hospital resources in the care of these patients. We hypothesize that physiologic variables obtained at the point of contact with PH personnel can better identify patients unlikely to benefit from transport and RE, thereby allowing conservation of both PH and hospital-based resources.
Methods
We retrospectively queried data from our Level 1 urban trauma center registry for all patients aged 15 years or greater who suffered a TFA and underwent PHCPR from 2014 to 2023. Patients aged 15 to 18 years old were included in our patient cohort, as these patients are triaged and managed nearly identically to patients aged 18 years or older in our hospital, and occasionally accurate patient age is unknown prior to arrival. We collected patient demographics (sex, age, and race/ethnicity) and details of PH timeline (time to and on scene and transport time from scene to hospital) as well as PH clinical data, including interventions (field intubation, needle thoracostomy, and intraosseous (IO) access). We compared PH records with hospital records to assure accuracy. Details regarding resuscitation efforts (RE) in the Emergency Department (ED), including blood product transfusion volume, chest tube insertion, endotracheal intubation, placement of central venous access, and surgical interventions, including RT and use of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA), were collected. Other data gathered included mechanism of injury, Abbreviated Injury Score (AIS), and presenting signs of life (SOL). Patients were reviewed to determine if they met inclusion criteria from the WTA or EAST for RT.
The primary outcome of interest was declaration of DOA/ITRE which we defined as patients transported who underwent no additional procedural interventions in the ED. Of note, point of care ultrasound (POCUS) was considered a confirmatory test of death to rule out any cardiac activity and was not considered a RE in this study. Deidentified data was collected into an Excel database (Microsoft Excel, Microsoft Corp). Statistical analysis was conducted using both SAS version 9.4 (SAS Institute) and EpiInfo7 (Centers for Disease Control, Atlanta). Continuous variables were compared with the Wilcoxon rank sum test, while categorical variables were compared with X2 or Fisher exact test, as appropriate. A 2-sided P < 0.05 was statistically significant. Multivariable logistic regression was performed to identify independent associations between PH variables and the outcome of interest (DOA/ITRE) using variables identified by univariate analysis. This study was deemed exempt by the Lundquist Institute Institutional Review Board.
Results
Demographics of Participants
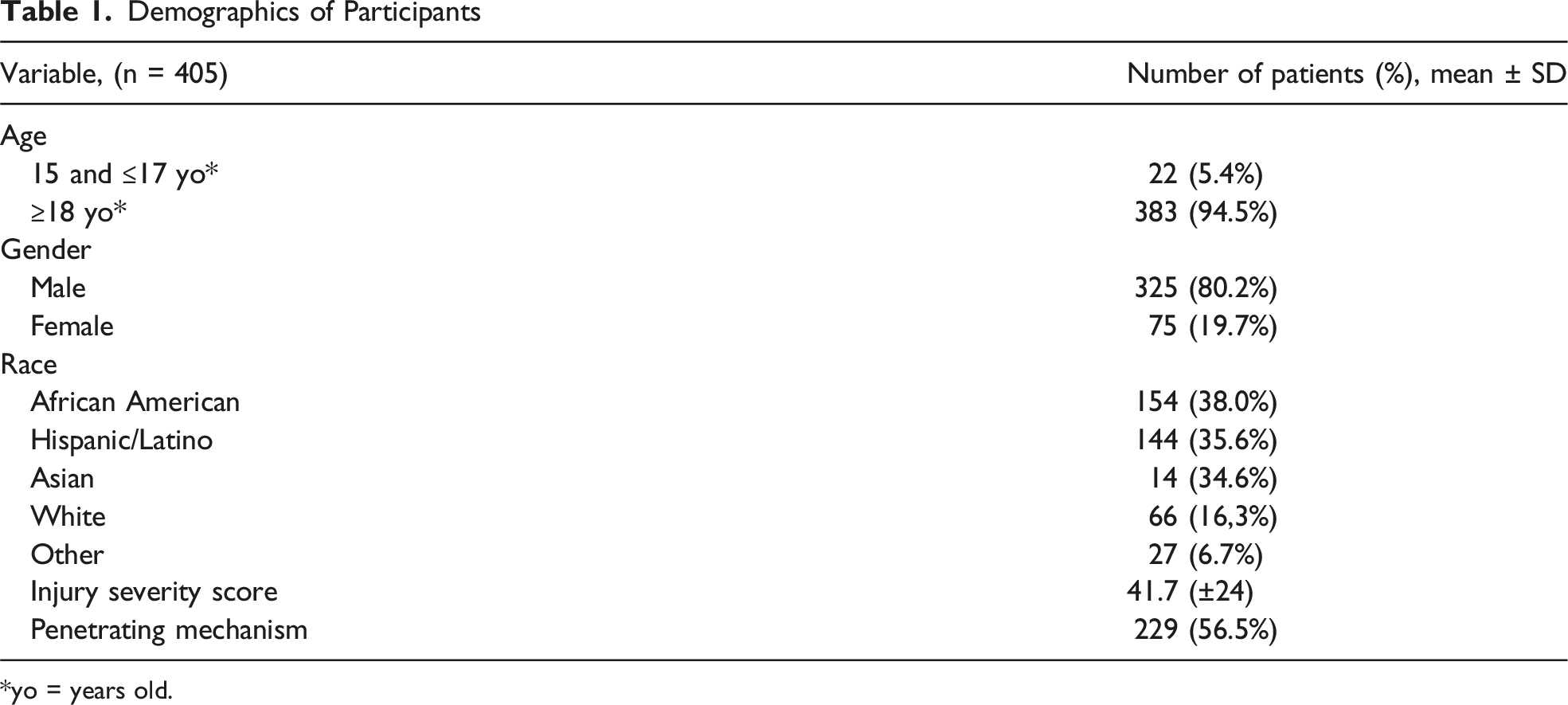
*yo = years old.
