
Abstract
Purpose
Bomb blast injuries in non-combat settings have seen a surge in the last two to three decades. Third-world countries like Pakistan have been at the receiving end of these attacks. However, the extent of the damage inflicted in these regions is not fully understood due to gross underreporting. We aim to assist radiologists in identifying common abdominopelvic injuries in bomb blast victims and highlighting specific injury patterns to guide more effective management.
Methods
This was a retrospective observational study designed to analyze abdominopelvic injuries among bomb blast victims treated at our institution. Data were retrieved from the hospital’s electronic health records and included demographic information (age and sex), injury classification, imaging results, treatment received, and clinical outcomes.
Results
Chi-square and t-tests showed no statistically significant difference in the gender or mean age distribution between patients who underwent abdominopelvic surgery and those who did not. The most common single injury category among the patients analyzed was secondary injury, while the most common combination of injuries observed was a combination of secondary and tertiary injuries. CT was the most frequently requested first-line radiological investigation, while US was most frequently requested as a second-line modality. Injuries to the liver were the most frequently observed solid-organ injury.
Conclusion
Efficient practices are essential in radiology departments to manage the surge in patient numbers seen after bomb blast incidents. Our study emphasizes the role of radiology scans and details the types of abdominopelvic injury patterns observed in bomb blast victims.
Introduction
Over the last few decades, bomb blast injuries in non-combat settings have become increasingly common as acts of terrorism. While bombings in first-world countries and major cities garner global attention, third-world countries like Pakistan often experience similar issues more frequently that go unnoticed. The unexpected nature of these target attacks on urban areas results in high-risk disasters that have high rates of morbidity and mortality. 1 While it is difficult to estimate the extent of damage in Pakistan due to gross underreporting, some studies have shown that victims are mostly males with ages ranging between 15 and 45.2,3
Due to the influx of casualties that overwhelm emergency departments (EDs) following bomb blasts, radiologists can quickly become as burdened as ED physicians because of the extensive yet necessary use of radiologic scans. The American Association for the Surgery of Trauma (AAST) has defined low- and high-grade visceral injuries as those that do not require surgical management and those that require surgery, respectively. 9
Our study aims to assist radiologists in identifying common abdominopelvic injuries in bomb blast victims and highlighting specific injury patterns to guide more effective management.
Methods
Study Design
This study employed a retrospective observational design to analyze abdominopelvic injuries among bomb blast victims treated at our institution. The study was approved by the Institutional Review Board of the Aga Khan University Hospital, Karachi, and informed consent was waived due to the study’s retrospective nature.
Study Population
The study population included all patients who presented to our facility with bomb blast injuries. Patients were included if they had documented abdominopelvic injuries confirmed by radiologic imaging (ultrasound, CT scan, or MRI). Exclusion criteria encompassed individuals with incomplete medical records, those transferred from other institutions without relevant imaging, and patients who did not survive long enough for imaging.