Prehospital Resuscitation Efforts
CPR = prehospital cardiopulmonary resuscitation.
Clinical Variables of Patients
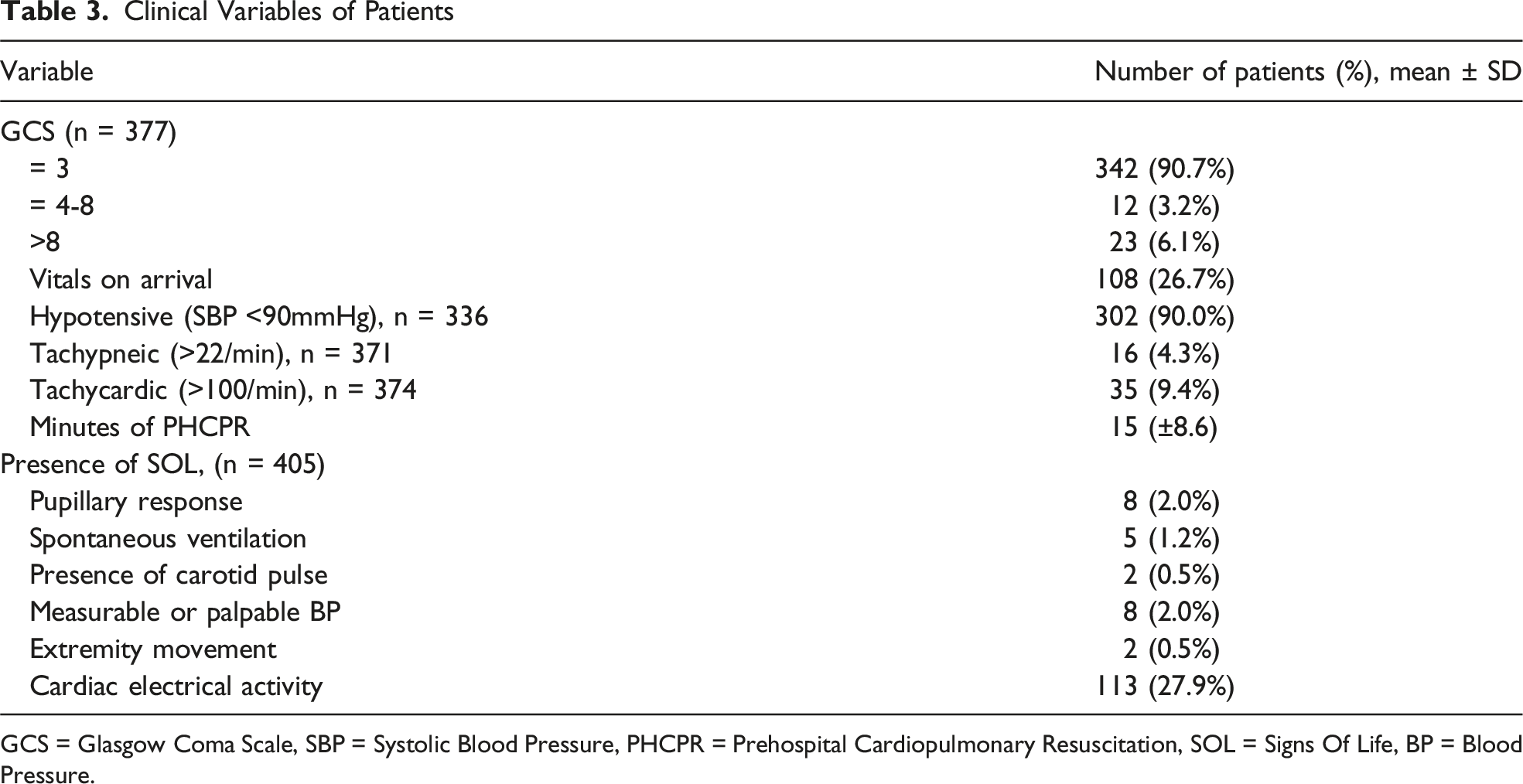
GCS = Glasgow Coma Scale, SBP = Systolic Blood Pressure, PHCPR = Prehospital Cardiopulmonary Resuscitation, SOL = Signs Of Life, BP = Blood Pressure.
Most patients presented with a GCS of 3 (90.7%) and were hypotensive (89.99%) (Table 3). Among this cohort, 124 patients (30.6%) presented with at least 1 sign of life; the most common was electrical cardiac activity (n = 113, 27.9%) (Table 3). Less than 2% of the patients were noted to have pupillary response, spontaneous ventilation, presence of carotid pulse, a measurable blood pressure, or extremity movement at the time of presentation to the ED.
A total of 102 (25.2%) patients were DOA/ITRE; these patients tended to be older (42.5 [29-53] vs 37.6 [24-47], P = .0.0095). These patients were more also more likely to have a blunt MOIs (52/176 patients (29.6%) vs 50/229 patients (21.8%), P = 0.007), and less likely to have PH interventions (30.3% vs 69.7%, P = 0.004). The use of POCUS between DOA/ITRE and those with ED resuscitation efforts was not statistically different.
Met Inclusion Criteria for WTA or EAST Guidelines
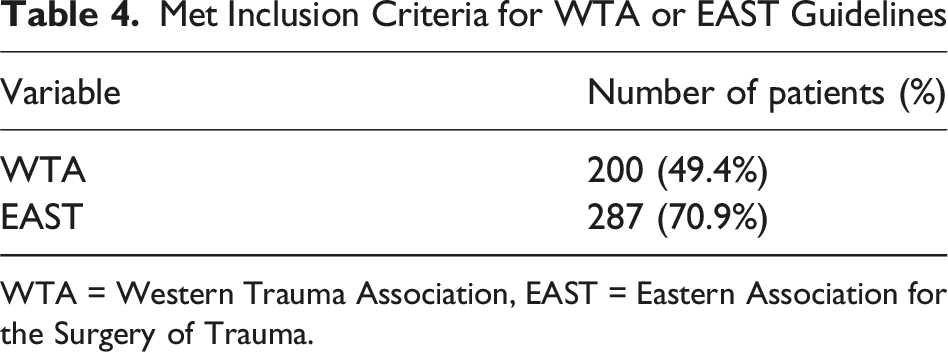
WTA = Western Trauma Association, EAST = Eastern Association for the Surgery of Trauma.
After performing a univariate analysis, we conducted a multivariable logistic regression to attempt to identify PH factors associated with ITRE. Included in this model were age, PH airway, other PH interventions, minutes of PHCPR, and mechanism of injury (blunt vs penetrating). On analysis, no single factor was found to be predictive of ITRE among this cohort.
Discussion
In this single institution study, we found that more than 25% of transported patients following TFA are declared DOA/ITRE once they arrive to the hospital. Our findings highlight that these patients were more likely to have a blunt MOI, be older, and undergo fewer PH interventions. Although multivariable analysis did not demonstrate 1 individual variable associated with ITRE, this series does highlight the ongoing need for increased collaboration with our PH colleagues. In addition, future research in this area would help better delineate which patients are most likely to benefit from PH transport following traumatic arrest. These results reinforce the need to identify PH variables associated with decreased likelihood of survival, which in turn can improve both PH triage guidelines as well as help refine hospital-based protocols for additional interventions in those suffering traumatic full arrest.
Our study shows that <2% of the patients were noted to have pupillary response, spontaneous ventilation, presence of carotid pulse, a measurable blood pressure, or extremity movement at the time of presentation to the ED; however, almost 30% were noted to have cardiac electrical activity. Currently, WTA or EAST do not clarify which type of cardiac activity is a predictor for overall favorable outcomes.7,8 In a single-center study, Martin et al 12 describes that PEA does not predict a favorable outcome for blunt trauma patients. Likewise, in a large multi-center study from Denmark, Wolthers et al found that an initial shockable rhythm was associated with a favorable outcome in TFA patients. 13 Given that for most of the patients in our cohort the only reported sign of life was cardiac electrical activity and given the established literature supporting the idea that PEA is an unfavorable cardiac rhythm for TFA patients, this calls into question whether further stratification of the type of cardiac rhythm should be included in future PH or hospital-based guidelines.