Data Collection
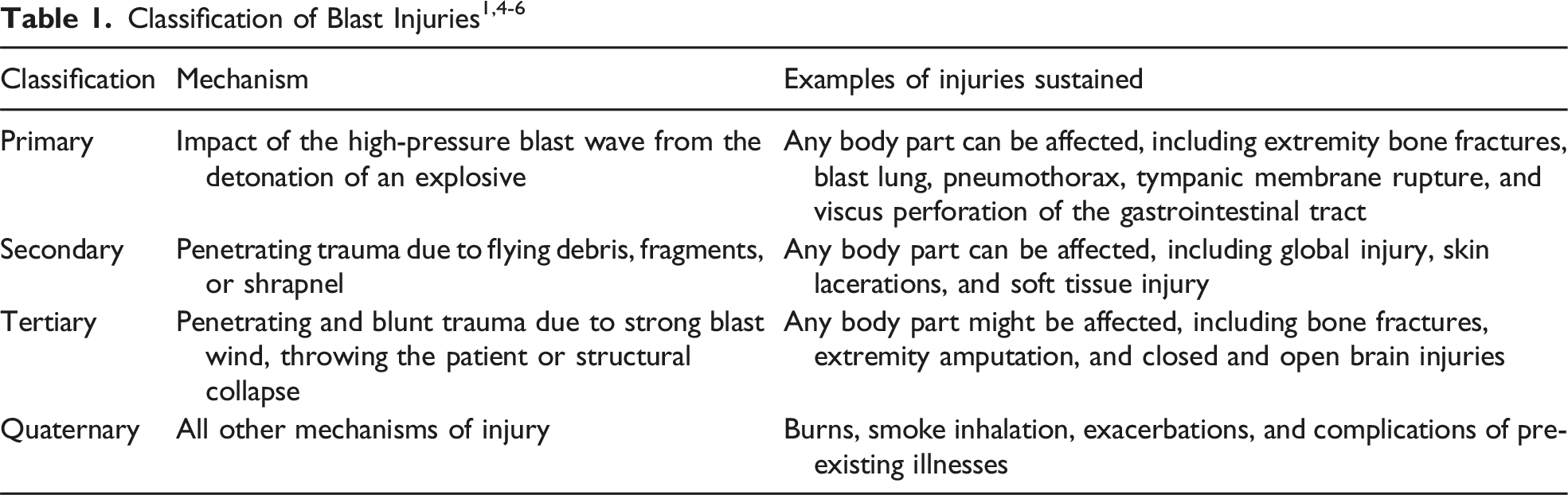
Data were retrieved from the hospital’s electronic health records and included demographic information (age and sex), injury classification, imaging results, treatment received, and clinical outcomes. Clinical parameters such as systolic and diastolic blood pressure and pulse rates were also examined to correlate physiological responses with injury severity. The demographic data of the patients involved in the study were analyzed to understand the distribution across different age groups and genders. Injury classifications were based on the established categories of bomb blast injuries: primary, secondary, tertiary, and quaternary. Specific attention was given to abdominopelvic injuries, categorized according to the type of injury sustained (eg, solid organ injuries, vascular injuries, and bowel perforations).
Statistical Analysis
Descriptive statistics were employed to summarize demographic data and injury characteristics. Categorical variables were expressed as frequencies and percentages, while continuous variables were reported as means and standard deviations. Statistical comparisons between different age groups and injury types were performed using chi-square and independent t-tests for categorical variables, with a significance level set at P < .05. All analyses were conducted using SPSS.
Results
Gender Distribution
The gender distribution between the two groups, those who underwent abdominopelvic surgery and those who did not, was analyzed using a Chi-square test. The test yielded a P-value of 0.529, indicating no statistically significant difference in the gender distribution between the two groups. Most patients in both groups were male, with a small number of female patients.
Age Distribution
The age distribution was compared between the surgery and no-surgery groups using an independent t-test. The mean age for patients who underwent surgery was 29.35 years (SD = 11.65), while the mean age for those who did not undergo surgery was 29.58 years (SD = 12.32). The t-test yielded a P-value of .919, suggesting no significant difference in the mean age between the two groups.
Injury Classification
Most of the patients had a combination of different injury categories (Figure 1 and Table 2). The most common single injury category among the patients analyzed was secondary injury, affecting 43 patients. This was followed by a combination of secondary and tertiary injuries, which were observed in 34 patients. Injuries that could not be characterized were noted in 27 patients, highlighting the complexity or ambiguity of certain cases. Tertiary injuries alone were identified in 16 patients. Distribution of Injury Classification Distribution of Injury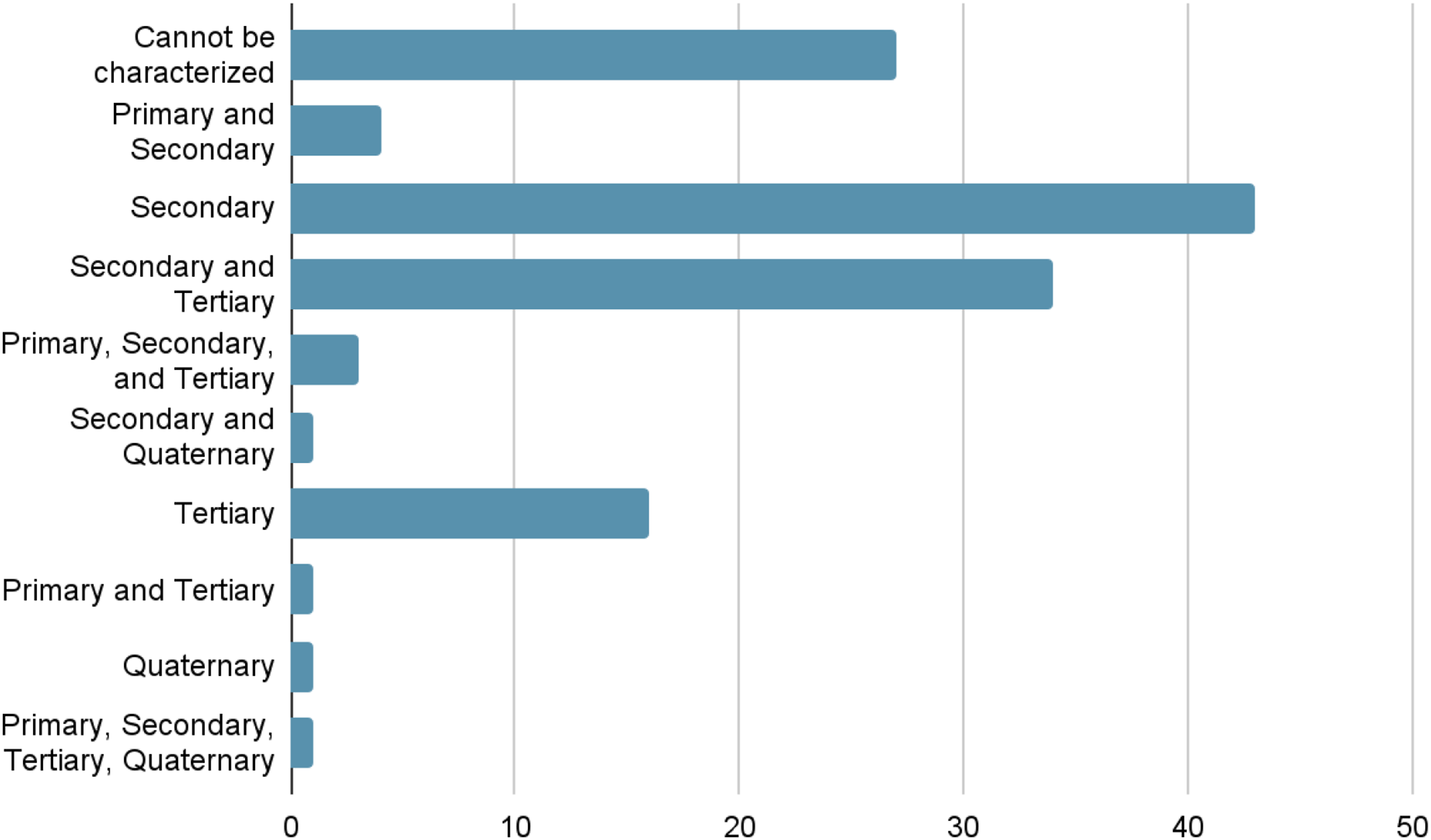
Primary and secondary injuries were combined in four patients, while three patients sustained a combination of primary, secondary, and tertiary injuries. Secondary and quaternary injuries were observed together in one patient, as were primary and tertiary injuries. Quaternary injuries alone were rare, affecting just one patient. Additionally, a single patient was found to have sustained injuries across all four categories—primary, secondary, tertiary, and quaternary.