In our study, those who were declared DOA/ITRE were more likely to have fewer PH interventions. Previous data has demonstrated that patients suffering blunt MOIs and those who underwent fewer PH interventions were more likely to have ITRE. 9 This is consistent with our own findings, where we observed a markedly higher rate of ITRE for patients with a blunt MOI as compared with a penetrating MOI (52/176 patients (29.6%) vs 50/229 patients (21.8%), P = 0.007). We also observed that this ITRE cohort was less likely to have PH interventions (30.3% vs 69.7%, P = 0.004). In contrast, in a retrospective study including 2 Level 1 trauma centers, Radulovic et al found that the odds of return of spontaneous circulation were lower in penetrating trauma in the presence of any PH intubation attempt (OR = 0.39, 95% CI 0.19-0.82, P = 0.01). 14 These findings stand in distinction to our own observations, where we noted improved likelihood of ongoing resuscitation for patients who had already undergone PH interventions. It is perhaps true that Radulovic and colleagues’ observations of the negative association between PH intubation and survival among penetrating trauma patients was due to PH personnel focusing on intubation instead of other RE such as IO access or decompression of the chest. It is also difficult to compare PH interventions across catchment areas given the vagaries of guidelines, protocol, and transfer times among different PH provider groups.
Currently there is no standardized protocol for PH interventions for patients with TFA. A standardized set of guidelines could help determine which patients should be transported which could then mitigate hospital costs and consumption of resources and even limit the exposure of health care professionals to occupational health hazards.15,16 In our own study, we demonstrated that patients who went on to receive additional interventions by hospital personnel were more likely to have undergone additional RE by PH personnel. This finding suggest that PH providers use their clinical judgment to determine which patients will benefit from additional interventions, which lends credence to the idea that there are patients who can be better triaged in the field to forego transfer to a trauma center given that for some patients, the only intervention that they will undergo is transport.
Given the long odds for patients who undergo RT, the decision-making surrounding this procedure can be complex and is often based on incomplete data for the treating clinician. Survival following RT has been associated with <65 years of age, absence of CPA, ISS <16, and penetrating injuries. 17 These findings coincide with our findings of RT being more commonly performed in patients following penetrating vs blunt injuries (152 (66.9%) vs 75 (33.0%), P < 0.001). It is important to note that the decision to proceed with RT or further RE in our hospital is ultimately decided by the clinician receiving these patients and making decisions based on clinical experience. Even though this has been extensively studied, the bulk of existing literature has addressed physiologic or time-based variables. No current national guidelines that guide the use of RT speak to PH variables explicitly, and therefore, this represents a current gap in the published literature. Given the lack of consensus surrounding PH variables, further research is needed to better delineate which patients are most likely to benefit from PH resuscitation and transport to the nearest trauma center.
The limitations to this study include those inherent to a single-center retrospective cohort analysis, thus leading to the inability to determine association rather than causation from events. There may have been missed patients due to misclassification, selection, and reporting bias during this time span. Notably, this study does not include patients who died without transport to the hospital, which limits our analysis of all patients with PH arrest to only those transported to our trauma center. Our data is also skewed geographically as most of the patients in this study are coming from South Los Angeles, which is an area with high crime and violence and could be a limitation as this may not be applicable to the greater United States population. 18 Furthermore, the data did not include information regarding social determinants of health such as neighborhood location or exposure to previous episodes of violence, which may have increased the incidence of penetrating trauma and may make our sample less representative of other trauma systems. Another limitation to our cohort is that PH personnel transport a patient from the scene solely due to safety concerns and would therefore represent a patient transported but deemed unlikely to survive or already declared deceased by PH personnel. Our cohort excluded these types of patients precisely for this reason, but our ability to definitively understand the thought process by our PH colleagues is limited to what is documented in the medical record and PH records.
Conclusions
More than 25% of transported patients following TFA have an immediate termination of resuscitative efforts once they arrive to the hospital. Our study shows that patients with blunt MOI, older age, and those who undergo fewer PH interventions are less likely to receive further RE in the ED. Patients who were DOA/ITRA spent less time in the ED, especially for patients with penetrating injuries. Our results indicate that there are likely a set of PH variables that may better inform decisions surrounding transfer of patients with PH arrest, most especially older patients with blunt MOI. Future research efforts could include a multi-center examination of these patients to further delineate which patients are unlikely to benefit from PH transport with a focus on the development of a framework for establishing PH variables predictive of poor outcome and as a means of strengthening field guidelines for termination of resuscitation prior to hospital transport.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.