Radiological Investigations
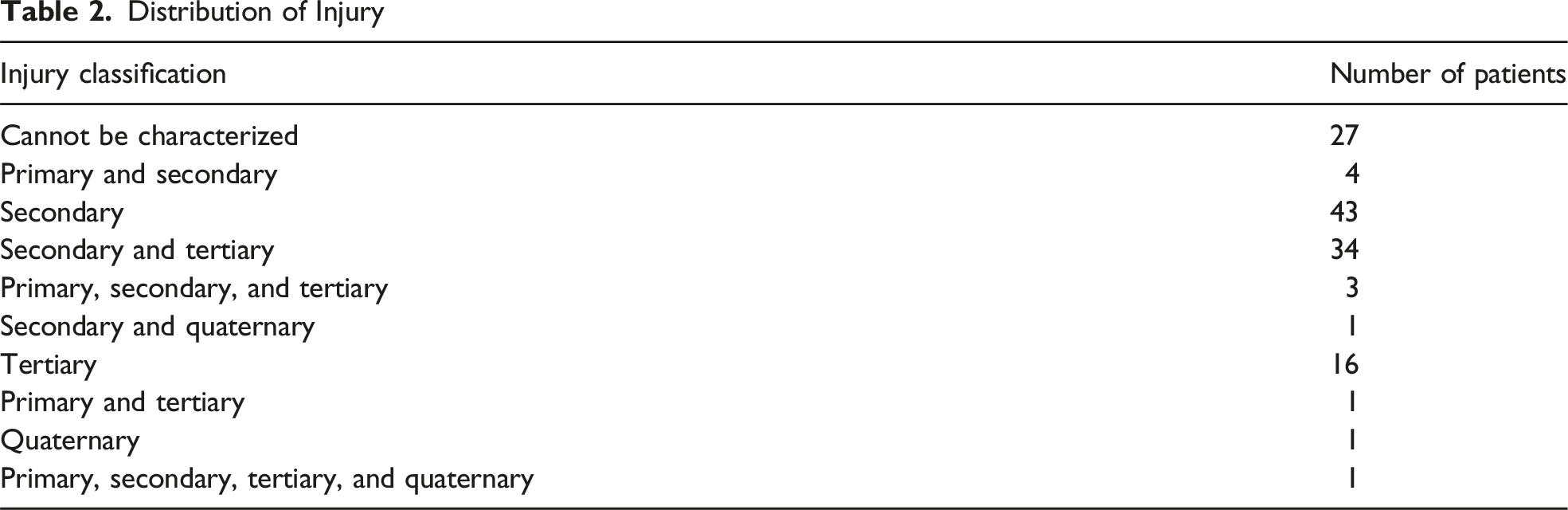
The most common first investigation for abdominopelvic injuries in bomb blast victims was a CT scan, with a total of 62 scans performed (Figure 2 and Table 3). Ultrasound (US) was the second most common first-line imaging modality, with 53 scans conducted. Plain radiography (XR) followed, with 26 initial scans, while conventional angiography and fluoroscopy were each utilized four times as the first imaging modality. Nuclear scans were the least frequently used as an initial investigation, with only one scan performed. Distribution of Modalities Used as First-line Radiological Investigations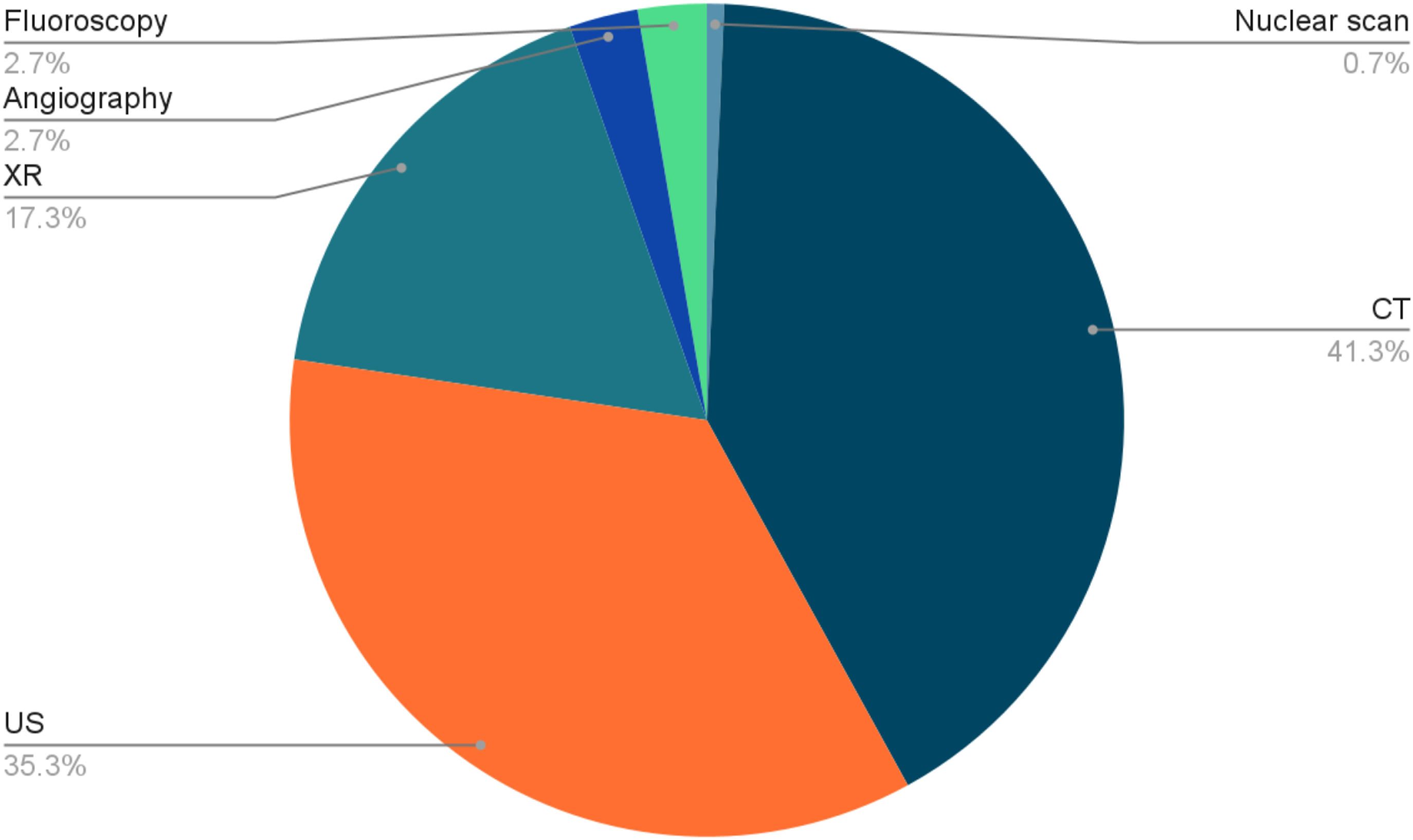
For subsequent investigations (Figure 3 and Table 3), ultrasound was the most frequently repeated imaging modality, with 33 scans conducted. CT scans were the second most common follow-up imaging, with 25 scans performed. Plain radiography (XR) was used 27 times in follow-up, fluoroscopy was utilized in eight cases, and conventional angiography and nuclear scans were each repeated once.
The most common finding on the first radiological scan was a normal scan, observed in 73 cases (Figure 4 and Table 4). This was followed by the detection of hemoperitoneum in 20 cases and pneumoperitoneum in 14 cases. Postsurgical findings and liver injuries were identified in eight cases each, while intra-abdominal collections were also noted in eight cases. Abdominal wall injuries and splenic injuries were each found in seven cases, and bowel perforation was observed in five cases. Less common findings included testicular injury (four cases), kidney injury (three cases), pseudoaneurysm (three cases), and urethral injury (one case). Adrenal injury and diaphragmatic injury were the least common, with only one case each.
In the second radiological investigation, the most common finding was again a normal scan, seen in 50 cases (Figure 4 and Table 4). Hemoperitoneum was detected in 10 cases, making it the second most frequent finding. Liver injury and splenic injury were both noted in four cases, while testicular injury, which had been detected in four cases initially, was also found in four cases during the second scan. Pneumoperitoneum and intra-abdominal collections were each identified in two cases. Bowel perforation was observed in two cases on the second scan. Kidney injury, pseudoaneurysm, and adrenal injury were all detected in one case each. Notably, urethral injury, initially identified in one case, was found in three cases on the second scan, indicating potential progression or new findings. The diaphragmatic injury was not observed in any second scan.
Low-grade visceral injuries were more common compared to high-grade injuries (as defined by AAST) in both the first and second investigations (Figure 5).
Need for Surgical Intervention
Out of the total 160 patients, 37 (23.1%) underwent abdominopelvic surgery, while the remaining 123 patients (76.9%) did not (Figure 6 and Table 5). This indicates that a minority of the patients in this cohort required surgical intervention.
Hospital Stay Duration
The duration of hospital stay was significantly different between the two groups. Patients who underwent abdominopelvic surgery had a mean hospital stay of 11.81 days (SD = 9.56), while those who did not have surgery had a mean stay of 7.96 days (SD = 9.93). The independent t-test yielded a P-value of .047, indicating a statistically significant difference in hospital stay duration between the two groups. This suggests that abdominopelvic surgery is associated with a longer hospital stay.
Discussion
Bomb blasts are among the most devastating forms of violence, causing extensive casualties and severe injuries. These acts of terrorism are often designed to inflict maximum harm on individuals and cause widespread destruction. A meta-analysis from 1970 to 2014 included 58 095 terrorist explosions worldwide and found the mean casualty statistics per incident to be 1.14 deaths and 3.45 wounded from non-suicide incidents, and 10.16 and 24.16 from suicide bombings (P < .05). 10 In Pakistan, densely populated cities are frequent targets for bomb blasts, and because these cities are larger, they receive more extensive reporting and analysis. Between 2007 and 2011, Karachi, a densely populated city with over 20 million residents, experienced 46 explosion incidents according to a study. 3 These events resulted in 249 fatalities and 893 injuries. The leading cause of death was shock from multiple injuries, accounting for 62.65% of fatalities. An additional study reveals that based on newspaper reports and online databases, 63 bomb blasts took place in Karachi from January 2000 to October 2007, with a mean of 7.8 ± 7.1 blast incidents per year. They resulted in 1592 casualties, 21% of whom were immediate deaths, and 79% were survivors who were shifted to hospitals. 11 Another study describes a total of 103 patients with bomb blast injuries who presented to seven selected EDs in Pakistan from November 2010 to March 2011. Most of the victims presented in Peshawar (n = 41, 39.8%) and Karachi (n = 31, 30.1%). 2 Furthermore, a three-year study in a hospital in Rawalpindi, Pakistan, found 1296 terrorist victims presented to the emergency department and (86.9%) were admitted, with a mean hospital stay of 8.2 ± 2.1 days. 8
Various studies in Pakistan have consistently shown that young males are the most common victims of bomb blasts. One five-year study found that out of 1142 cases, only 55 (4.82%) were female, while 1087 (95.18%) were male, with ages ranging from 15 to 45 years. 3 An additional study highlights a similar trend in which all victims were male, and the majority of victims were between 16 and 45 years of age. 12 A different study reported a higher percentage of female victims, around 25% with a median victim age of 30 years, 2 while yet another indicated that only 2% 26 of the cases were female, with a mean victim age of 33.2 years. 8 This variation suggests that the percentage of female victims depends on the area affected, although young males remain predominantly affected. Our study supported these findings, with only 10 out of 160 patients (6.25%) being female and a mean age of around 30 years. A possible explanation for this is that terrorists often target large gatherings that culturally, women tend to avoid, and hence, young males become the primary victims. Other cities, such as Beirut and Paris, where fewer of these cultural norms exist, had more equal gender distribution (around 60% and 55%, respectively) and higher median age (around 47 and 37, respectively).13,14
Bomb blasts affect patients through multiple mechanisms that are evident by the wide variety of injuries affecting multiple body regions and organ systems. 15 Patterns of these injuries depend on several factors, including the environment of the blast (if it is in a closed or open space), the number of shrapnel expelled, and the nature of the explosive material. 16 The resulting polytraumatic injury pattern makes it difficult to classify a blast injury and apply conventional injury scoring systems in clinical practice. For example, an explosion can cause complex injury patterns in a single patient that may be described as both blunt and penetrating and occur through multiple injury mechanisms.5,17 Our study yielded similar results, with 44 out of the 104 patients who could be classified into a specific injury pattern exhibiting multiple categories of injuries, and one patient presenting with all four categories of injury.
Research has demonstrated that the high pressure linked to blast injuries frequently results in blast lung and tympanic membrane injuries.18,19 Extremity-related wounds are also quite prevalent. A meta-analysis spanning 40 years found that these injuries were the most common, involving 32% of all cases. 9 Another study conducted in Somalia reported that 101 patients (57.7%) sustained extremity injuries, and among them, 76 (75.2%) had at least one fracture. 20 Head injuries are also common, with severe head trauma being one of the leading causes of fatalities among blast victims.7,21 The gastrointestinal (GI) tract is vulnerable to injury due to its heterogeneous density and gas-containing structures. A study comparing intra-abdominal injuries across various types of traumas found that bowel injuries occurred in 71.4% of blast victims, 64.4% of gunshot victims, and 25.3% of blunt trauma victims (P < .001). The study also noted that penetrating shrapnel (secondary injury) was responsible for bowel injuries in all but one patient (94.4%) in the blast group. 22 Solid organ injuries caused by secondary and tertiary blast mechanisms are typical clinical problems, but the powerful forces from primary mechanisms can also lead to lacerations of solid abdominal viscera.23,24 In our study, bowel perforation was relatively rare, occurring in only five patients. While a larger number of patients had solid organ injuries, the incidence was still lower than expected based on the literature. This discrepancy may be attributed to the diverse blast environments encountered in Pakistan. However, the literature suggests that abdominal injuries may present later and might not be detected during the initial emergency room triage. A study reported that a patient, who had been discharged from the ED in stable condition following a mass casualty incident, returned the next day with abdominal pain, tenderness, and guarding. Upon examination, it was discovered that 75% of the lumen of a segment of the distal jejunum was perforated. 25 Abdominal hematomas can also be challenging to detect due to their delayed development, making them easy to miss. 24 Hence, it is suggested that patients with pain, tenderness, or other possible signs of abdominal injury should be observed for at least 48-72 hours regardless of the results of any diagnostic examination, and all victims of blast injuries should be vigilant of any developing symptoms. 26
Radiologists are crucial in mass casualty incidents like bomb blasts due to the complex injury patterns involved. During the 2004 Madrid bombings, focused abdominal sonography for trauma (FAST) was conducted on 63 patients in the initial hours. By the end of the day, 75 helical CT scans and one MRI scan had been completed. Additionally, three vascular interventional radiology procedures (embolization) were performed to address intercostal artery, hepatic, and hepatosplenic bleeding. 27 The presence of abundant metallic shrapnel often limits the use of MRI; however, identifying shrapnel locations, their fragments, and resulting injuries is pivotal. Occasionally, a shrapnel fragment may be concealed or challenging to detect through a small entry wound. Therefore, even victims with seemingly minor injuries may require radiological evaluations. 28 Shrapnel detected on plain abdominal and pelvic radiographs can be further assessed for peritoneal penetration and visceral injuries through CT studies to prevent unnecessary surgical interventions. CT is the definitive method for evaluating abdominal penetration and shrapnel-related injuries and is essential for triaging surgery in hemodynamically stable patients. Understanding whether shrapnel has not penetrated the peritoneum (as indicated by imaging) is valuable in avoiding unnecessary laparotomy in victims of low-powered explosions. 29 Our study mirrored these findings, with CT scans being the most frequently used initial investigation for abdominopelvic injuries in bomb blast victims, totaling 62 scans. US was the second most common first-line imaging modality, with 53 scans conducted. Plain radiography (XR) followed, with 26 initial scans, and nuclear scans were used the least. No MRIs were conducted as an initial imaging modality.
Following a bomb blast, it is crucial to manage the hospital’s high volume of patients while maintaining a delicate balance between thorough assessment and the judicious use of limited resources. Ensuring that scans are performed efficiently helps prevent the radiology department from disrupting the overall flow of patient care. Hare et al recommended the mass casualty plan roles for the radiology department in case of bombings and other possible mass casualty incidents
6
: 1. All elective and non-urgent patients are cleared from the hospital, in particular from the emergency department and radiology. Both clinical and non-clinical staff are allocated to key areas of the radiology and emergency department. 2. The role of radiology involves bedside radiography and FAST in the emergency department, as well as plain radiography and fluoroscopy in the X-ray department and theater and CT of some patients. A radiologist should be stationed in the major trauma bays to perform FAST to exclude free abdominal fluid or hemodynamically significant abdominal injury. Radiologists are also stationed in the emergency department, immediately reporting all plain radiographs and communicating with the supervising clinicians, with a similar set-up in CT. As for the entire hospital, plans for further backup staff should be in place if there is a prolonged event. 3. All critically ill patients require a chest, cervical spine, and pelvis view as routine, as well as plain films based on the site of penetrating wounds, as these can cause complex internal injuries. 4. Unstable patients should be transferred straight to the operating room for exploratory laparotomy/thoracotomy or other operative procedures to treat the cause of hemodynamic instability. 5. Stable but critically ill patients can be transferred to CT before surgery. The scout view should cover the entire body (to look for shrapnel and undetected fractures) and be followed by CT of the head, chest, and pelvis.
Conclusion
Following a bomb blast, hospitals experience a substantial increase in patient numbers, necessitating the effective use of radiology services. Efficient practices are essential in radiology departments to manage this surge. Additionally, radiologists must be familiar with common injury patterns and potential injuries. Our study emphasizes the role of radiology scans and details the types of injury patterns observed. A limitation of our study is the lack of data on patients who succumbed either en route to the hospital or at the site of the explosion, which may affect the overall representation of injury severity. Despite these constraints, it is noteworthy that our findings reveal a surprisingly high number of normal scans, especially since as a tertiary care hospital, we often receive complex cases that are referred to us from other hospitals. This observation is particularly intriguing given the diverse range of injuries studied across multiple bomb blasts, occurring in both enclosed and open environments with various mechanisms of injury. The relatively low incidence of high-grade injuries in our study highlights the complex nature of abdominopelvic trauma and underscores the need for continued research to better understand the full spectrum of bomb blast injuries.
Supplemental Material
Supplemental Material - Approach and Management of Multiple Victims of Civilian Bombing Events With Abdominopelvic Injuries: A 20-Year Institutional Experience in Pakistan
Supplemental Material for Approach and Management of Multiple Victims of Civilian Bombing Events With Abdominopelvic Injuries: A 20-Year Institutional Experience in Pakistan by Muhammad Nadeem Ahmad, Zahra Fatima Rahmatullah, Muhammad Masood Alam, Fatima Bhojani, Mallick Muhammad Zohaib Uddin, Shahzeb Ali, Naila Nadeem, Muhammad Salman Khan, and Uffan Zafar in The American Surgeon
Footnotes
Author Note
This article submission has been presented as an oral paper presentation at the 110th Scientific Assembly and Annual Meeting of the Radiological Society of North America, held December 1-5, 2024 in Chicago, Illinois.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.